Acute Pelvic Pain: A Ball Pen May Be a Cause?
Garjesh Singh Rai1, Rakesh Roshan2, Radha Sarawagi3, Mahendra Mohan Vyas4, Deepak Goel5
1 Associate Professor, Department of Radiodiagnosis, Peoples College of Medical Science and Research CentreBhopal, Madhya Pradesh, India.
2 Post Graduate Student, Department of Radiodiagnosis, Peoples College of Medical Science and Research CentreBhopal, Madhya Pradesh, India.
3 Professor, Department of Radiodiagnosis, Peoples College of Medical Science and Research CentreBhopal, Madhya Pradesh, India.
4 Assistant Professor, Department of Radiodiagnosis, Peoples College of Medical Science and Research CentreBhopal, Madhya Pradesh, India.
5 Post Graduate Student, Department of Radiodiagnosis, Peoples College of Medical Science and Research CentreBhopal, Madhya Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Radha Sarawagi, Professor, Department of Radiodiagnosis, Peoples College of Medical Science and Research Centre, Bhanpur Road, Bhopal, Madhya Pradesh, India.
Phone: +919644606316,
E-mail: radhasanjeevgupta@gmail.com
Chronic Urinary tract infection (UTI) is a common problem in women and can be seen without any significant anatomical and functional pathology. Foreign bodies within the urinary bladder are not rare and should be considered as a cause of chronic and recurrent UTI. Intravesical foreign bodies can be self inflicted, iatrogenic or migration from adjacent organs. History in these cases is often misleading and presentation of foreign body mostly becomes apparent as suprapubic pain, dysuria with or without hematuria. We present a case of self-inflicted foreign body within the bladder of a young female who presented with recurrent urinary tract infections for six months that did not respond to medical treatment.
Computed tomography, Foreign body, UTI, Urinary bladder, Ultrasonography
Case Report
An 18-year-old young unmarried female presented with the complaints of severe lower abdominal pain, dysuria and mild fever. On physical examination patient was febrile and restless with mild suprapubic tenderness. No other findings were detected per abdominal examination.
Plain radiograph of abdomen was performed which showed two metallic density foreign bodies in the pelvic region, of which one was smaller & pointed and other was larger and tubular. A low density linear object was seen lying obliquely in the pelvis and appeared to be aligned with the smaller foreign body [Table/Fig-1]. Transabdominal sonography was performed which revealed a 6.3cm long tubular object [Table/Fig-2a] in the bladder lumen which was lying obliquely. The tip of the object was hyperechoic and appeared impacted in the right lateral bladder wall. Remaining part of the object was isoechoic with smooth margins. Another hyperechoic object was noted in dependent portion of bladder lumen on left side with posterior acoustic shadowing [Table/Fig-2b]. Innumerable low level floating echoes were noted in distended urinary bladder with thickened and irregular posterior wall. Plain CT scan of lower abdomen [Table/Fig-3a&b] showed a long tubular low density structure lying obliquely in the bladder lumen with high density pointed tip. The shape of the structure resembled a ball point pen. Other high density tubular foreign body was noted at dependent part resembling the cap of pen. Pointed tip had invaded the right posterolateral wall of bladder with subsequent focal thickening. Cystoscopic removal of foreign body has been performed and a ball pen and its cap have been taken out without any surgical or post surgical complication.
Plain radiograph of pelvis shows two metallic density foreign bodies in the pelvic region, of which one was smaller and pointed (arrowhead) and other was larger and tubular (arrow). A low density linear object (red arrow) was seen lying obliquely in the pelvis and appeared to be aligned with the smaller foreign body

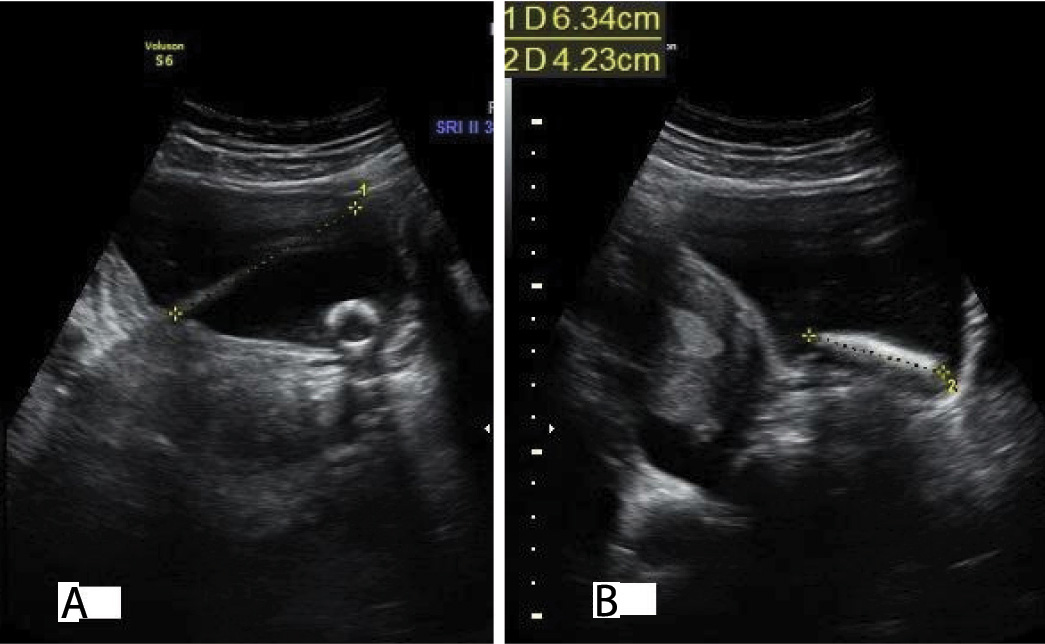
Sonography of urinary bladder in oblique transverse section (A) shows an obliquely lined echogenic foreign body of 6.3 cm in length with impacted tip in bladder wall. Sonography of urinary bladder in sagittal section (B) shows an echogenic foreign body of 4.2 cm length at dependent position of lumen.
Oblique sagittal plain computed tomography scan (A) reveals a linear object (arrow)within the urinary bladder with hypodensity at the superior half, isodensity at the inferior half and metallic density pointed tip (arrowhead) indenting the bladder wall. Coronal computed tomography scan through posterior part of urinary bladder (B) showing a tubular metallic density structure resembling a cap of ball pen (arrowhead)

Discussion
Foreign body in urinary tract is not uncommon however data regarding exact incidence of occurrence in India or worldwide is not available. Only single case reports or case series are available in medline search. Rafique M in Urol J reported 17 cases of intravesical foreign body over five years [1].
Self inflicted foreign bodies in urinary bladder rarely present directly; rather they present with lower urinary tract symptoms like dysuria, lower abdominal pain with or without fever. One major difficulty in the early diagnosis is due to patients who choose to ignore the insertion of foreign body because of embarrassment [2]. There is often misleading history of trauma or other stories. In our case the patient gave history of oral ingestion of ball pen six months ago. In adults, urethral self insertion of foreign body is usually done for erotic stimulation or is done by mentally retarded person. Curiosity and inquisitiveness are the main cause for urethral insertion of foreign body in childhood [3]. The list of foreign body contains almost every conceivable object including wires, screws, pencils, hairpin, matchsticks, pen, fruit kerels, fish hooks, drinking straw, nails, rifle bullet, chew gum, snake, razor blade, wrist watch, etc [4,5]. Aetiology of foreign body in the bladder may be classified as insertion of foreign body by the person him/her self, iatrogenic (penetration during surgery of urinary tract, uterus, vagina and abdomen) or migration from adjacent organs (intrauterine devices). In some cases the foreign body was inserted to urethra to prevent conception [5]. The duration of symptoms before diagnosis ranged from weeks to few months and the interval between insertion and removal of foreign body ranged from month to few years [4]. Complication of foreign body in lower urinary tract includes infection, abscess, extravasation, diverticuli, perforation, fistula formation and stone formation however serious life threatening complications are uncommon. Ito et al., [6] reported a case of intravesical foreign body with vesical rupture and peritoneal invasion. Priapism is also been reported in few cases [7]. The diagnosis of foreign body in urethra and bladder is usually based on clinical history and imaging. When the foreign body is radio-opaque, diagnosis can be established by pelvic radiograph, sonography and computed tomography, and radiolucent object can be identified by Ultrasonography and MRI. Intravesical foreign body was more commonly reported in female possibly due to short urethra. Bladder foreign body creates challenge to urologist that needs an urgent management. The suitable method for extraction of intravesical foreign body depends on the size, shape and age of the patient and associated complications [1]. A minimal invasive surgery like cystoscopy with biopsy forceps is suitable method in most of the cases however open surgery may be required in cases of large impacted foreign bodies, complications like perforation of bladder wall or fistula formation. Injuries of urethra must be avoided especially in case of large object [8]. Percutaneous suprapubic retrieval under direct visualization via cystoscopy is an alternative [9]. Some authors suggest this technique in children [10]. Open removal via suprapubic cystostomy and vesicular exploration is most invasive, but required for large, impacted, and lacerating objects.
Conclusion
Foreign body in the urinary bladder could manifest with various symptoms and signs and history is often misleading. When a patient presents with complaints of lower abdominal pain, dysuria, fever and other urinary symptoms, we should also consider foreign body as a causative agent especially when patient is suffering from psychiatric problem or belonging to adolescent age group. X-ray and USG are basic and appropriate diagnostic tools for early detection however CT scan and MRI can be performed for detailed investigations and complications arising from foreign body.
[1]. Rafique M, Intravesical foreign bodies: review and current management strategiesUrol J 2008 5(4):223-31. [Google Scholar]
[2]. Ashworth SW, Hurtado TR, Cuenca PJ, Wedmore I, Kang CS, Puzzling groin pain in a 15 year-old boyJ Emerg Med 2005 28(1):83-85. [Google Scholar]
[3]. Mukerji G, Rao AR, Hussein A, Motiwala H, Self-introduction of foreign body into urinary bladderJ Endourol 2004 18(1):123-25. [Google Scholar]
[4]. Osca JM, Broseta E, Server G, Ruiz JL, Gallego J, Jimenez-Cruz JF, Unusual foreign bodies in the urethra and bladderBr J Urol 1991 68(5):10-12. [Google Scholar]
[5]. Khan Ali S, Kaiser CW, Dailey B, Krane R, Unusual foreign body in the urethraUrol Int 1984 39(3):184-86. [Google Scholar]
[6]. Ito H, Ninomiya A, Furuuchi J, A case of intravesical foreign body with a vesical rupture invading the peritoneal cavity: a case reportHinyokika Kiyo 2009 55(7):425-27. [Google Scholar]
[7]. Wenderoth U, Jonas U, Curiosity in urology? Masturbation injuriesEur Urol 1980 6(5):312-13. [Google Scholar]
[8]. Irekpita E, Imomoh P, Kesieme E, Onuora V, Intravesical foreign bodies: a case report and a review of the literatureInt Med Case Rep J 2011 4:35-39. [Google Scholar]
[9]. Georgius P, A novel method to remove an unusual foreign body (Blu-Track)BJU Int 2000 86(6):749-50. [Google Scholar]
[10]. Hutton KA, Huddart SN, Percutaneous retrieval of an intravesicular foreign body using direct transurethral visualization: a technique applicable to small childrenBJU Int 1999 83(3):337-38. [Google Scholar]