Arnold Chiari Malformation with Spina Bifida: A Lost Opportunity of Folic Acid Supplementation
Deepa Ganesh1, Benjamin M Sagayaraj2, Ravi Kumar Barua3, Nidhi Sharma4, Upasana Ranga5
1 Assistant Professor, Department of Gynaecology, Saveetha Medical College and Hospital, Chennai, Tamilnadu, India.
2 Associate Professor, Department of Paediatrics, Saveetha Medical College and Hospital, Chennai, Tamilnadu, India.
3 Professor, Department of Gynaecology, Saveetha Medical College and Hospital, Chennai, Tamilnadu, India.
4 Associate Professor, Department of Gynaecology, Saveetha Medical College and Hospital, Chennai, Tamilnadu, India.
5 Associate Professor, Department of Radiology, Saveetha Medical College and Hospital, Chennai, Tamilnadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Deepa Ganesh, 51 A Medavakkam Tank Road, Kilpauk, Chennai-600010 Tamilnadu, India. Phone : 9841257779, E-mail : drdeepa@gmail.com
In Arnold Chiari (kee-AHR-ee) II malformation elongated cerebellar tonsils are displaced inferiorly through the Foramen Magnum into the upper cervical spinal canal. It is a complex anomaly with skull, dura, brain, spine and cord manifestations. Meningomyelocele is seen in all cases. We present a case of type II Arnold Chiari Malformation diagnosed in utero in a pregnant lady .There was no periconceptional folic acid supplementation. As the role of the Methylene Tetra Hydro Folate Reductase gene polymorphism in neural tube defects is becoming evident, a simple opportunity as folic acid supplementation should not be missed. Folate supplementation as fortification of cereal grains will also prevent other conditions like congenital heart defects, urinary tract anomalies, orofacial defects, limb defects and pyloric stenosis.
Arnold chiari, Folic acid, Pregnancy, Periconception
Case Report
A 20-year-old lady presented to the Antenatal clinic at 28 wk of gestation for routine antenatal check up. Her last menstrual period was seven months back. She was a Primigravida, with a second degree consanguineous marriage to her mother’s cousin brother. Her menstrual cycles were regular and she was married for one year. She had no history of contraceptive use .She gave no history suggestive of intake of ovulation induction drugs. She was moderately pale and had received no folic acid or iron supplementation .On examination uterine symphysio-fundal height corresponded to 28 wk of gestation .Fetal movements were present and fetal heart was heard. Her haemoglobin was 9 gm/dl and peripheral smear was neutrophilic, normocytic and normochromic.
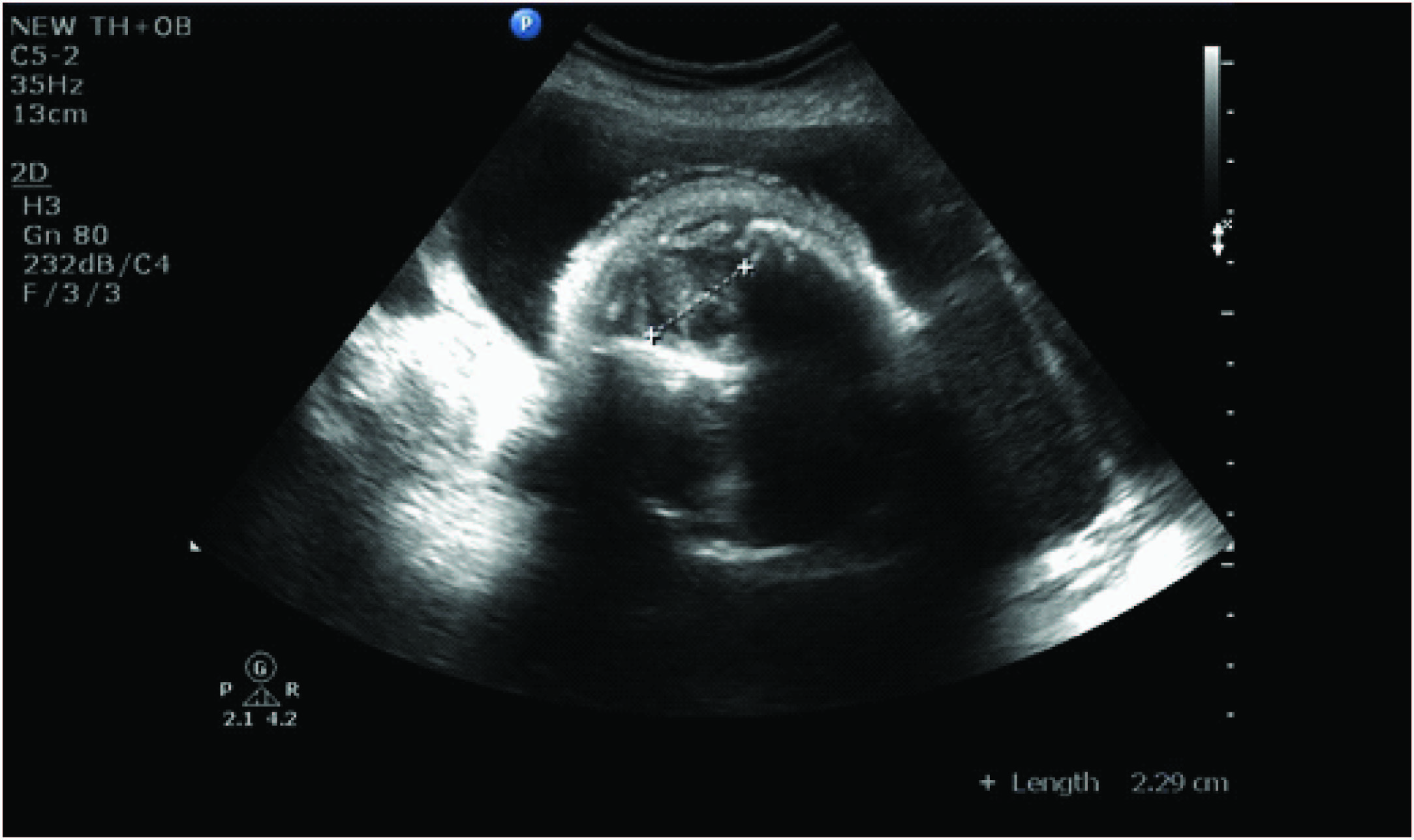
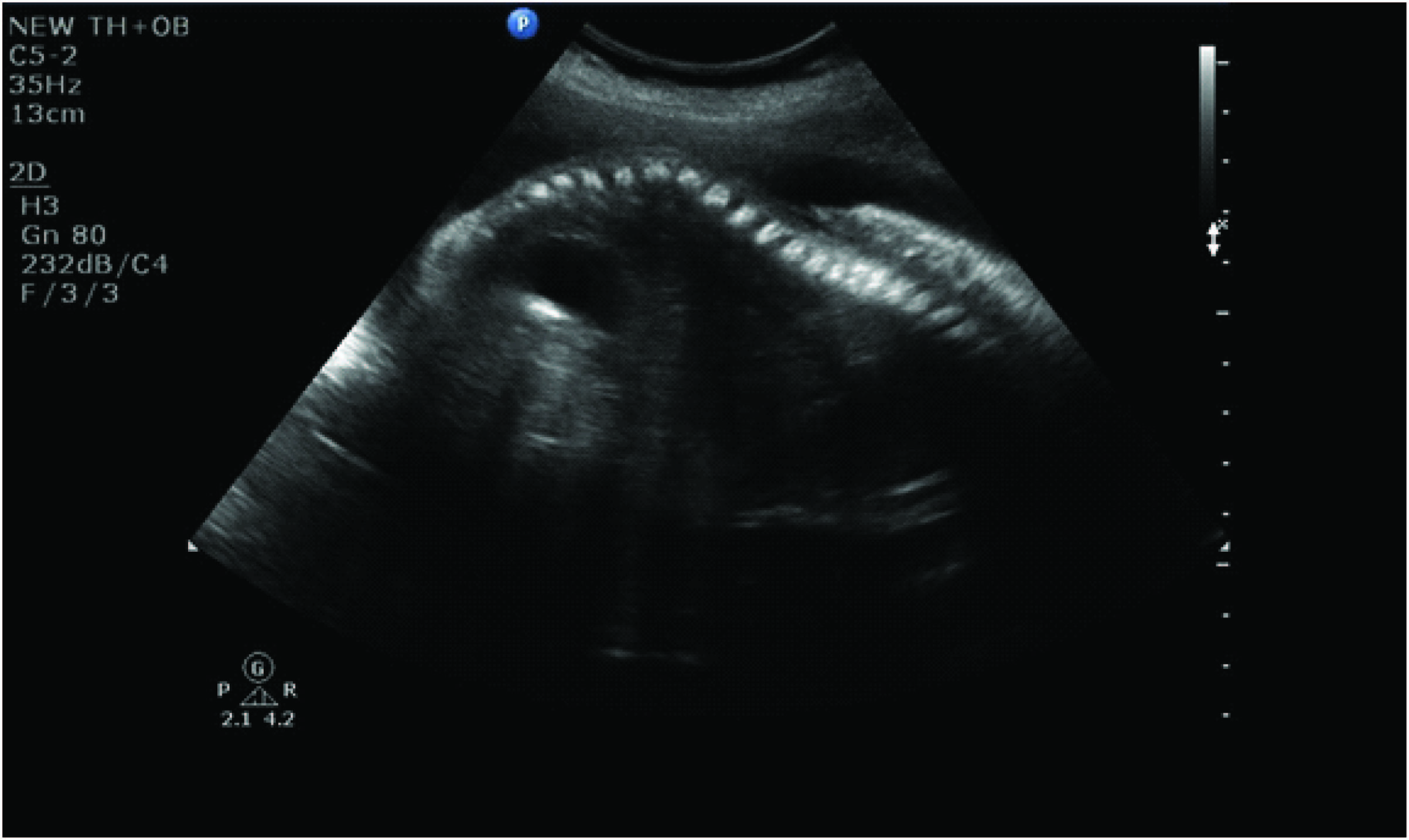
Obstetrical ultrasonography of fetal cranium revealed a crowded posterior fossa and dilated supratentorial ventricular system suggestive of hydrocephalous [Table/Fig-1a]. The spinal canal in cervical region was dilated. There was absence of spinous processes in the lumbar spine [Table/Fig-1b]. MRI showed type II Arnold Chiari malformation. There was hydrocephalous with cerebellar herniation [Table/Fig-2]. There was open spinal dysraphism with dorsolumbosacral myeloschiasis. One unit of cross matched packed cells was transfused. Consent for medical termination of pregnancy was taken after counseling the couple. Labour induction and augmentation was done with two Prostaglandin E2 gel. A male baby of 1.1 kg was delivered vaginally. Cord blood was collected for karyotyping. The baby had hydrocephalous with a swelling in the posterior occipital region. Open spinal cord with meningo-myelocele was present in the lumbo-sacral region [Table/Fig-3]. A CT scan of the still born baby confirmed spina bifida [Table/Fig-4]. The dead fetus was sent for autopsy. Fetal autopsy report showed a 27 wk male foetus of 1100 gm with a crown rump length of 20 cm, crown heel length of 34 cm, chest circumference of 23 cm and head circumference of 27 cm. The umbilical cord had normal insertion (2 cm from the edge of placenta). Head circumference was measured as 22 cm. There were purulent exudates over the meninges and dilated ventricles. The cerebral tonsils were displaced inferiorly through the foramen magnum into the upper cervical spinal canal. Microscopic study of cerebellum revealed focal gliotic scarring of the cerebellar tonsils. Spine showed spina bifida and rachischisis from D10 level to S1 level with absence of posterior spinal elements. Patient was discharged on folate and iron supplements. Fetal karyotype study was normal.
Fetal ultrasound with crowded posterior fossa, ventriculomegaly and dilatation in upper spinal canal
Fetal ultrasound with meningomyelocele
Fetal MRI: Hydrocephalous with cerebellar herniation. There is open spinal dysraphism with dorsolumbosacral myeloschiasis

The still born baby with a swelling in the posterior occipital region. Open spinal cord with meningo-myelocele is present in the lumbo-sacral region

CT scan spine of the still born birth

Discussion
Arnold Chiari malformations were first described in pediatric autopsy specimens in 1891 by Hans Chiari -Austrian Pathologist (1851-1916) [1]. In legacy with the name of his professor Dr Arnold, and his name, the hind brain disorder is named as Arnold Chiari malformation [2]. The incidence is gradually rising because of increased detection with MRI. Exact etiology so far is unknown. Chiari I malformation, the tonsillar ectopia is mostly asymptomatic until adulthood. The diagnosis is made by measuring how far the tonsils protrude below the margin of foramen magnum. The measurement is taken from (ophisthion to basion) inner margins of foramen magnum to the inferior most part of tonsils. A simple rule [3] is
Above the foramen magnum : normal
< 5mm : also normal but the term benign tonsillar ectopia can be used
>5 mm : Chiari I malformation
It should also be noted that the “normal’ position of cerebellar tonsils varies with age [4]. In neonates the tonsils are located just below the foramen magnum and descend further during childhood, reaching their lowest point somewhere between 5-15 years of age. As the age advances the tonsils ascend and come to rest at the level of foramen magnum [4].
In Chari II malformation, the pegs like (cf rounded) cerebellar tonsils are displaced inferiorly through the foramen magnum into the upper cervical spinal canal. The vermis the fourth ventricle and medulla are normal or minimally deformed. Moderate hydrocephalous has been documented in about 25% cases [2]. Syringomyelia is present in 60% of established cases. Skeletal anomalies are found in 25% of cases. Basilar invagination are found in 50% of cases, Klippel Feil syndrome is present in upto 10% of cases. Atlanto-occipital assimilation can also be present.
Skull malformations may include calvarial defects (lacunar skull).There is small posterior fossa with low lying transverse sinuses. The falx is fenestrated and the tentorium hypoplastic. Foramen magnum is wide. Brain anomalies include inferiorly displaced vermis, medullary kink and spur. Corpus callosal hypoplasia or complete agenesis may be present. Myelomeningocele is present in all cases. We speculate that hind brain herniation is secondary to meingomyelocele. This results as a consequence of failed posterior neural pole closure. The posterior neural pole usually closes at 6 wk of menstrual age [5].
The Chiari III malformation includes herniation of hindbrain into the low occipital and high cervical region along with Chiari II malformation [2]. In rare cases the pons and medulla may also be herniated. The herniated brain tissue may show necrosis, fibrosis and gliosis. The Chiari IV malformation is a case of severe cerebellar hypoplasia. The posterior fossa is large, the brain stem is small and there is no hydrocephalous [2].
In view of the severe morbidity associated with these malformations, a daily intake of 400μgms of folic acid is recommended in the preconception period. The Methylene tetrahydrofolate dehydrogenase gene (MTHFD is one of the key genes involved in folate pathway [6]. A large metanalysis study strongly suggests that the MTHFD 1 G1958A gene polymorphism is strongly related to neural tube defects [6]. Genetic defects are not modifiable. Albeit, a lot can be done to fortify folic acid supplementation in pregnancy to reduce the incidence of neural tube defects. Folic acid is heat labile. Avoiding overcooking, including fresh green leafy vegetables in diet and cereal grain fortification of folate can reduce the incidence of all folate deficiency associated congenital anomalies.
Open neural tube defects, can be repaired in utero, as documented recently in the Ochsner experience [7]. The timely closure of spinal defect with seprafilm prevents hind brain herniation. The scar is well healed at birth and the neurological damage is prevented. This research protocol was not possible in our hospital. We had to terminate the pregnancy after prognosticating the parents. Although a preconceptional folic acid supplementation could have been done in our set up, this was missed, as the lady presented late in the pregnancy. Majority of neural tube defects can be prevented by folic acid supplementation in the preconceptional period. Folic acid fortification of staple food grains has lead to reduction of incidence of neural tube defects in USA, Canada, Mexico and Nova Scotia [8–11]. In Europe, the European Registration of Congenital Anomalies and Twins (EUROCAT) has published a special report on the prevention of neural tube defects by periconceptional folic acid supplementation [12]. Associations of Arnold Chiari malformations with low serum Vitamin B12 levels have been documented in two studies [13,14].
It is believed that 1; 00,000 years ago our ancestors ate 14-16 servings of fresh fruits and vegetables (major source of folic acid) each day [5]. With our modern cooking, we are all at a risk of inadequate folic acid intake through diet alone. Folate is required to synthesize RNA and DNA, required for growth, repair and adequate immune response.We should have adequate folate as children for appropriate growth, as women to prevent birth defects and as adults for proper cardiovascular health and cancer protection. The best possible strategy would be fortification of staple cereal grains with daily intake of 400μg folate. A potential effect would be unmasking of background Vitamin B12 deficiency.This will need attention especially in elderly population to prevent neuropathy.A dual fortification with folate and Vitamin B12 can be considered in India as well. The opportunity is open.
Conclusion
Arnold Chiari Malformations can be prevented by preconceptional folic acid and Vitamin B 12 supplementation. In India, most of the pregnancies are unplanned. The rostral and caudal neural pores close at 6 wk of gestation. A delayed folic acid supplementation is bound to miss the vital period of organogenesis and neural tube closure. It is imperative to supplement our cereal grains with folic acid and vitamin B12 to prevent the social and economic burden of birth defects.This strategy has already benefitted developed countries.
Competing Interests
We do not have any commercial association that might pose a conflict of interest in connection with the manuscript. We certify that neither this manuscript nor one with substantially similar content under our authorship has been published or is being considered for publication elsewhere.
[1]. Tubbs R Shane, Aaron A, Cohen-Gadol Hans Chiari (1851-1916)J Neurol 2010 257:1218-20. [Google Scholar]
[2]. Sarmah, Prakritish Bora. Arnold Chiarri Malformation Type II. Ped Rad. (serial online) Vol 9, no 10 http://www.kinderradiologie-online.de/radiology/20091018134917.shtml#.VGWfUzSUcR1 [Google Scholar]
[3]. Elster AD, Chen MY, Chiarri I Malformation: Clinical and radiological reappraisalRadiology 1992 183(2):347-53. [Google Scholar]
[4]. Kornienko VN, Pronin IN, Diagnostic Neuroradiology 2005 VerlagSpringerISBN : 3540213406 [Google Scholar]
[5]. Hall Judith G, Folic acid: the oppourtunity that still existsCMAJ 2000 162(11):1557-59. [Google Scholar]
[6]. Jianxin Jiang, Yanfei Zhang, Liang Wei, Zhiyang Sun, Zhongmin Liu, Association between MTHDI G1958A Polymorphism and neural tube defects susceptibility: A Meta-AnalysisPlos One 2014 9(6):e1011169 [Google Scholar]
[7]. Kahn Lora, Mbabuika Nnenna, Edisan P, Valle–Giler Juanita Graces, Moore R. Clifton, Hilaire and Cuong J Bui (2014) Fetal Surgery: The Ochsner experience with in-utero spina bifida repairThe Ochsner Journal 2014 14(1):112-18. [Google Scholar]
[8]. Bonin MM, Bretzlaff JA, Therrien SA, Rowe BH, Knowledge of periconceptional folic acid for the prevention of neural tube defects. The missing links. Northeastern Ontario Primary Care Research GroupArch Fam Med 1998 7:438-42. [Google Scholar]
[9]. Ray JG, Meier C, Vermeulen MJ, Boss S, Wyatt PR, Cole DE, Association of neural tube defects and folic acid fortification in CanadaThe Lancet 2002 360(9350):2047-48. [Google Scholar]
[10]. Martinez de Villareal L, Decline of neural tube defects cases after a folic acid campaign in Nuevo Leon, MexicoTeratology 2002 66(5):249-56. [Google Scholar]
[11]. Persad VL, Van den Hof MC, Dube JM, Zimmer P, Incidence of open neural tube defects in Nova Scotia after folic acid fortificationCanadian Medical Association Journal 2002 167(3):241-45. [Google Scholar]
[12]. Meijer WM, de Walle HE, Differences in folic acid policy and the prevalence of neural-tube defects in Europe; recommendations for food fortification in a EUROCAT report.(Article in Dutch)Ned Tijdschr Genneeskd 2005 149(46):2561-64. [Google Scholar]
[13]. Verma R, Pratiaraj HN, Unusual association of Arnold Chiari malformation and Vitamin B12 deficiencyBMJ Case Reports 2012 2012:piibrc0320126138 [Google Scholar]
[14]. Welsch Melanie, Antes Sebastian, Kiefer Michael, Meyer Sascha, Eymann Regina, Association of Chiari malformation and Vitamin B12 Deficiency in a familyChilds Nervous System 2013 29(7):1193-98. [Google Scholar]