A Rare Presentation of Gastric Signet Ring Cells: Signet Ring Cell Lymphoma
Sithara Venkateshwar1, Thomas Alexander2, Moses Ambroise3, Renu G’Boy Varghese4, Anita Ramdas5
1Post Graduate, Department of Pathology, Pondicherry Institute of Medical Sciences, Ganapathychettikulam, Kalapet, Pondicherry, India.
2Professor, Department of Gastroenterology, Pondicherry Institute of Medical Sciences, Ganapathychettikulam, Kalapet, Pondicherry, India.
3Assistant Professor, Department of Pathology, Pondicherry Institute of Medical Sciences, Ganapathychettikulam, Kalapet, Pondicherry, India.
4Professor and Head of Department, Department of Pathology, Pondicherry Institute of Medical Sciences, Ganapathychettikulam, Kalapet, Pondicherry, India.
5Professor, Department of Pathology, Pondicherry Institute of Medical Sciences, Ganapathychettikulam, Kalapet, Pondicherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sithara Venkateshwar, Pondicherry Institute of Medical Sciences, Ganapathychettikulam, Kalapet, Pondicherry-605014, India.
Phone: 9176626410,
E-mail: sitharavenkateshwar@gmail.com
We herewith present a rare and interesting case of gastric signet ring cell lymphoma (SRCL) in a 40-year-old retroviral positive lady. SRCL is a rare morphological variant of nodal lymphomas.Biopsy from the suspected lesion in the stomach showed diffuse sheets of cells with a large central vacuole displacing the nucleus to the periphery of the cell, imparting signet ring cell morphology. Negative reaction to PAS (Periodic acid Schiff) stain and subsequent strong positivity for the immunohistochemical markers such as CD45 (Leucocyte commonantigen) and CD20, a B-cell marker helped us to arrive at a diagnosis of signet ring B- cell lymphoma.
Adenocarcinoma, Candidiasis, Lymphoid cells
Case Report
A 40-year-old lady presented to Pondicherry Institute of Medical Sciences, Puducherry, India with complaints of epigastric pain, vomiting and dysphagia for solid food for three months. Epigastric pain was radiating to back, and worsened with food intake. Vomitus was bile stained at times. History of loss of appetite and weight were also present. She had a past history of tuberculosis for which she had taken treatment for six months.
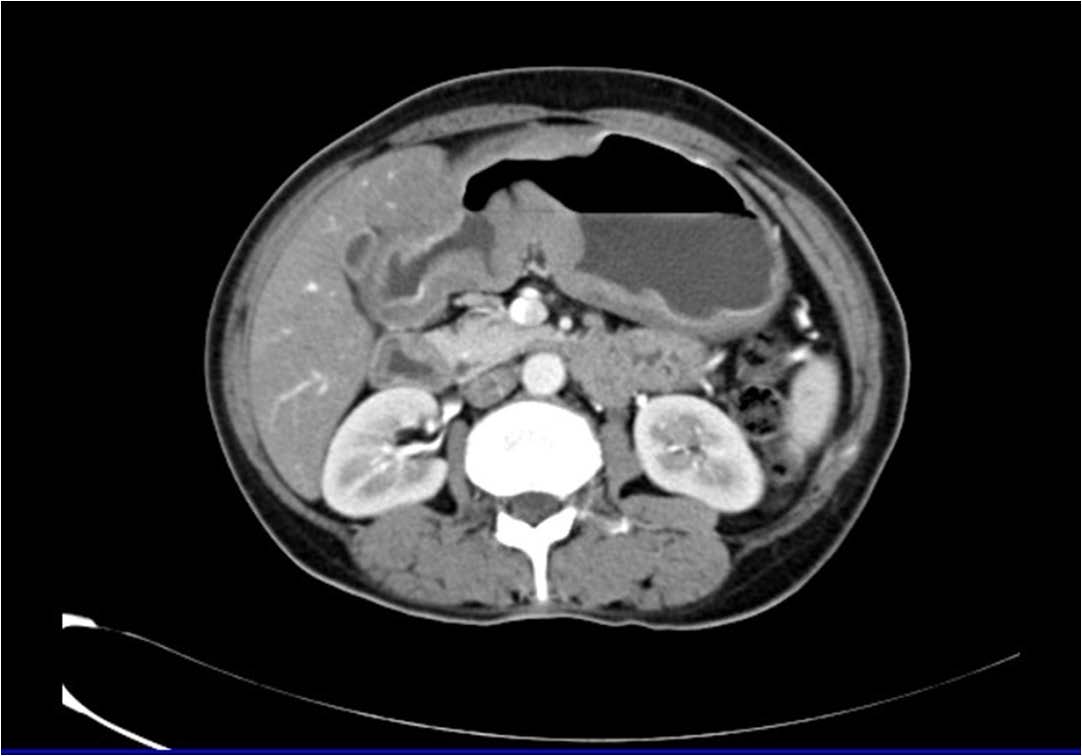
Physical examination revealed tenderness in the upper abdomen without any palpable mass. Oral examination revealed candidiasis. CECT (Contrast enhanced computer topography) abdomen showed thickening of gastric body and antrum with maximum thickness of 17mm [Table/Fig-1]. It also revealed perigastric and celiac lymphadenopathy with the largest lymph node measuring 2.6x1.6cm. Gastroscopy revealed a diffuse thickening of the antrum with edematous duodenal mucosa. Endoscopic mucosal biopsies were taken from these areas.She was also found to be HIV positive.
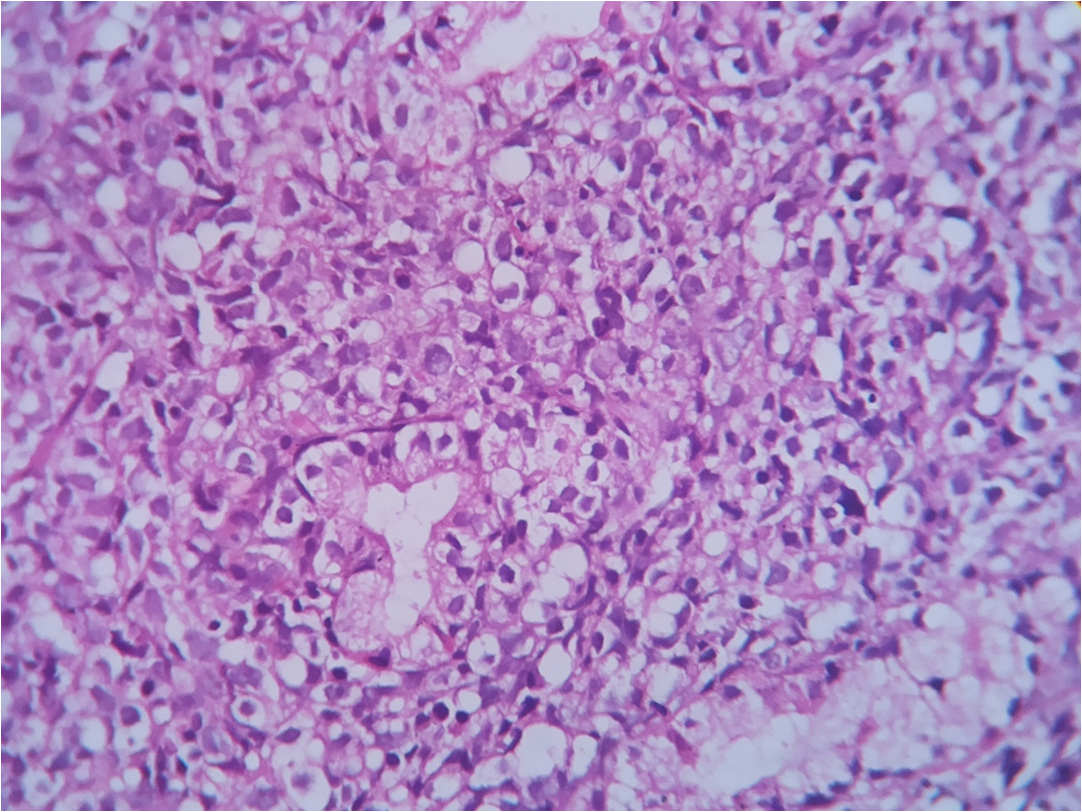
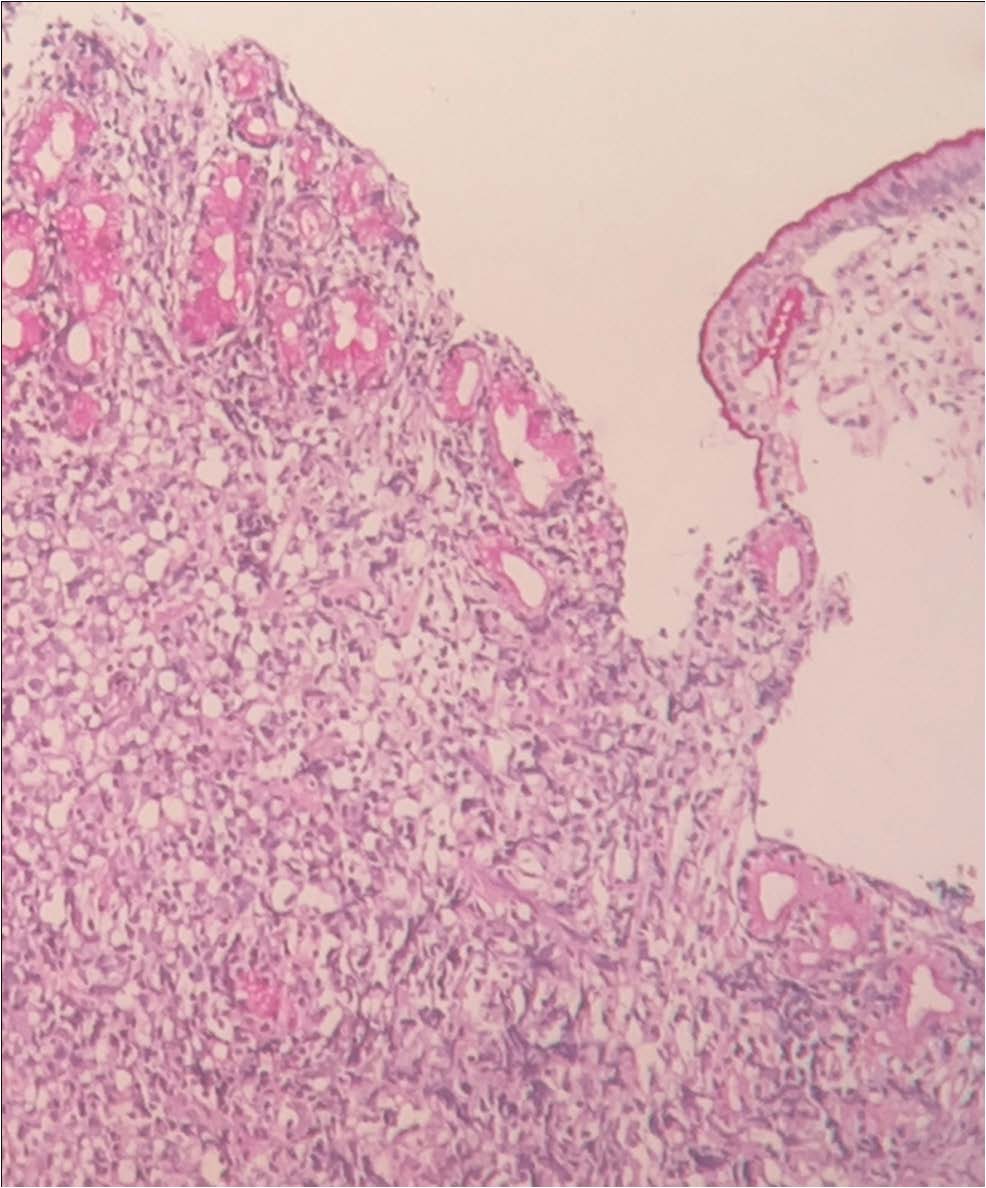
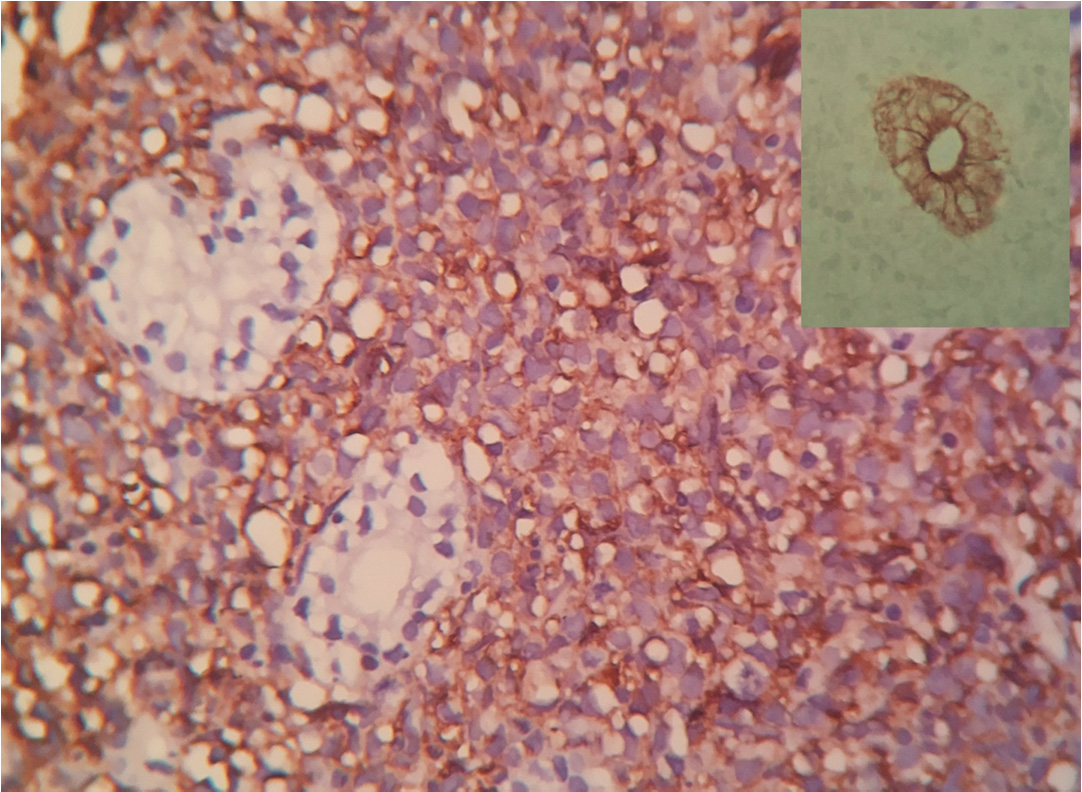
Histopathological examination of mucosal bits from the gastric lesion showed diffuse infiltration by sheets of cells having vacuolated cytoplasm compressing and displacing the nucleus to the periphery of the cell resulting in a signet-ring cell morphology [Table/Fig-2]. Foci of necrosis were also noted. A provisional diagnosis of signetring cell carcinoma was made. PAS stain turned out to be negative [Table/Fig-3]. Hence, the possibility of a signet ring cell lymphoma was thought of and therefore immunohistochemical staining was done. The tumor cells showed strong positive staining with LCA (Leukocyte common antigen) and CD-20 (B-cell marker) and negative staining with CD3 (T-cell marker) and cytokeratin, thus confirming the diagnosis of signet ring cell lymphoma of B – cell origin [Table/Fig-4]. Unfortunately, the patient was lost to follow-up.
Discussion
Signet ring cell lymphoma (SRCL) is a rare morphological variant of Non-Hodgkins lymphoma [1] with cytoplasmic inclusions/ vacuolations pushing the nucleus to the periphery thus imparting a signet ring appearance. These cytoplasmic vacuoles contain immunoglobulins that must be differentiated from the signet ring cells of mucinous adenocarcinoma [2,3]. These signet ring cells lack immunoreactivity with cytokeratin, but show strong positivity with immunomarkers of lymphoid cells such as CD20 [4]. They have been reported as morphological variants of nodal lymphomas usually of follicular origin. SRCL can be subdivided into three cytological subtypes based on tumor morphology and immunohistochemistry as clear cell type, Russell body (Eosinophilic globule) type and hyaloplasmic deposit type [5].
It has been reported in various other sites also and only rarely in the gastrointestinal tract.There are two interesting case reports of its occurrence in the stomach. Sumida et al., have reported a case of H. pylori and API2-MALT1 gene-negative gastric mucosa-associated lymphoid tissue lymphoma with a carcinoma-like signet-ring cell lymphoepithelial lesion [6]. An interesting case of gastric signet-ring cell lymphoma with free alpha chains in the gastro-duodenal juice was also reported earlier [7]. Zamboni et al., noted carcinoma like signet ring cells in 26 out of 70 gastric mucosa-associated lymphoid tissue (MALT) Lymphomas. The signet ring cells were seen as either isolated or grouped in clusters.Their data suggested that signet ring cells occurring in gastric MALT lymphomas could represent a particular type of lymphoepithelial lesion (LEL) in which the foveolar cells disaggregated by the lymphomatous infiltration acquire a globoid, signet-ring appearance [8]. Recently SRCL of the small intestine has also been reported with no associated abdominal lymphadenopathy or splenomegaly. Immunohistochemical markers were consistent with SRCL of B-cell type [9]. Our case revealed sheets of atypical cells with prominent signet ring cell morphology infiltrating gastric glands. But these signet ring cells did not reveal positivity with PAS stain causing a diagnostic dilemma for us.
The various diagnostic possibilities morphologically include signetring cell carcinoma, MALT lymphoma, epithelioid GIST and hepatoid variant of gastric carcinoma.In our case, the tumor cells were negative for cytokeratin, but were positive for LCA and CD20 [10]. Hence, we labeled our case as gastric signet -ring B-Cell lymphoma.Our case is much similar to the earlier case reports [6]. Ultra structure of signet ring cell will also help to differentiate SRCL of B-cell lineage from one of T-cell lineage. Increased number of multivesicular bodies (mVBS) is found in neoplastic than reactive lymphocytes and in T-cell lymphomas [11]. It is also important to remember that signet ring cell lymphomas which contain eosinophilic globules in their cytoplasm can be PAS positive, because of IgM [3].
It is very important from the point of therapy and management that a diagnosis of SRCL should not be missed. In the present case, the initial diagnosis favored was signet-ring cellcarcinoma of stomach and a diagnosis of lymphoma was reached only after histochemical and immunohistochemical results. The clinical manifestations and prognosis of SRCL resembles that of non- SRCL [3,9].
Gastrointestinal lymphomas are uncommon as compared to adenocarcinoma.HIV infected individuals are more vulnerable to develop extra nodal lymphomas and their incidence is increasing in HIV infected and AIDS patients [12]. The prevalence of AIDS associated extranodal lymphomas is increasing even with antiretroviral therapy [13].
CECT showing marked focal thickening of gastric antral wall
Gastric glands invaded by lymphoma cells. H&E 10x
Lymphoma cells showing PAS negativity. PAS stain 10x
Lymphoma cells showing CD 20 positivity. (CD 20 stain 10x). Inset shows lymphoma cells showing Cytokeratin negativity, in contrast to a normal gastric gland. (Cytokeratin stain 40x)
Conclusion
Gastric SRCL should always be considered as a differential for a poorly differentiated neoplasm with signet-ring change in the stomach. The possibility of gastric SRCL must be excluded using histochemical and immunohistochemical studies even in cases with extensive signet ring change.
[1]. N Nakamura, S Yoshida, J Shinzawa, S Yoshida, Y Sasaki, M Sato, Signet ring cell lymphomaJ Clin Exp Hematopathol 2002 43(0.2):71-76. [Google Scholar]
[2]. HL Ioachim, LJ Medeiros, Follicular lymphoma. In: Ioachim HL, Medeiros LJ, editors. Ioachim’s Lymph Node Pathology,TetracyclineTeratology 2009 4th EditionPhiladelphiaLippincottwilliams & Wilkins:395 [Google Scholar]
[3]. JR Krause, Signet ring lymphoma: a potential diagnostic mishapProc (BaylUniv Med Cent) 2013 26(3):293-94. [Google Scholar]
[4]. AM Boguz, B Tierno, D Brown, G Pihan, Extreme signet ring cell change in a large cell lymphoma of follicular originInt J Surg Pathol 2013 21(4):399-403. [Google Scholar]
[5]. T Sumida, S Nagata, H Ohgoshi, Y Ishida, T Kuwabara, T Tsumura, A case of H. pylori and API2-MALT1 gene-negative gastric mucosa-associated lymphoid tissue lymphoma with a carcinoma-like signet-ring cell lymphoepithelial lesionNihon Shokakibyo Gakkai Zasshi 2006 103(11):1257-63.Japanese. PubMed PMID: 17085907 [Google Scholar]
[6]. JJ Navas-Palacios, MD Valdes, JJ Lahuerta-Palacios, Signet-ring cell lymphoma. Ultrastructural and immunohistochemical features of three varietiesCancer 1983 52(9):1613-23. [Google Scholar]
[7]. MF Tungekar, Gastric signet-ring cell lymphoma with alpha heavychainsHistopathology 1986 10(7):725-33. [Google Scholar]
[8]. G Zamboni, G Franzin, A Scarpa, F Bonetti, M Pea, GM Mariuzzi, Carcinomalike signet-ring cells in gastric mucosa-associated lymphoid tissue(MALT) lymphomaAm J Surg Pathol 1996 20(5):588-98. [Google Scholar]
[9]. N Basir, C BickleI, PU Telesinghe, MS Abdulla, VH Chong, Signet cell lymphoma of the small bowel: A case reportOman Med J 2012 27(6):491-93. [Google Scholar]
[10]. M Krsti, V Kati, Histological, mucin histochemical and immunohistochemical features of gastric signet ring cell carcinomaVojnosanit Pregl 2008 65(11):835-38. [Google Scholar]
[11]. BP Eyden, PA Cross, M Harris, The ultrastructure of signet-ring cell non-Hodgkin’s lymphomaVirchows Arch A Pathol Anat Histopathol 1990 417(5):395-404. [Google Scholar]
[12]. M Ahmed, Al-Akwaa N Siddique, A Ibrahim, Al-Molfeh Primary gastric lymphomaWorld J Gastroenterol 2004 10(1):5-11. [Google Scholar]
[13]. MS Shiels, RM Pfeiffer, HI Hall, J Li, JJ Goedert, LM Morton, Proportions of Kaposi sarcoma, selected non-Hodgkin lymphomas, and cervical cancer in the United States occurring in persons with AIDS, 1980-2007JAMA 2011 305(14):1450-59. [Google Scholar]