Successful restoration of partially edentulous situations, especially kennedy’s class-I, II &IV requires lot of contemporary and conventional treatment approaches. Semi precision attachments play a major role in retention of clinically challenging partially edentulous situation. Attachment retained partial dentures can be one of the successful treatment option in prosthdontics. This article presents a unique technique of retaining gum stripper using semi precision attachments.
Gum stripper, Kennedy’s class-IV, Precision attachment, Rheine83
Case Report
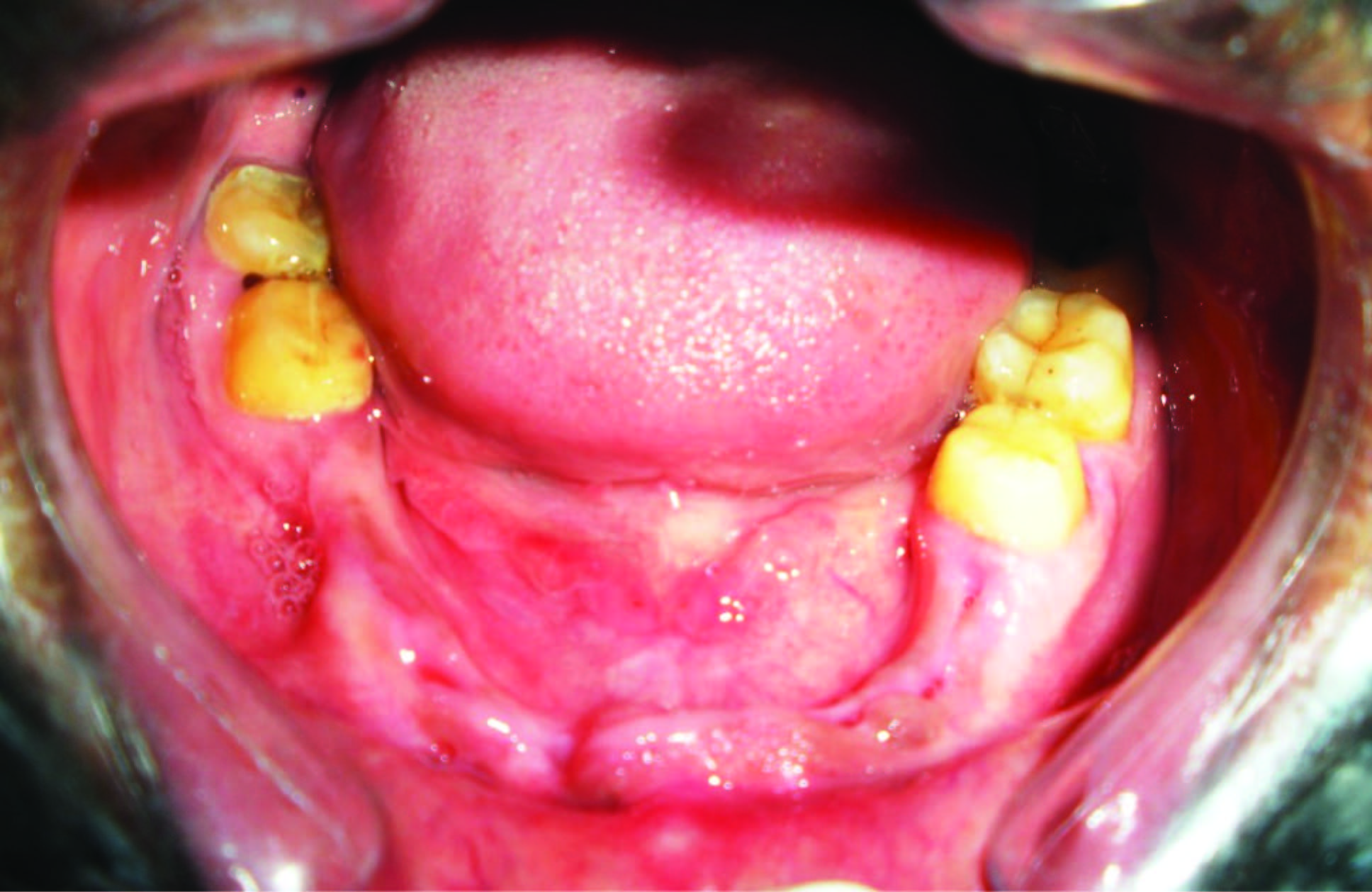
A 36-year-old male patient referred to Department of Prosthdontics. Bapuji dental college and hospital, Davangere, India, for opinion regarding rehabilitation of bilaterally missing mandibular anteriors and bicuspids. The reason for tooth loss was trauma. He gave a history of unsatisfactory acrylic partial denture. Patient had decreased lip support in anterior mandibular region. On intraoral examination, it was noted that the patient had fully dentate maxillary arch and missing 31,32,33,34,35, and 41,42,43,44,45,46 (Kennedy’s class IV) in mandibular arch. The remaining teeth in mandible arch were periodontally sound [Table/Fig-1]. Intra oral peri-apical radiographs in relation to 47, 48, 36, and 37 showed intact lamina dura, minimal bone loss and no peri apical pathology.
Mandibular arch showing kennedy’s class IV
Treatment options for such condition would be:
Conventional treatment partial denture
Conventional cast partial denture
Overlay denture
Implant supported fixed partial denture
Attachment supported cast partial denture
Attachment supported treatment partial denture.
Considering the pros and cons of each treatment option, attachment supported treatment partial denture offered following advantages.
Better retention even in severely resorbed ridges,
Aesthetics,
No surgical intervention, no post-op sensitivity,
Economical and
No elective endodontic therapy.
All RPD with attachments, especially the extracoronal type, are considered more efficient in providing retention and restoring function and aesthetics [1,2].
After complete clinical examination, a prosthetic treatment plan was set up. Prosthesis with extracoronal precision attachment was planned for Kennedy’s class IV condition in mandibular arch. Tooth preparation i.r.t. 36, and 47 abutment teeth was performed to receive full coverage metallic crowns. The abutments prepared were temporized after making definitive impression with addition silicone elastomeric impression material (aquasil, 3M ESPE). Putty reline impression technique was used.
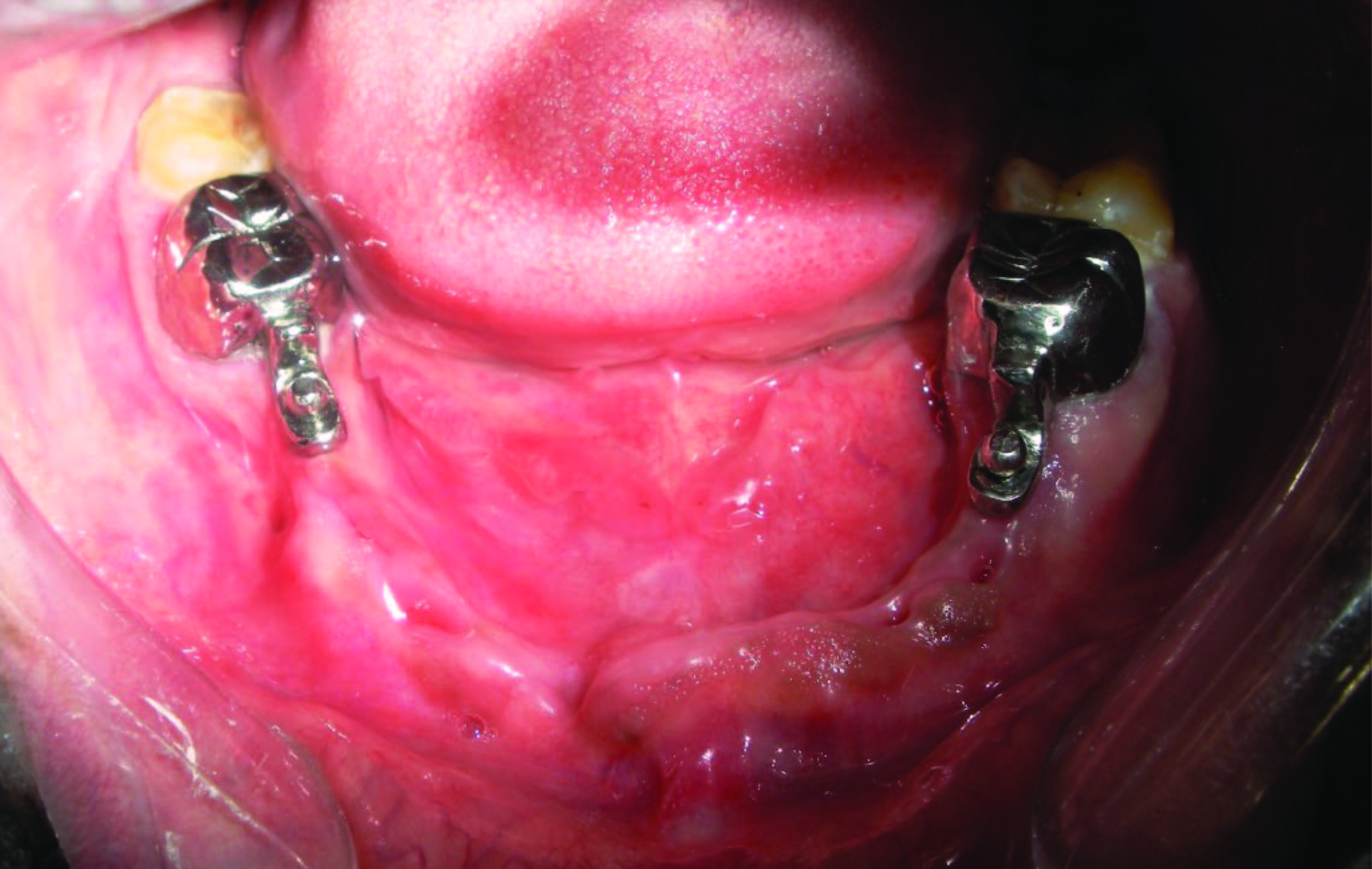
Cast was poured in type IV gypsum product (Ultrarock- kalabhai). Wax-up of 36 and 47 was done to receive full metal crown. Patrix parts of the semi precision attachments (OT CAP Rhein83 Inc. USA) were attached to the mesial side of wax patterns of both 36&47. And their parallelism was checked with the help of a dental surveyor. After casting of wax pattern along with castable parts of rhein83, it was tried in the patient mouth. Full metal crowns along with attachments were cemented using glass ionomer luting cement (GC FUGI 1, GC Corporation. TOKYO. JAPAN) [Table/Fig-2]. Now treatment partial denture is tried in wax-up stage to evaluate space for attachments, denture stability, support, esthetics, occlusion and speech. Patient's consent was taken before acrylization of the trial denture. It was cured in heat cure acrylic resin (Travelon, Dentsply limited, Addlestone, UK),
Final cementation of full metal crown along with attachment in 47 & 36
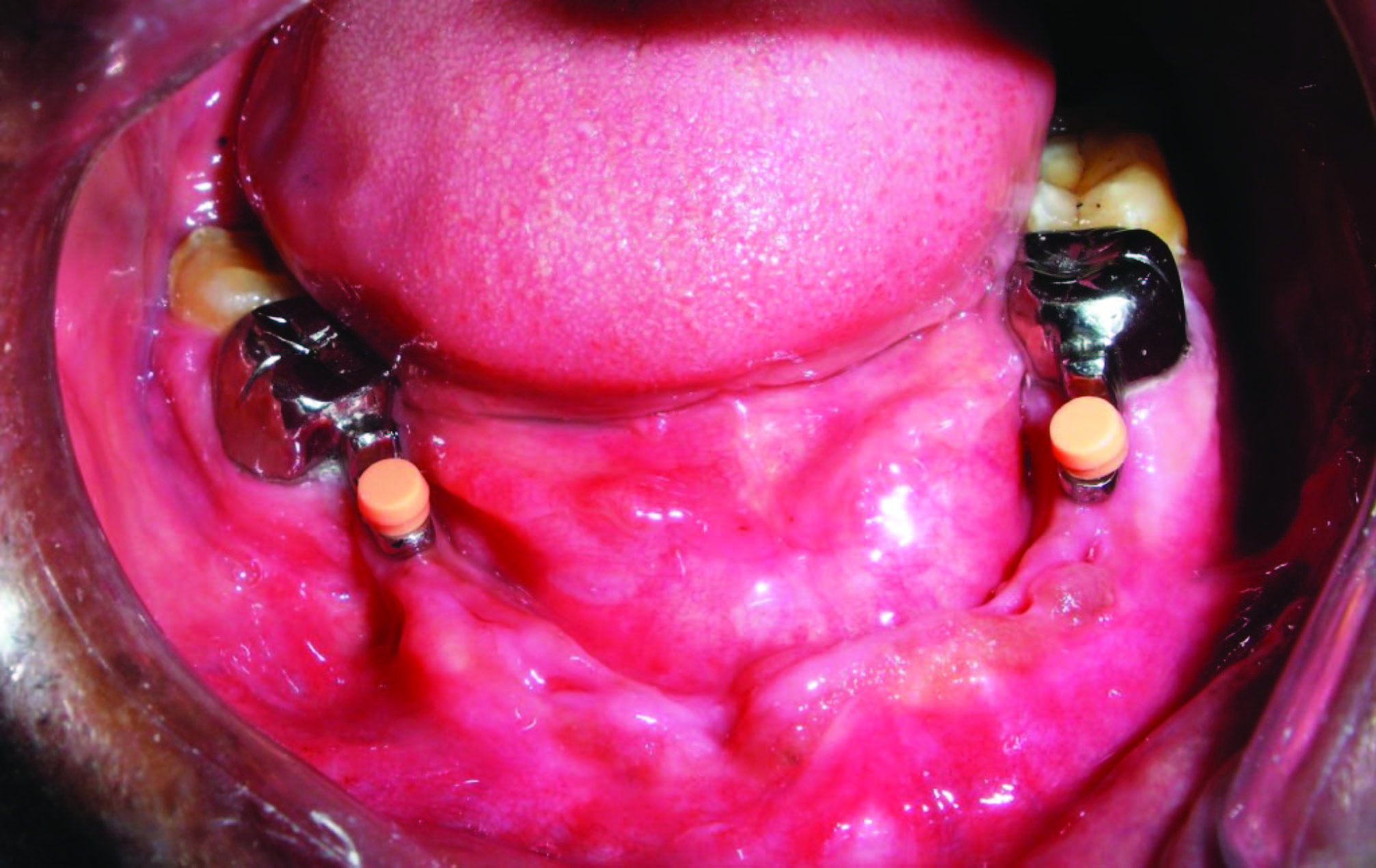
Trial seating of the finished prosthesis was performed. retentive caps were placed on top of ball attachments [Table/Fig-3]. These retentive caps were picked up within the partial denture with the help of self cure acrylic resin (DPI, cold cure) [Table/Fig-4]. After the final insertion [Table/Fig-5&6] routine oral hygiene instructions were given.
Full metal crown along with retentive resilient cap in 47&36
Retentive caps picked up within partial denture

Final insertion of Prostheses

Intra oral view of final prosthesis in occlusion

Patient was recalled after 24 h, 1 wk and 3 mnth for recall checkup to evaluate the tissues for any irritation, trauma and occlusal prematurities. Prognosis of the treatment seems to be satisfactory.
Discussion
Despite the fact that FPD is better tolerated by the patients in comparison to RPD, the later is still prevalent in partially dentate people [3]. Attachments can contribute to stress concentration with Kennedy class I, class II and class IV RPDs. Which can be overcome by different methods of controlling stress include splinted abutments, stability of the denture base, rigid design of the prosthesis, broad denture base coverage, occlusal harmony, loading techniques, and shimming [4].
Generally retention of RPD is obtained from clasp, telescopes, or some form of attachments. An intact caries-free tooth intended as a retentive abutment is best provided with a clasp or adhesive attachments [5]. Though survival rate of vital tooth as telescopic abutment in retaining Removable dental prostheses is 89%, root canal treatment increases the risk factor of abutment loss [6] and the visible component of clasp jeopardizes the aesthetics [7]. A few retrospective studies regarding survival of attachments retained partial denture show 83.3% for 5 y, 67.3% up to 15 y and of 50% when extrapolated to 20 y [8,9]. Hence, Removable dental Prostheses fabricated with precision/semi precision attachments for retention and support are the best prosthesis available to dentistry where fixed restorations are contraindicated [10].
One of the recent case report suggest oral rehabilitation using an FPD/RPD with attachments is one of the most conservative and best indicated therapeutic modalities considering the limiting bone condition and the extension of the prosthetic space [11].
Precision attachments are wholly or partially machined accessories used for retention of removable prosthesis. Towards the end of the 19th century Parr, Peeso, Chayes, and other experts designed gadgets which were subsequently called as precision attachments. These devices allowed prostheses to combine the advantages of both fixed and of removable restorations [12]. Precision attachments have been constructed into two halves, a matrix and a patrix, the halves being so arranged that they articulate with one another to form a precise but separable joint. Precision attachments are available as prefabricated and resin patterns. Resin patterns can be customised to the space available without affecting aesthetics and function [13]. There are numerous attachments available. Among them Rhein 83 system are simple and offer spherical retention. The versatality of applications to many restoration solutions offered by the spherical retention is widely recognized in the treatment of the partially edentate and totally edentate patients [14]. These attachments are designed to be placed intracoronally or extracoronally. All RPD with attachments, especially the extracoronal type, are considered more efficient in providing retention and restoring function and aesthetics [2].
Selections of retainer for removable dental prosthesis mainly depends on the remaining tooth structure, the intra and inter maxillary relationships, aesthetics, and financial aspects [15]. They serve the same purpose as that of the clasps, i.e., to retain and attach a fixed partial denture or partial denture to natural teeth [16] and has disadvantage of more tooth reduction and at least 3 mm of vertical height above the crest of ridge [16].
Attachment used in this case was Rhein83 OT CAP Inc. USA [Table/Fig-7]. It is an extracoronal castable attachment positioned on the distal of the crowns as an extension allowing vertical space for optimal aesthetics. The castable OT male CAP can be easily shaped with the crowns during wax-up stage. Precision attachment offers considerable advantages in dentistry because of their flexibility. It is a well known fact that the movement of RPD transmits force to the distal most abutment. To minimize the stress on distal abutment we have followed the philosophies of impression making of distal extension situation [17] and by using semi precision attachment which will act as a tress breaker.
The RHEIN 83 OT CAP attachments system

A survey on design of RPD in dental laboratories of Greece has shown 50% of RPDs fabricated were retained by precision attachments [18]. A study regarding analysis of retention and wear of ball attachments has shown the material combination of a precious gold alloy matrix and a titanium ball seems to be favourable for long-term retention [19]. Finally, in addition to taking the biomechanical aspects into consideration, periodic follow-up is essential to avoid damage to the support structures and guarantee adequate long-term function and aesthetics [20].
Conclusion
Removable partial dentures are the treatment of choice in rehabilitation of long span anterior edentulous space. Dental implants can be used in such situations to go for fixed treatment options. Considering the economical factors and surgical risk, semi precision attachments can be effectively used to improve patient comfort, aesthetics and retention in removable partial dentures. Retention of these attachments can be monitored and upgraded during follow up visits just by replacing retentive caps within the dentures.
[1]. Awang RAR, Arief EM, Hassan A, Spring loaded plunger attachment for retention of removable partial denture: a case reportArch Orofac Sci 2008 3:32-35. [Google Scholar]
[2]. Chikunov I, Doan P, Vahidi F, Implant-retained partial overdenture with resilient attachmentsJ Prosthodont 2008 17(2):141-8. [Google Scholar]
[3]. Zitzmann NU, Hagmann E, Weiger R, What is the prevalence of various types of prosthetic dental restorations in Europe?Clin Oral Implants Res 2007 18(Suppl 3):20-33. [Google Scholar]
[4]. Lee K, Double impression procedure for removable partial denture retained with semiprecision attachments: a clinical reportJ Prosthet Dent 1996 75(6):583-87. [Google Scholar]
[5]. Zitzmann NU, Rohner U, Weiger R, Krastl G, When to choose which retention element to use for removable dental prosthesesInt J Prosthodont 2009 22:161-67. [Google Scholar]
[6]. Dittmann B, Rammelsberg P, Survival of abutment teeth used for telescopic abutment retainer in removable partial denturesInt J Prosthodont 2008 21:319-21. [Google Scholar]
[7]. Ku Y, Shen Y, Chan C, Extracoronal resilient attachments in distal-extension removable partial denturesQuintessence Int 2000 31:311-17. [Google Scholar]
[8]. Burns DR, Ward JE, A review of attachments for removable partial denture design: part 1. Classification and selectionInt J Prosthodont 1990 3:98-102. [Google Scholar]
[9]. Burns DR, Ward JE, A review of attachments for removable partial denture design: part 2. Treatment planning and attachment selectionInt J Prosthodont 1990 3:169-74. [Google Scholar]
[10]. Feinberg E, Feinberg EM, Attachment-retained partial denturesN Y State Dent J 1984 50:161-64. [Google Scholar]
[11]. dos Santos Nunes Reis JM1, da Cruz Perez LE, Alfenas BF, de Oliveira Abi-Rached F, Filho JN, Maxillary rehabilitation using fixed and removable partial dentures with attachments: a clinical reportJ Prosthodont 2014 23(1):58-63. [Google Scholar]
[12]. Preiskel HW, Precision attachment for the partially dentate mouthAnn R Coll Surg Engl 1974 75:294-98. [Google Scholar]
[13]. Shetty NB, Shetty S E N, Shetty O, D'souza R, Precision attachments for aesthetics and function: a case reportJ Clin Diagn Res 2014 8(1):268-70. [Google Scholar]
[14]. Alsabeeha NH, Payne AG, Swain MV, Attachment systems for mandibular two-implant overdentures: A review of in vitro investigations on retention and wear featuresInt J Prosthodont 2009 22:429-40. [Google Scholar]
[15]. Zitzmann Nicola U, Rohner Urs, Weiger Roland, Krastl Gabriel, When to choose which retention element to use for removable dental prosthesisInt J Prosthodont 2009 22:161-67. [Google Scholar]
[16]. Zahler JM, Intracoronal precision attachmentsDent Clin North Am 1980 24(1):131-41. [Google Scholar]
[17]. Phoenix RD, Cagna DR, De Freest CF, Stewart's clinical removable partial prosthodontics 2003 3rd edIllinois, USAQuintessence books:351 [Google Scholar]
[18]. Avrampou M, Kamposiora P, Papavasiliou G, Pissiotis A, Katsoulis J, Doukoudakis A, Design of removable partial dentures: a survey of dental laboratories in GreeceInt J Prosthodont 2012 25(1):66-69. [Google Scholar]
[19]. Wolf K, Ludwig K, Hartfil H, Kern M, Analysis of retention and wear of ball attachmentsQuintessence Int 2009 40(5):405-12. [Google Scholar]
[20]. Wöstmann B, Balkenhol M, Weber A, Long-term analysis of telescopic crown retained removable partial dentures: survival and need for maintenanceJ Dent 2007 35:939-45. [Google Scholar]