Case Report
A 21-year-old lady from Darjeeling district accidentally was detected for anomalies in the right hand, while she has accompanied her brother for symptom with fever and cold in Paediatric Medicine OPD. There was a wide U shaped gap in her right hand with only hypoplastic thumb and little finger. All other central digits were absent. The deformity represented as Atypical ‘Cleft Hand’ or ‘Lobster claw deformity’ [Table/Fig-1]. All the movements of thumb were also restricted notably. On examination there were no malformations found in fellow side as well as in lower limbs, palate, lips, ears or elsewhere [Table/Fig-2] . As told by the subject there was no such anomaly in her siblings nor in parents.
On skiagraphy [Table/Fig-3] of antero-posterior view of the affected hand, features found were as described below:
1. Carpal bones: There were normal two rows of carpal bones. The scaphoid and trapezium could not get isolatedly identified. Instead of them, a larger bony mass was found as the fused masses of those two bones (scapho-trapezoid fusion).
2. Metacarpal bones: Metacarpals of central digits (second, third and fourth) were grossly hypoplastic only retaining their bases, which were fused to respective carpal bone loosing carpo-metacarpal joints. The prominent first metacarpal was also fused with the scapho-trapezoid mass and hence the first carpo-metacarpal joint was also absent. The first and fifth metacarpal have less prominent heads compared to the fellow side.
3. P halanges: Absent for central digit. For the thumb and little finger only the proximal digits were present.
4. Joints:
(a) Intercarpal joints: present, besides the scapho-trapezoid part
(b) Carpo-metacarpal joints: absent, besides the base of fifth metacarpal
(c) Metacarpo-phalangeal joint: Only in first and fifth finger
(d) Interphalangeal joint: absent
Skiagram of fellow side was found to be normal in all aspect [Table/Fig-4]. Karyotyping was done and found for 46 XX normal presentations. Ultrasonographic and echocardiographic screening also revealed no abnormality. Detailed further chromosomal studies could not be done due to infrastructural limitation.
On further interview, the lady could not provide any significant antenatal history of her mother. Her other siblings were normal and with no deformities. She had her normal life since birth except such hand deformity and could not recall any chronic diseases since childhood.
Discussion
‘Cleft hand’ signifies the groups of malformations in hand where central digits are congenitally absent. It has been reported to be the fifth commonest anomaly of the hand. Earlier researcher has described its incidence to be 1 in 10,000 live births to 1 in 1,20,000 live births. This condition is known in different names as ‘Ectrodactyly’, ‘lobster-claw deformity’, ‘pincer-cleft deformity’, ‘crab-claw deformity’ as well as ‘split-hand malformation’. The bones of lateral sides (thumb-index finger) and those of medial side (ring-little finger) commonly show fusion. The two parts of hand are somewhat opposed to each other acting as lobster-claw [1-4]
The spectrum of presentation may be from absence of single central digit upto absence of all the digits. The clefting depends upon the presence of metacarpal bones, as more will be presence, more is the clefting. This deformity according to its presentation has been categorized as;
Type 1 (Typical): Typical V-Shaped clefting with presence of metacarpals, typical crab-clawing of the extreme fingers, bilateral, involving foot, associated with other developmental defects (syndromic presentation) viz. anencephaly, cleft lip, cleft palate etc. In these cases familial inheritance are often seen.
Type 2 (Atypical): Atypical cleft, often U or spreaded U shaped, unilateral, sporadic, un-inherited, involving one limb, partial/ complete absence of metacarpals, hypoplastic thumb & little finger, not associated with other syndromic manifestations. Phenotypically our case belonged to this category.
Type 3 (Nil-clefting): where all digits are absent, and there will be no cleft further [5-7].
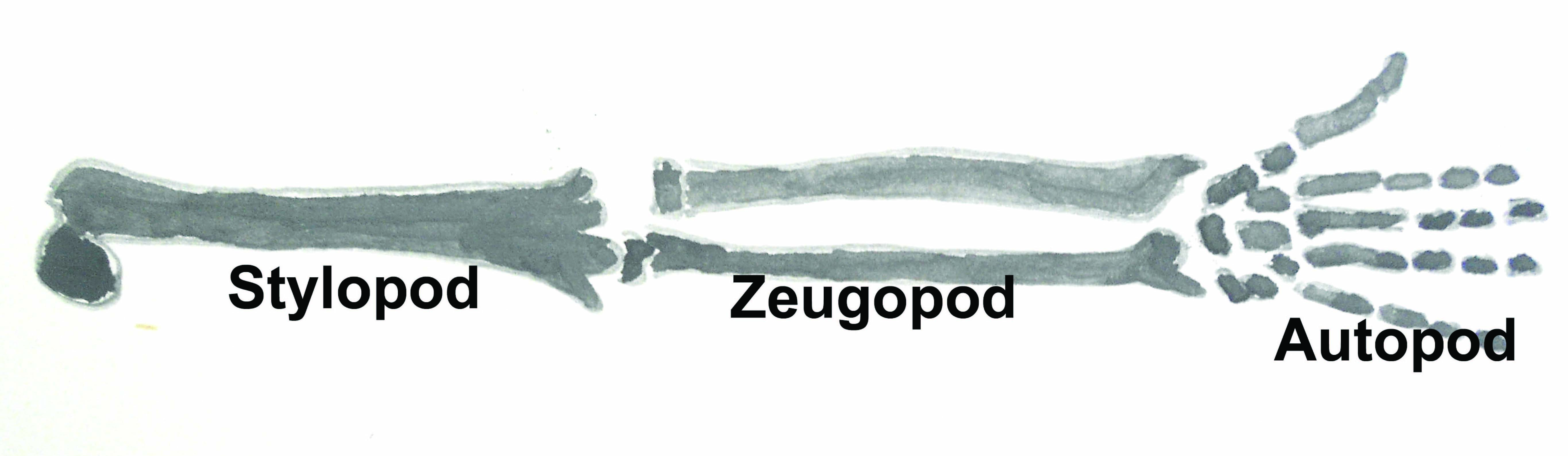
Malformations have been explained in the literature as abnormal intrinsic embryonic development due to genetic defect as a consequence of exposure to teratogens or maternal metabolic disease. For description the developing limb is divided in three zones proximo-distally as Stylopod (girdle to first hinge joint; in case of upper limb, the arm), Zeugopod (from first to second hinge joint; in case of upper limb, the forearm), Autopod ( the most distal part carrying phalanges; viz. palm and sole) [1,8-11] [Table/Fig-5].
Developing limb is dually contributed by lateral plate and somatic mesoderm. Within the proliferated cells of lateral flank, the cells of the adjacent somites (to form muscles, vessels and nerves) start to invade. Such proximo-distal outgrowth is directed by signals from the Apical Ectodermal Ridge (AER) present at distal tip. Fibroblast growth factors (Fgfs) acts as key mediators to strengthen it. The antero-posterior patterning is modified by Zone of Polarizing Activity (ZPA), a cluster of cells at the posterior border of the limb near the flank [1,8].
Amongst the multiple genes Homeobox (Hox) genes at the 5’ region of chromosome no. 7 & 2 are respectively involved in development and differentiation of limb bud with its different mesodermal elements. The Sonic hedgehog (Shh), similar to Drosophila hedgehog (Hh), a secreted molecule in association of Retinoic acid (Vitamin A) regulates the target genes to regulate the morpho-differentiation of ZPA. The Hox genes recently have been shown gets agonised by Bone morphogenic protein (Bmp) and antagonized by Noggin (Nog) controls the formation of carpals, metacarpals and phalanges [1,8-11].
The gradual deposition and differentiation of cells to form the tissues of limb have been explained by two models, the progress zone model and the early specification model. In the Progress-Zone (PZ) model, the cells acquire their positional information in proximodistal sequence facilitated by the apical ecodermal ridge (AER) in immature condition. As they leaves the progress zone (PZ), they gets differentiation. So the cell that leaves the PZ later will get most distal position. So the first cell leaving the PZ will form the sylopod (S), next batch will form the zeugopod (Z) and the last batch will form the autopod (A) respectively [1,8] [Table/Fig-6].
In the contrary, the Early-Specification (ES) model describes that a pre-specified cell population expanding on the growing limb grows in proximo-distal fashion in response to the cell-to-cell interaction. That explains the cells gets specified for the three zones of limb bud previously in S-Z-A sequence, then expands and finally forms the skeleton-muscular components. 1,7,8 [Table/Fig-6].
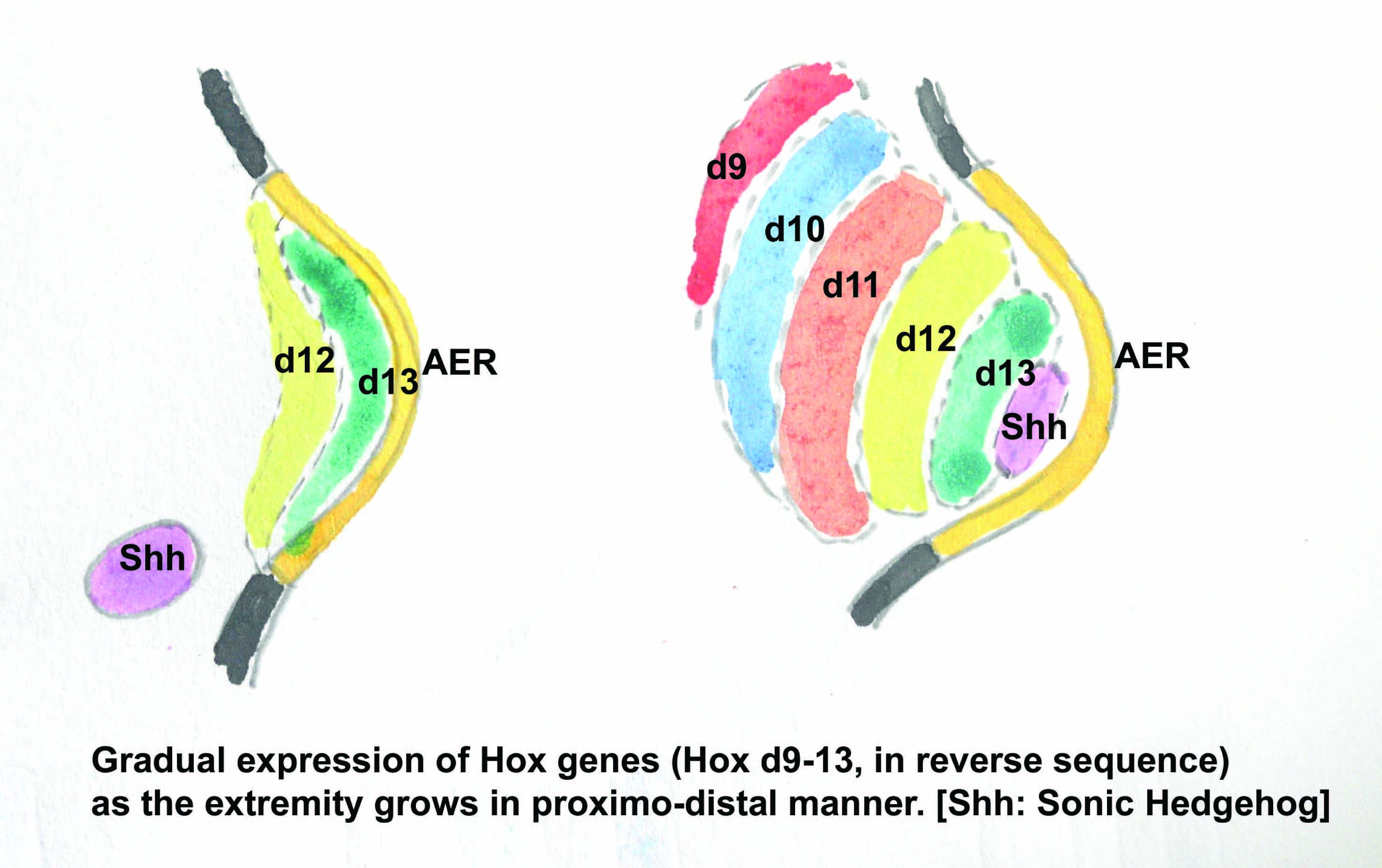
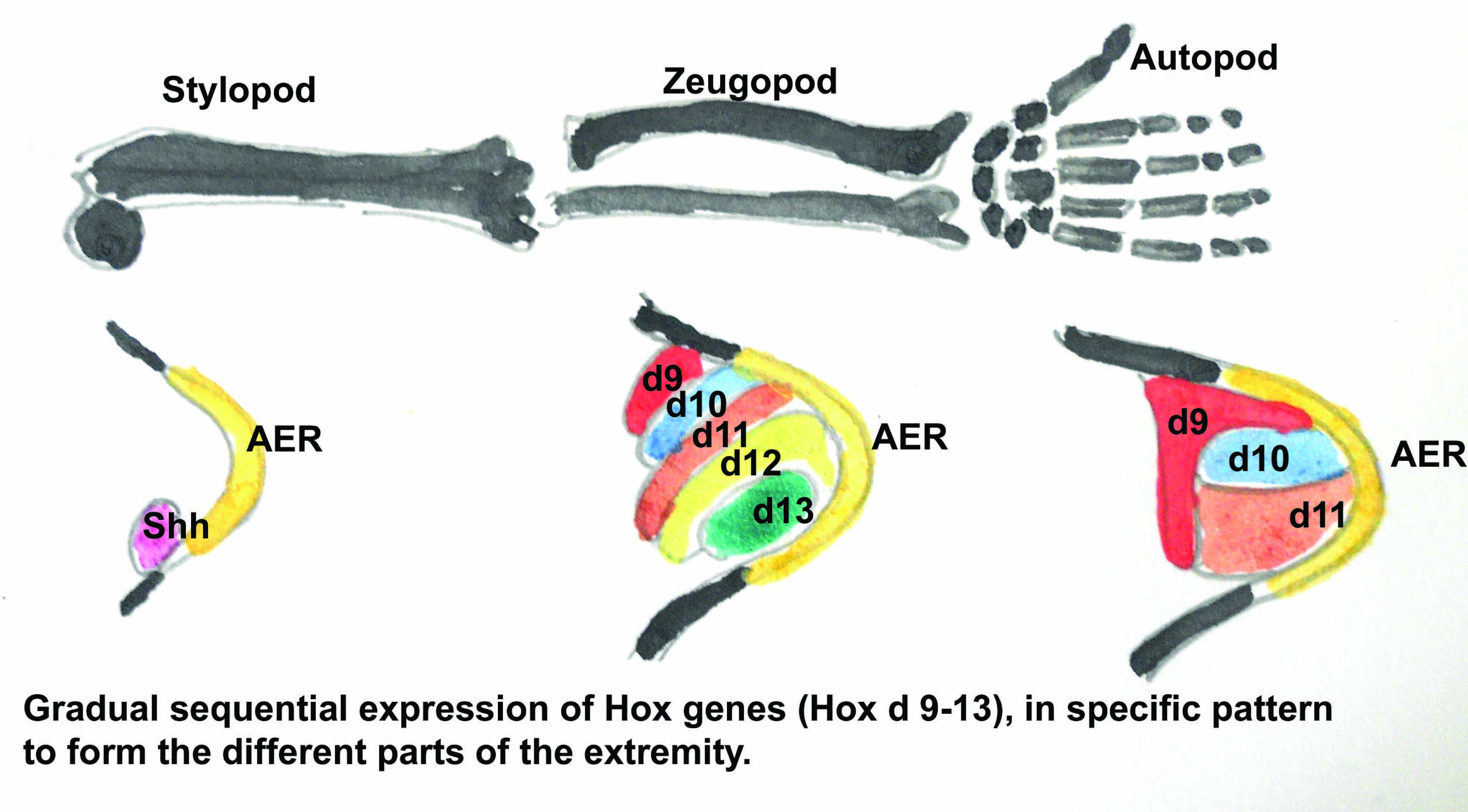
These entire sequencing is mediated by Fgf with the influence of Shh. Wnt7a, another secreted molecule regulates the dorsal identity of the limb. During the entire processing Hox A, D 9-13 genes are expressed in specified rhythm to determine the shape and identity of skeletal elements [1,7,10,11] [Table/Fig-7,8].
Thus, digits also appear in sequential manner, with thumb in the radial side. As the limb grows, the ZPA moves distal wards to remain in proximity to the posterior border of the AER. Any mis-expression or false-expression (missense mutation) of Shh or Retinoic Acid in the anterior margin of the limb leads to digital deformity [1,7].
In recent years cases of cleft hand have been reported from Indian families, where some of the manifestations was familial as well as inherited and in those cases the defect in chromosome no. 7 q deletion have been reported [12-14].
For the split-hand/foot malformation (SHFM) till date four genetic loci have been identified. SHFM1 gets in chromosome 7q21.3-22.1, SHFM2 gets in chromosome Xq26, SHFM3 gets in chromosome 10q25 and SHFM4 caused by mutation of p63 genes on chromosome 3q27. Phenotypically two types of such malformation have been identified, as (Type 1) deficiency of central rays (digits) with a definite cleft (cleft-hand/lobster-clawing), and (Type 2) Monodactyly with only fifth digit. Incidentally it has been found that in all types of SHFM the mutation of p63 gene is participant [15]. The cleft hand can be considered as dactyl dysplasia caused by degeneration of the central segments of apical Ectodermal ridge, leaving only the radial and ulnar rays intact, proposed to be caused by missense mutation of p63 gene [11-15].
Such a deformity not only carries functional limitation of the affected hand, but also high degree of psychiatric morbidity of the patient. Its management depends on high-skilled plastic (cosmetic) surgery with rehabilitation. Basic target of surgery is to achieve a good pinch-and-gasp along with acceptable cosmesis. In typical clefthands surgery is quiet easier with cleft-closure, syndactyly-release, correction of thumb adduction and removal the deforming bones [16-18].
But in atypical cleft hands, the hypoplastic thumb and/or little finger makes it challenging; where surgeons use to follow Z-plasty in the first stage with removal of redundant/rudimentary bone segments following the metatarsal osteotomy, to improve the gap. On absence of metatarsal, this also becomes difficult and in those cases grafting becomes essential. But whatever be the approach full correction is almost impossible [16-18].
The figure showing two hands of the lady: right hand having atypical spreaded-U clefting in hand, with normal fellow hand

Besides the one limb, there were no obvious anomalies in other limbs to the lady (hence a monomelia)

Skiagram of the affected hand, showing (1. Schapho-trapezo-metacarpal fusion in first digit( 2. Normal trapezoid and capitate with fused bases of the respective metacarpals. (3. Separate rudimentary base of the third metacarpal (4. Isolated prominent fifth metacarpal (5. Proximal phalanx of little finger

Skiagram of both hands, where the left side is normally developed

Developmental nomenclature of different parts of a developing limb. ‘Stylopod’ demarcates the arm, ‘Zeugopod’ demarcates the forearm and ‘Autopod’ demarcates the hand
Above figure represents two ‘models’ of development of the limb. After the AER (Apical Ectodermal ridge) appears in the side of the flank, there are two hypotheses of limb growth. [In figure abbreviated as, AER: Apical Ectodermal ridge; PZ: Progress zone; ZPA: Zone of Polarising activity; S: Stylopod formative genes; Z: Zeugopod formative genes; A: Autopod formative genes]
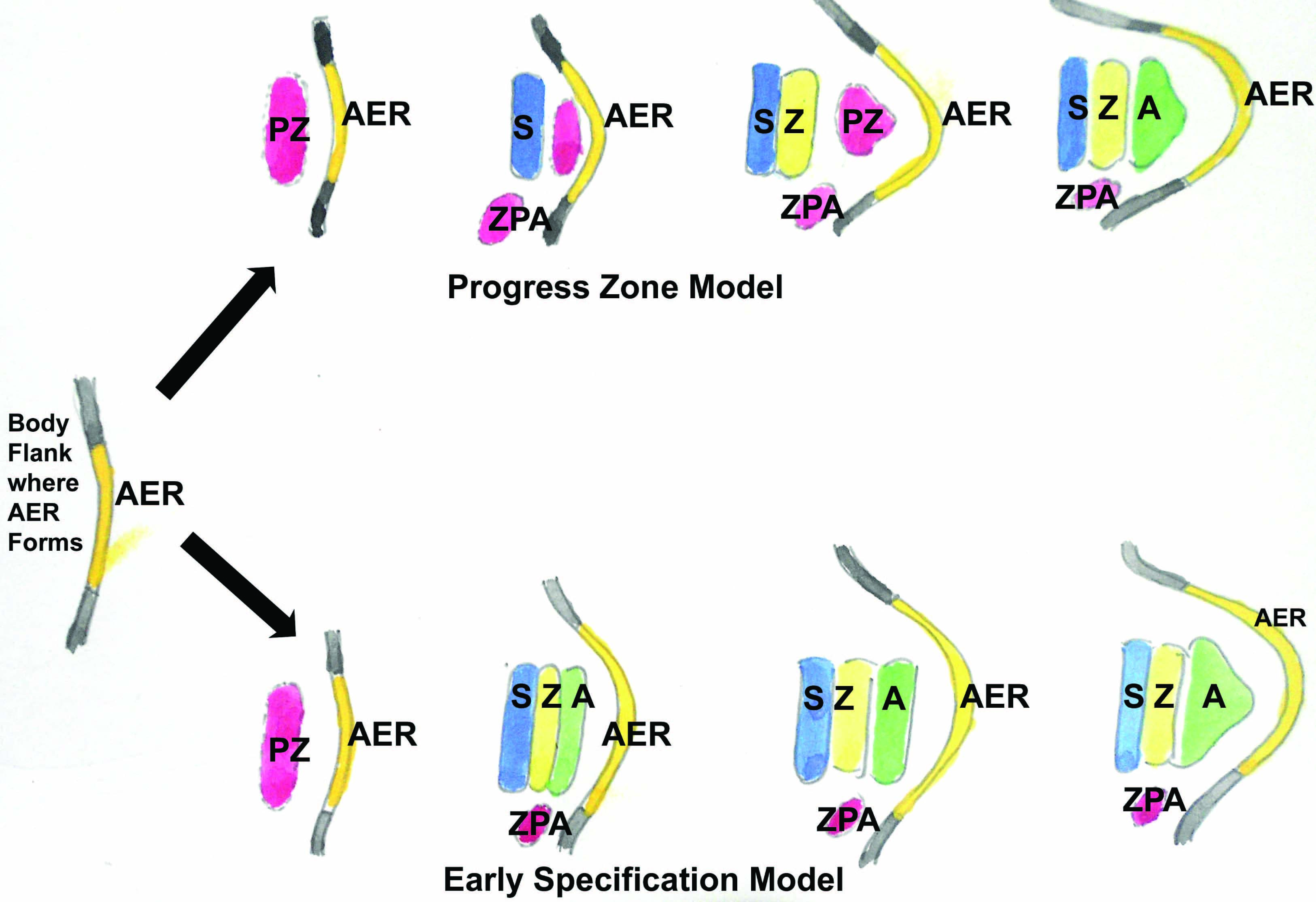
Figure describes the gradual expression of Hox genes along with the growth of the extremity. [In figure abbreviated as, Shh: Sonic hedgehog gene; AER: Apical Ectodermal ridge; d 9-13: expression of Hox D 9-13 genes]
sequential Hox gene expression in formation of different components of the developing limb
Conclusion
Such an anomaly with higher degree of functional limitation as well as psychological depression has now-a-days been regarded as a social burden. So earlier will be the presentation, easier will be the correction. Thus detection at birth requires utmost importance. Our endeavor was to get the ontogenetic explanation of such cases in purview of the knowledge of Embryology.
Acknowledgement
The authors sincerely do acknowledge the patient to provide her consent for photography. They also like to express sincere regards to the honorable Principal of the institute and the HOD, Dept. of Pediatrics for their permission to do this study.
[1]. TW Sadler, Clinical correlates. In- Skeletral system (ch. 9). Langman’s medical embryologyTeratology 2009 11th EditionNew DelhiWolter Klauer Health (India) Pvt. Ltd:136-41. [Google Scholar]
[2]. PW Buss, Cleft hand/foot: clinical and developmental aspectsJ Med Genet 1994 :726-30. [Google Scholar]
[3]. K Tsuge, S Ischii, Y Lieba, Report of the Japanese Society for surgery of the hand, committee on congenital malformations of the handOrthop Surg (Jpn) 1980 31:1959-63. [Google Scholar]
[4]. AN Baba, YJ Bhat, SM Ahmed, A Nazir, Unilateral cleft hand with cleft footInternational Journal of Health Sciences, Qassim University 2009 3(2):243-46. [Google Scholar]
[5]. AB Swanson, A classification for congenital hand malformationsJ Hand Surg 1976 1:8-22. [Google Scholar]
[6]. SC Jr Sandzén, Classification and functional management of congenital central defect of the handHand Clin 1985 1:483-98. [Google Scholar]
[7]. W Blauth, A Falliner, Morphology and classification of cleft handsHandchir Mikrochir Plast Chir 1986 18:161-95. [Google Scholar]
[8]. GC Scwabe, S Mundlos, Genetics of congenital hand malformationHandir Mikrochir Plast Chir 2004 36:85-97. [Google Scholar]
[9]. DO Maisels, Theory of Pathogenesis of Lobster Claw deformitiesHand 1970 2:79 [Google Scholar]
[10]. BD Caldwell, Genetics of split hand and split foot: a case studyJ Am Podiatr Med Assoc 1996 86:244-48. [Google Scholar]
[11]. P Ianakiev, MW Kilpatrick, I Toudjarska, Split-hand/split-foot malformation is caused by mutations in the p63 gene on 3q27Am J Hum Genet 2000 67:59-66. [Google Scholar]
[12]. SD Amalnath, M Gopalakrishnan, TK Dutta, Split-hand/feet malformation in three tamilian families and review of the reports from IndiaIndian J Hum Genet 2014 20(1):92-95. [Google Scholar]
[13]. A Agrawal, R Agrawal, R Singh, R Agrawal, S Agrawal, Lobster claw deformityIndian J Dent Res 2014 25(2):243-47. [Google Scholar]
[14]. A Gulia, A Marwah, Unilateral cleft hand (lobster-claw deformity)Indian J Med Res 2013 138(6):1031-32. [Google Scholar]
[15]. A Patel, D Sharma, J Yadav, E Garg, Split hand/foot malformation syndrome (SHFM): rare congenital orthopaedic disorderBMJ Case Rep 2014 :2014 [Google Scholar]
[16]. V Wood, The cleft-hand (Central deficiencies) In: Green DP, ed. Operative Hand Surgery 1982 New YorkChurchill-Livingstone:233-43. [Google Scholar]
[17]. SPJ Kay, AJ Platt, Congenital disorders: Cleft hand (Chapter 86). In- Hand surgery 2004 1st EditionPhiladelphiaLippinkotts Williams & Willkins:1465-67. [Google Scholar]
[18]. AE Flatt, Cleft hand and central defects. In Flatt AE (Ed). The care of congenital hand anomaliesTetracyclineTeratology 1994 St LouisMO: Quality Medical Publishing:337 [Google Scholar]