Influences of Gender on Postoperative Morphine Consumption
Sivakumar Periasamy1, Raja Poovathai2, Srinivasan Pondiyadanar3
1 Associate Professor, Department of Anesthesiology, Critical Care and Pain Medicine, Vinayaka Missions Kirupananda Variyar Medical College & Hospitals, Salem, Tamil Nadu, India.
2 Assistant Professor, Department of Anesthesiology, Critical Care and Pain Medicine, Vinayaka Missions Kirupananda Variyar Medical College & Hospitals, Salem, Tamil Nadu, India.
3 Professor & Head, Department of Anesthesiology, Critical Care and Pain Medicine, Vinayaka Missions Kirupananda Variyar Medical College & Hospitals, Salem, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sivakumar Periasamy, 23/2, Sri Krishna Kudil, Neduncahalai Nagar, Salem-636005, India.
Phone: 9994398639,
E-mail: ssukir@yhaoo.co.in
Background: Gender related differences on morphine consumption during postoperative period following abdominal surgeries.
Materials and Methods: Four hundred and fifty ASA I & II patients of either sex (male =231, female = 219), between the age group of 18-65 y undergoing elective intra abdominal surgeries under general anaesthesia were included for the study. Patients with preexisting pain either acute or chronic preoperatively were excluded from the study. Anaesthesia and analgesia protocol during surgery was standardized. Postoperatively, a loading dose was given to achieve the visual analogue scale (VAS) of ≤30 and subjects were connected to patient control analgesia (PCA) pump containing 0.4 mg/ml of morphine configured to deliver a bolus dose (1 mg) with a 5 min lock-out period. The total analgesic requirements along with VAS (visual analog scale) score were analysed between males and females in the first 24 h postoperatively. All demographic data and between group comparisons were analysed with student t-test. Within group comparisons were done by using one-way-ANOVA test and Tukey’s Honestly significant Difference test.
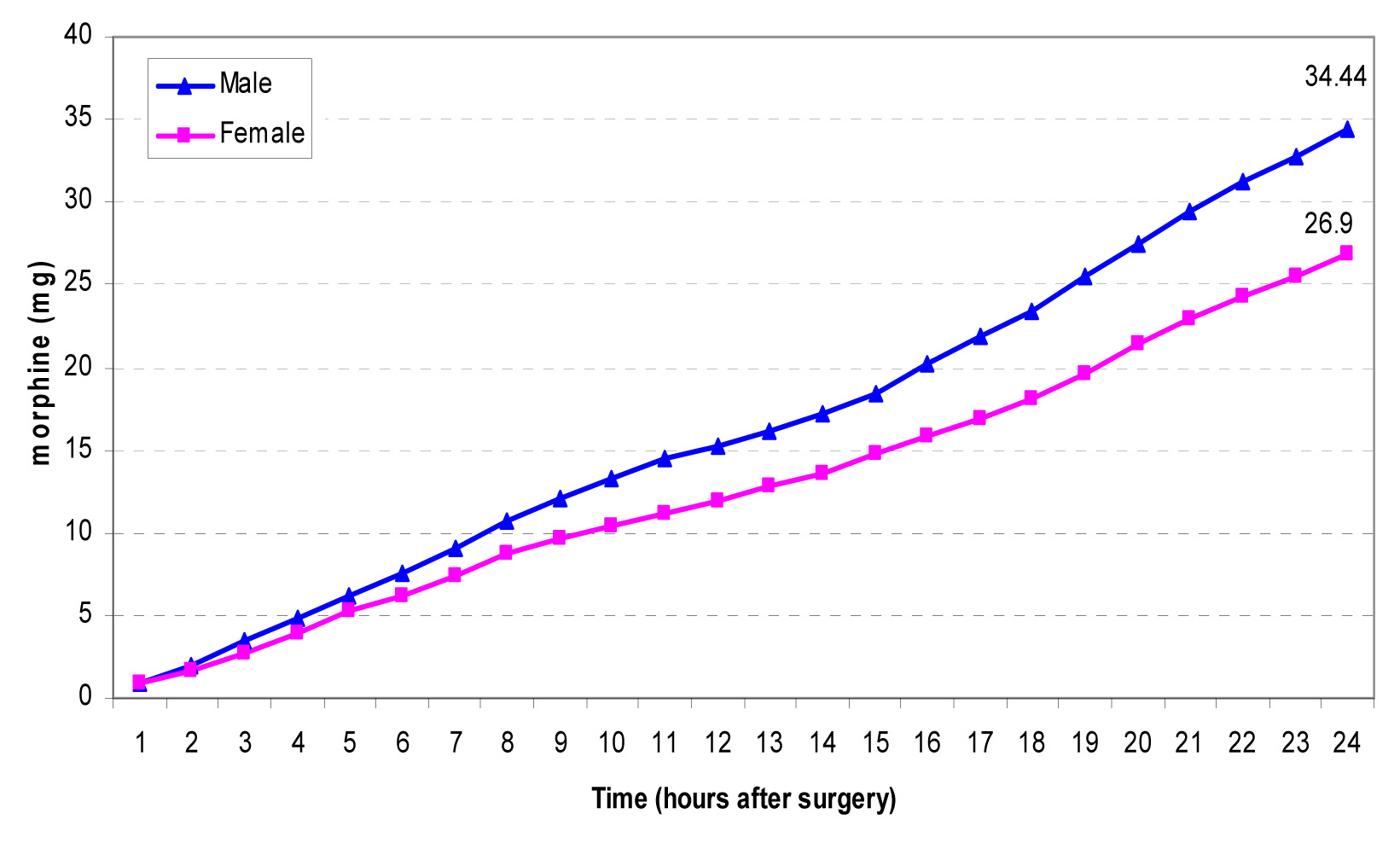
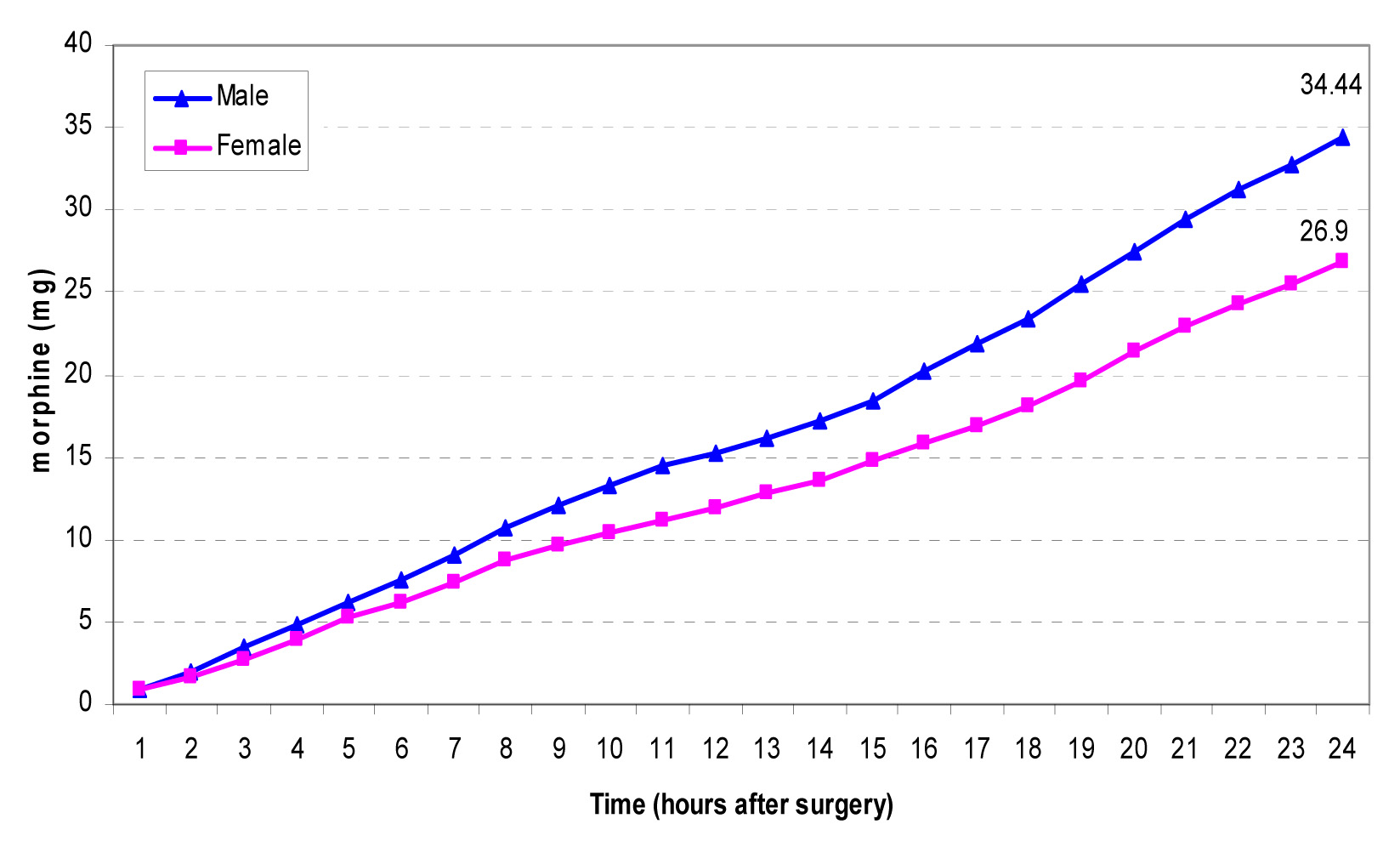
Results: During the first 24 h, males consumed significantly higher amount of morphine (34.35 ± 6.68 mg) when compared to females (26.78 ± 7.14 mg), p < 0.001.
Conclusion: We conclude that men require more morphine in the postoperative period than women.
Morphine, Patient-controlled analgesia, Postoperative pain
Introduction
Postoperative pain has adverse effects on the patients hemodynamic, metabolic and endocrine systems. As being more patients with co-morbidities are undergoing surgeries and more extensive and complicated procedures are involved it would require a stress free environment in the post-operative period to avoid any additional morbidity and mortality in the perioperative period. A smooth transition during the perioperative period without any cardio-respiratory and metabolic consequences of major surgery is the main goal of perioperative management. Adequate analgesia to alleviate pain is one of the important parts of postoperative management. Assessment and treatment of postoperative pain needs individualized approach as it is difficult to have uniform protocols as pain sensitivity differs among individuals. Analysing the factors which would predicts pain sensitivity and pain behavior might help in managing the postoperative pain. Various factors influence the analgesic requirements in the post operative period [1]. Age, weight, height, body mass index, sex, type of surgery, surgery site, preoperative pain and pain medication could influence the needed analgesics to maximize the pain relief while minimizing the serious adverse effects like respiratory depression. Analgesics have wide inter individual variation particularly opioids. This would preclude the fixed dose prescription for analgesia. PCA has been instrumental in individualizing the pain management in the post operative period and proved to be safe and effective [2,3]. PCA also enabled clinicians to analyse the post operative pain, assess the analgesic requirements and effective analgesia. Recent systematic review [4] on the predicting factors for postoperative pain and analgesic consumption showed preoperative anxiety; age, preoperative pain and type of surgery influenced the analgesic consumption. Gender was not a consistent predictor in their review. But the numbers of quality studies particularly the clinical studies are limited to analyse. Based on this qualitative systematic review, this study tried to address the gender influences on the analgesic consumption.
Women are more prone for clinical pain conditions and likely to get more pain following surgery and procedures than men. Chronic pain conditions occur more frequently in the female gender. Fibromyalgia, headache and migraine, rheumatoid arthritis, temparo mandibular pain conditions are more common in females. A combination of multiple biological and psychosocial factors plays a role in these gender differences. Genetic factors include a subset of genes that modulate the proteins involved in pain perception, pain pathway, analgesic metabolism, transport and receptor signaling. Apart from the sex dependant factors like lean body mass and water composition, there are receptor density; cytochrome enzymes, cyclical hormonal changes could potentially influence the pharmacokinetics and pharmacodynamics of any drug. There are lot of research about these differences which stresses that female gender should be adequately included in any drug trials before drawing any conclusions on efficacy and adverse effects [5]. Research into these receptor level experimental studies would give us the different sensitivities to different drugs. The contribution of each factor is not well defined but there is a strong relationship between gender on the pain perception and threshold. But only few studies have been done on humans. In all these studies, gender differences were not observed as primary focus of the study. We had designed our study primarily to study the influences of gender on the postoperative morphine consumption.
Materials and Methods
Four hundred and fifty ASA I & II patients of either sex, between the age group of 18-65 years undergoing elective intra abdominal surgeries under general anaesthesia were randomly recruited for the study. The patients were assigned into male (Group M, n = 231) or female (Group F, n = 219) groups. Informed consent was taken from all patients and the study was approved by the hospital ethics committee. Patients with history of bronchial asthma, chronic obstructive airway disease, and chronic pain on any drug or alcohol abuse were excluded from the study. Preoperative analgesic use, hormone therapy were excluded from the study population. All patients were given a detailed explanation about the usage of PCA pump (Graseby 3300, Herts, UK) and visual analog scale (100 mm-unmarked straight line, 0 corresponding to no pain and 100 to severe pain) [6]. Patients were premedicated with oral diazepam (0.2 mg/kg) on the night before surgery. In addition, intravenous morphine morphine (0.2 mg/kg) was given half an hour before surgery. General anaesthesia was induced with propofol (2mg/kg) and tracheal intubation was accomplished with vecuronium bromide (0.1 mg / kg). Anaesthesia was maintained with isoflurane (1 to 1.5%) in 66% nitrous oxide and 33% oxygen. Morphine (0.05 mg/kg) was administered intravenously during induction and 0.02 mg/kg top ups were given every hour. Intraoperative haemodynamic parameters were maintained within 20% range of the preoperative value. Intra operatively hemodynamic fluctuations requiring hemodynamic support and who required postoperative ventilator support were excluded. Operative time required more than 4 h was excluded from the study population. At the end of surgery, residual neuromuscular block was reversed with a mixture of neostigmine (0.05 mg/kg) and glycopyrrolate(0.01 mg/kg). All patients were shifted to postoperative recovery unit once they were fully awake and alert and were continuously monitored for 24 hour.
Postoperatively, when the patients were awake, VAS score was evaluated. A loading dose of morphine was given in incremental doses of 1 mg every 5 min till the VAS score reached ≤30. The dose of morphine required to reduce the VAS score to ≤30 was recorded. Subsequently, PCA pump was configured to deliver a bolus of 1 mg with a lock-out period lasting for 5 min. VAS score was recorded at every 2 h till the first 8 h and subsequently at 4 hourly intervals till 24 h. Heart rate, respiratory rate, and oxygen saturation were continuously monitored while non-invasive blood pressure was recorded at half-hourly intervals. At the end of 24 h, total morphine consumption (excluding the loading dose) and number of good demands and bad demands were retrieved on hourly basis from the infusion pump history panel.
Statistical Analysis
SPSS software (version 17) was used for statistical analysis. Demographic data was analysed with two tailed unpaired student t-test. Within group comparisons were done by using one-way-ANOVA test and Tukey’s honestly significant difference test. Non parametric data were analysed by Mann-Whitney U Test. Group mean was expressed as mean +/- 2SD. p value < 0.05 was considered as significant.
Results
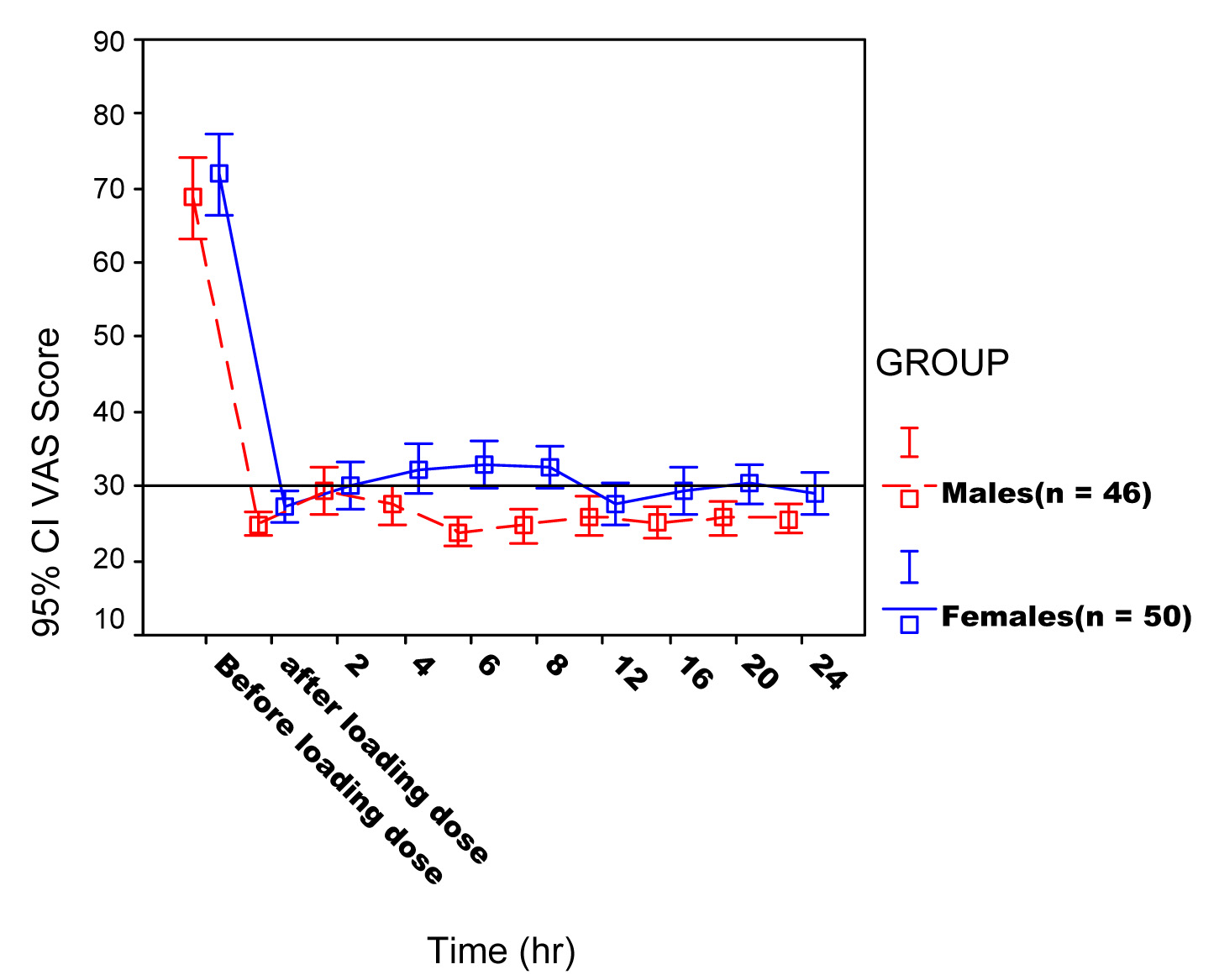
Demographic and anthropometric variables including lean body mass were comparable between the groups [Table/Fig-1]. VAS score was significantly higher among females throughout the first postoperative day. But the mean VAS score was around 30. The loading dose needed to bring down the pain scores to VAS ≤ 30 ranged between 2 – 8 mg with a mean of 4.09 ± 1.44 mg in males and 3.8 ± 1.67 mg in females (p = 0.37) [Table/Fig-2]. The VAS scores remained at a satisfactory level below 35 in both groups throughout the study period [Table/Fig-3]. Though the pain relief was satisfactory in both the groups, the mean VAS score was higher in females. The mean hourly demand delivery ratio for males was 1.84 ± 1.65 and 1.65 ± 1.22 for females. In males, the consumption in the first 24 h ranged from 21 to 59 mg with a mean of 34.35± 6.68 mg. In females, this varied between 13 to 58 mg with a mean of 26.78± 7.14 mg [Table/Fig-4] (p<0.001). To assess the influence of site of surgery with the consumption pattern, the patients who underwent upper abdominal procedures were separated out and the morphine consumption was compared between the groups. This also showed a similar pattern of consumption and a significant difference (p < 0.001) between the groups [Table/Fig-5].
| Demographic Data | Male | Female |
|---|
| Age (years) | 46.59 ± 12.72 | 40.20 ± 10.42 |
| Weight (kg) | 43.74 ± 7.47 | 50.54 ± 11.81 |
| Duration of surgery (min) | 140.22 ± 74.94 | 125.70 ± 67.29 |
| Type of surgery (%) | | |
| Upper abdominal | 68.4% | 46% |
| Lower abdominal | 31.6% | 54% |
Values = Mean ± SD
Morphine consumption during the first 24 hours postoperative period Values = Mean ± SD
| Male | Female | ‘p’ value |
|---|
| Loading dose morphine (mg) | 4.09 ± 1.44 | 3.8 ± 1.67 | 0.37 |
| Total morphine consumption (mg) | 34.35 ± 6.68 | 26.78 ± 7.14 | <0.001 |
VAS score comparison between males and females over 24 hours
Mean cumulative morphine consumption
Morphine consumption in upper abdominal surgeries
Discussion
In our study we found a significant difference in the postoperative morphine requirements between males and females. The morphine consumption was higher in males than females. Burns et al., [7] found the median 24 hour morphine consumption was 71.4 mg in males and 48.8 mg in females. With that they had found the median pain scores were below 30 in both groups and were comparable also. In our study the mean pain scores were ≤ 30 in both groups even though it was slightly higher in the female group which was statistically significant. This difference cannot be attributed to the difference in total consumption because we believe the VAS scores ≤ 30 is indicative of adequate pain relief. The total consumption in our study was lower than their study in both groups. This may be due to the higher doses of morphine, which we used for intraoperative analgesia and in addition to that we excluded the loading dose. Ethnic influences in the postoperative morphine consumption that may be another reason for this difference. So, ethnic influences can be a contributing factor because our patient’s requirements were comparable with the Asian studies conducted on Chinese patients by Tsui et al., [8] and Chia et al., [9]. Tsui et al., had found that the mean morphine consumption in the first 16 h and 17-41 h postoperatively were 25.7 and 17.8 mg respectively. This dose was comparable with our study. They also found higher consumption in males than females. Chia et al., had found that gender was a predictive factor for postoperative morphine consumption. They found that the mean consumption in males was 18.9 ± 8.9 mg with 15.3 ± 8.8 mg in females in the first postoperative day. Their results showed higher consumption in males which was similar as in our study but the total consumption was lower than our study. Another study done on two hundred patients showed morphine requirements were 23.2 mg for the first 12 h, 22.2 mg for the next 12 h and 16 mg for the last 12 h. Female patients required significantly less morphine than male. Interestingly such difference was no more present for patients older than 60 y [10]. Study by Auburn F et al., [11] with 4,317 patients, intravenous morphine titration was administered as a bolus of 2 (body weight < or= 60 kg) or 3 mg (body weight > 60 kg) during the immediate postoperative period at 5 minutes interval. The mean morphine dose required to obtain pain relief was 11.9 +/- 6.8 mg. Women had a higher initial VAS score and required a greater dose. In contrast, no significant difference was noted in elderly (aged > 75 y) patients. They concluded women had more pain required more analgesics but this difference disappeared in later age. This is in contrary to our studies. The reason for the gender differences in morphine requirements may be explained by several factors. The increased consumption in males can be due to the reluctance in the use of PCA in women. The education level also may be higher in men when compared to women. These factors should be considered in future studies.
Several studies identified women reports more pain than men. We found the initial VAS score was significantly higher and the mean VAS score throughout the first postoperative period among females rated higher than males. But the vas scores were clinically acceptable in both groups. Numerous studies done on healthy subjects with experimental pain as well as clinical studies, supports our study. Women reported more pain when venipuncture pain was compared and it correlated with estrogen and progesterone levels positively [12]. Healthy volunteers, when injected hypertonic saline in the tibial muscle women reported more pain for long duration [13]. The increased pain sensitivity among females could be due to gonadal hormones, neurophysiologic differences among gender. Testosterone appears to provide better tolerance to pain. These differences are not only limited to the biological variations but the socio cultural factors could play a role. Generally women express pain without any inhibition contrary to the masculine gender as their gender role allows it [14]. So they reported more pain than men, though the consumption was lower than men.
Studies have shown that the difference in gender was not particular to morphine analgesia. The opioid agonist-antagonist pentazocine, nalbuphine and butorphanol which acts predominantly at kappa-receptors, produced significantly better postoperative analgesia in females than in males, probably reflecting a difference in kappa-opioid-activated endogenous pain modulating circuits among gender [15]. Significant differences were found in the morphine induced respiratory depression between males and females [16]. Women appear to be more susceptible of nausea and vomiting following opioids analgesics [17]. Women are more sensitive to neuromuscular blocking drugs [18]. Contrary to this men are more sensitive to propofol [19]. Patient sex is an independent factor influencing the response to anaesthesia and recovery after surgery. Women emerged faster from general anaesthesia but their overall quality of recovery was poorer. Female sex hormones, particularly progesterone, might be involved, with premenopausal women having faster recovery time but poor overall recovery [20].
The neurophysiological mechanisms behind the gender differences are studied. Estrogen modulates central pain circuits involving migraine, trigeminal neuralgia and Fibromyalgia. Estrogen stimulates tryptophan hydroxylase, an enzyme which produces serotonin, an implicated neurotransmitter in migraine [21]. Estrogen receptors activate MAPK/ERK signaling pathway that mediates nociceptive processing in trigeminal nucleus caudalis. Carpous callosum thickness, preoptic hypothalamic area, planum temporal showed different size and morphology among gender [22]. Studies using Positron emission tomography with H2O showed varying cerebral blood flow and glucose utilization processing areas in brain [23]. The differences on the pain perception could be explained by this varying activation of forebrain structures to the stimulus among both sexes.
A detailed research will guide gender specific approaches in pain management. Newer drugs modalities on pain management will appear bearing these in mind. This knowledge could be applied in choosing the right modality of pain management. Also, right drug in right dosages would ensure good analgesic management with fewer side effects as well. The limitation on our study what we found was, we did not have a psychological stress analysis before the surgery which is a strong predictor of postoperative pain severity with a gender difference. The gender difference can be at all levels: pharmacokinetic; pharmacodynamic; social; cultural. So, gender has to be considered as an important influencing factor when the postoperative analgesia is being prescribed.
Conclusion
In summary, analgesic consumption in the post operative period showing definite gender difference with female gender having higher analgesic response than the male counterparts. This was confirmed with the adjusted lean body mass difference between the groups. This again stresses the pharmacokinetic and pharmacodynamic differences results from genetic, hormonal and receptor level rather simply to put on the lower lean body mass.
Values = Mean ± SD
[1]. Glasson JC, Sawyer WT, Lindley CM, Ginsberg B, Patient-specific factors affecting patient-controlled analgesia dosingJ Pain Palliat Care Pharmacother 2002 16(2):5-21. [Google Scholar]
[2]. Barros GA, Lemonica L, Patient controlled analgesia in a university hospitalRev Bras Anestesiol 2003 53(1):69-82. [Google Scholar]
[3]. De Kock M, Scholtes JL, Postoperative P.C.A. in abdominal surgery. Analysis of 200 consecutive patientsActa Anaesthesiol Belg 1991 42(2):85-91. [Google Scholar]
[4]. Hui Yun Vivian Ip, Abrishami Amir, Philip WH Peng, Jean Wong, Frances Chung, M.D., F.R.C.P.C, Predictors of Postoperative Pain and Analgesic Consumptio. A Qualitative Systematic ReviewAnaesthesiology 2009 111:657-77. [Google Scholar]
[5]. Rosseland LA, Stubhaug A, Gender is a confounding factor in pain trials: women report more pain than men after arthroscopic surgeryPain 2004 112(3):248-53. [Google Scholar]
[6]. Hawker GA, Mian S, Kendzerska T, French M, Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP)Arthritis Care Res 2011 63:S240-52. [Google Scholar]
[7]. Burns JW, Hodsman NB, McLintock TTC, Gillies GW, Kenny GN, McArdle CS, The influence of patient characteristics on the requirements for postoperative analgesia. A reassessment using patient-controled analgesiaAnaesthesia 1989 44(1):2-6. [Google Scholar]
[8]. Tsui SL, Tong Wn, Irwin M, The efficacy, applicability and side –effects of postoperative intravenous patient-controlled morphine analgesia: an audit of 1233 Chinese patientsAnesthIntens Care 1996 24:658-64. [Google Scholar]
[9]. Chia YY, Chow LH, Hung CC, Liu K, Ger LP, Wang PN, Gender and pain upon movement are associated with the requirements for postoperative patient-controlled i.v. analgesia: a prospective survey of 2,298 Chinese patientsCan J Anesth 2002 49(3):249-55. [Google Scholar]
[10]. Macintyre PE, Jarvis DA, Age is the best predictor of postoperative morphine requirementsPain 1996 64(2):357-64. [Google Scholar]
[11]. Aubrun F, Salvi N, Coriat P, Riou B, Sex- and age-related differences in morphine requirements for postoperative pain reliefAnaesthesiology 2005 103(1):156-60. [Google Scholar]
[12]. Ring C, Veldhuijzen van Zanten JJ, Kavussanu M, Effects of sex, phase of the menstrual cycle and gonadal hormones on pain in healthy humansBiol Psychol 2009 81(3):189-91. [Google Scholar]
[13]. Lei J, You HJ, Variation of pain and vasomotor responses evoked by intramuscular infusion of hypertonic saline in human subjects: influence of gender and its potential neural mechanismsBrain Res Bull 2012 87(6):564-70. [Google Scholar]
[14]. Wise EA, Price DD, Myers CD, Heft MW, Robinson ME, Gender role expectations of pain: relationship to experimental pain perceptionPain 2002 96:335-42. [Google Scholar]
[15]. Gear RW, Miaskowski C, Gordon NC, Paul SM, Heller PH, Levine JD, Kappa-opioids produce significantly greater analgesia in women than in menNat Med 1996 2(11):1248-50. [Google Scholar]
[16]. Cepeda MS, Farrar JT, Baumgarten M, Boston R, Carr DB, Strom BL, Side effects of opioids during short-term administration: effect of age, gender, and raceClin Pharmacol Ther 2003 74(2):102-12. [Google Scholar]
[17]. Bijur PE, Esses D, Birnbaum A, Chang AK, Schechter C, Gallagher EJ, Response to morphine in male and female patients: analgesia and adverse eventsClin J Pain 2008 24(3):192-98. [Google Scholar]
[18]. Adamus M, Gabrhelik T, Marek O, Influence of gender on the course of neuromuscular block following a single bolus dose of cisatracurium or rocuroniumEur J Anaesthesiol 2008 25(7):589-95. [Google Scholar]
[19]. Wilhelm W, Buchinger H, Biedler A, Altmann S, Larsen R, Kreuer S, Influence of gender on propofol consumption and recovery timesAnaesthesist 2005 54(6):567-74. [Google Scholar]
[20]. Buchanan FF, Myles PS, Cicuttini F, Effect of patient sex on general anaesthesia and recoveryBr J Anaesth 2011 106(6):832-39. [Google Scholar]
[21]. Gupta S, McCarson KE, Welch KM, Berman NE, Mechanisms of pain modulation by sex hormones in migraineHeadache 2011 51(6):905-22. [Google Scholar]
[22]. Allen LS, Richey MF, Chai YM, Gorski RA, Sex differences in the corpus callosum of the living human beingJ Neurosci 1991 11(4):933-42. [Google Scholar]
[23]. Casey KL, Minoshima S, Morrow TJ, Koeppe RA, Comparison of human cerebral activation pattern during cutaneous warmth, heat pain, and deep cold painJ Neurophysiol 1996 76(1):571-81. [Google Scholar]