Dermatoglyphics and Karyotype Analysis in Primary Amenorrhoea
Shweta S Talhar1, Bharat R Sontakke2, Jwalant E Waghmare3, Aditya M Tarnekar4, Moreshwar R Shende5, Asoke K Pal6
1 Assistant Professor, Department of Anatomy, Mahatma Gandhi Institute of Medical Sciences, Sevagram, Wardha, Maharashtra, India.
2 Assistant Professor, Department of Anatomy, Mahatma Gandhi Institute of Medical Sciences, Sevagram, Wardha, Maharashtra, India.
3 Associate Professor, Department of Anatomy, Mahatma Gandhi Institute of Medical Sciences, Sevagram, Wardha, Maharashtra, India.
4 Professor, Department of Anatomy, Mahatma Gandhi Institute of Medical Sciences, Sevagram, Wardha, Maharashtra, India.
5 Professor & Head, Department of Anatomy, Mahatma Gandhi Institute of Medical Sciences, Sevagram, Wardha, Maharashtra, India.
6 Professor, Department of Cytogenetics, Mahatma Gandhi Institute of Medical Sciences, Sevagram, Wardha, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shweta S. Talhar, Assistant Professor, Department of Anatomy, Mahatma Gandhi Institute of Medical Sciences, Sevagram, Wardha-442102, Maharashtra, India. Phone : 09604232792, E-mai : Shweta@mgims.ac.in
Background: Dermatoglyphics is the scientific study of the skin ridge patterns on the fingers, toes, palms of the hands and soles of feet. Dermatoglyphics is in use as a supportive diagnostic tool in genetic or chromosomal disorders as well as in clinical conditions with genetic etiologies. Primary amenorrhoea and Dermatoglyphics, both have the suspected multifactorial (genetic and environmental) aetiologies.
Objective: In the present study the finger dermatoglyphic patterns were studied in primary amenorrhoea cases and age matched fertile control females and also attention was given to find out whether a specific dermatoglyphic trait exists in primary amenorrhoea cases and whether it was statistically significant.
Materials and Methods: To study the role of dermatoglyphics in primary amenorrhoea, a study was conducted on 30 subjects with primary amenorrhoea (as cases) and compared it with equal number of age matched fertile females (as controls). We studied fingertip patterns in all the subjects enrolled. Simultaneously we have assessed the Karyotype of primary amenorrhoea cases.
Result and Conclusion: Two subjects in experimental group have shown abnormal Karyotypes. The most significant finding in present study was increased total finger ridge count (TFRC) in primary amenorrhoea cases which was statistically significant. We also found higher frequency of loops and arches in primary amenorrhoea with abnormal karyotypes. This type of study may be quite useful as a supportive investigation, in stating the predisposition of an individual to primary amenorrhoea and referral of an individual for karyotyping.
Dermatoglyphics, Karyotype, Primary amenorrhoea
Introduction
The term Dermatoglyphics has its origin from Greek words, derma means skin and glyphic means carvings [1]. The term was coined by Dr. Harold Cummins- the Father of Dermatoglyphics, at the University of Oklahoma in 1926. Dermal ridge differentiation takes place early in fetal development. The resulting ridge configurations are genetically determined and influenced or modified by environmental factors [2]. They are stable throughout life, unique to the individual and significant as a means of identification. Moreover, characteristic dermatoglyphic abnormalities have been reported in genetic disorders like Down’s syndrome [3], Klinefelter’s syndrome [4], breast cancer [5] etc. In down’s syndrome, mostly ulnar loop pattern was observed. Abnormal dermatoglyphic features such as simian crease, Sydney line, and patterns in the hypothenar and Interdigital areas have been observed more frequently in down’s syndrome [3]. In Klinefelter’s syndrome increased in whorls and decreased in loops was observed when study was conducted in six such patients [4]. A pattern of six or more digital whorls was identified more frequently in women with breast cancer than in those without the disease [5]. Dermatoglyphic study in children of oral cleft have showed increased frequency of ulnar loops [6]. When dermatoglyphic study was conducted on diabetic males, increased radial, ulnar loops and arches with decreased whorls were observed [7]. Finger tip study in students presented with extensive dental caries showed more whorls [8].
Dermatoglyphics is in use as a diagnostic tool in genetic or chromosomal disorders as well as in clinical conditions with genetic etiology. WHO Annual reports 1982 and 1985 have estimated that 15% of the human population is infertile and that amenorrhoea is the 6th major cause of female infertility [9]. So, the study was designed to see the dermatoglyphic pattern in primary amenorrhoea subjects and also to find out the dermatoglyphic pattern in primary amenorrhoea subjects who have abnormal karyotypes. Amenorrhoea and Dermatoglyphic patterns both have multifactorial determinants which can be broadly categorized as genetic and environmental [9]. In a number of diseases having a strong genetic basis dermatoglyphics may be a supportive diagnostic aid. Some of these genetic disorders like Turner’s syndrome and gonadal dysgenesis manifest with ‘primary’ amenorrhoea. Failure of onset of menstruation beyond the age of 16 y regardless of development of secondary sexual characters is called as primary amenorrhoea [10]. When there is absence of menstruation for six months or more following normal menstruation, it is called secondary amenorrhoea [11]. Our aim was to establish the relationship between primary amenorrhoea and Dermatoglyphics, due to their suspected genetic aetiology.
Materials and Methods
The present study was carried in the Department of Anatomy and Department of Obstetrics & Gynecology from January 2010 to August 2011. Thirty primary amenorrhoea subjects, from central Indian population with the age ranging from 17 to 25 y, were enrolled as ‘cases’ and thirty age matched fertile females as ‘controls’. For all the subjects informed consent was taken in their local language along with detailed history before starting the procedure. All the records were maintained.
Inclusion criteria
For ‘cases’: Female subjects of 17 to 25 y of age who presented themselves in Obstetrics/Gynecology OPD with the problem of failure to have onset of menses (primary amenorrhoea). All the subjects were referred from Obstetrics/Gynecology Department to the division of human cytogenetic for karyotyping.
For ‘controls’: Married females up to the age of 25 y who had given birth to at least one live child without the history of miscarriages or genetic abnormalities. All the subjects were examined by specialist and found healthy. The subjects were also not suffering from any known genetic or clinical disorders and were not on medication.
Cytogenetic analysis
All these 30 primary amenorrhoea subjects were also subjected for karyotyping in the division of human cytogenetic in the Department of Anatomy; Karyotypes were analysed by conventional Giemsa staining and G-banding by Trypsin and Giemsa (GTG) [12].
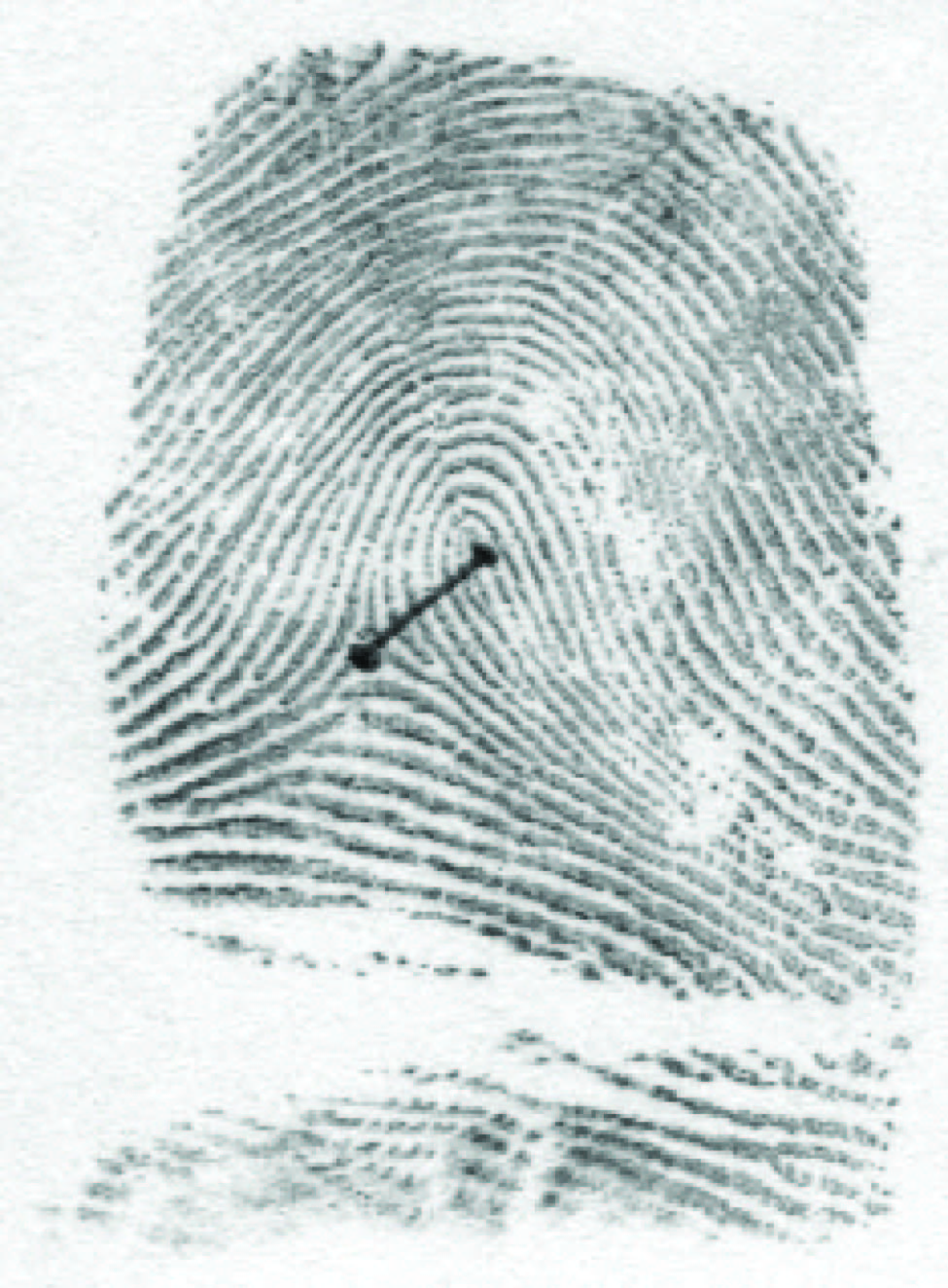
Method of dermatoglyphic recording: Ink method was selected in our study for dermatoglyphic analysis [13]. Palmar and each fingertip dermatoglyphic prints of control females as well as primary amenorrhoea females were taken by rolling the finger from radial to ulnar side to include whole of the patterns [Table/Fig-1&2]. Detailed dermatoglyphic analyses of the prints were done with the help of magnifying lens.
Dermatoglyphic print of fingertips of control female R1-WcR2-Lu R3-Lu R4-LuR5-Lu

Dermatoglyphic print of fingertips of primary amenorrhoea female R1-LUR2-WC R3-WC R4-WC R5-LU

Following parameters were studied:
Qualitative analysis of finger tip patterns (FTP).
Study of arches (arch plain/ arch tented) [Table/Fig-3a].
Study of loops (ulnar loop/ radial loop) [Table/Fig-3b&c].
Study of whorls (simple whorl / whorl composite) [Table/Fig-3d,e,f,g].
Quantitative analysis of finger tip patterns by doing finger ridge count (Total finger ridge count (TFRC) and Absolute finger ridge count (AFRC)).

Ulnar Loop(LU) Ridge counting done along the line,

Simple whorl (Spiral whorl-WS)

Simple whorl (Concentric whorl-WC)

Composite whorl (Central pocket loop)

Composite whorl (Lateral pocket loop)

Total Finger Ridge Count (TFRC): It includes the sum of ridge counts of all ten digits, where only the larger count is used on those digits with more than one ridge count. It expresses size of pattern.
Absolute finger Ridge Count (AFRC): The additions of the ridge counts from all the separate triradii on all ten digits are included in AFRC. It reflects the pattern size and pattern type also.
Statistical Analysis
statistical analysis was done by descriptive statistics and inferential statistics using Mann-Whitney U-Test and Chi-square test using statistical software SPSS Version 17.00 and Graphpad Prism four.
Results
The dermatoglyphic observations of finger tips of 30 control females and 30 primary amenorrhoea female subjects were analysed and recorded as per following details:
Basic finger tip patterns:
Control group
Loops: Loops were the most frequent pattern in controls. We found 202 loops out of 300 fingertips and the frequency was 67.33% [Table/Fig-4]. The proportion of ulnar loops to radial loops in control females was 199:3 [Table/Fig-5]. Thus there was increased percentage of total ulnar loops (66.33%) as compared to total radial loops (1%) in controls.
Whorls: In all controls the whorls were found to be the second in the descending order of frequency amongst digital patterns. 79 out of 300 fingertips of control females had whorls. The frequency was 26.33% in control females [Table/Fig-4]. The proportion of total simple whorl to total whorl composite in control females was 52:27 [Table/Fig-6]. Thus there was increased percentage of total simple whorl (17.33%) as compared to total whorl composite (9%) in controls.
Arches: In all control females arches were the least frequent pattern. 19 out of 300 fingertips of control females had arches. The frequency was 6.33% [Table/Fig-4]. The proportion of total arch plain to total arch tented in control females was 18:1 [Table/Fig-7]. Thus there was increased percentage of total arch plain (6%) as compared to total arch tented (0.33%) in controls.
Distribution of finger tip patterns on both hands in two groups
| 10 Finger average | TL% | TW% | TA% |
|---|
| CF(Rt+Lt)/2 | 67.33 | 26.33 | 6.33 |
| PAF(Rt+Lt)/2 | 63.33 | 33.99 | 2.67 |
Statistical analysis of loops
| Parameter | Controls (%) | Primary amenorrhoea subjects (%) | Chi Square | p-value |
|---|
| TUL | 199 (66.33%) | 186 (62%) | 0.34 | 0.55 NS, p>0.05 |
| TRL | 3 (1%) | 4 (1.33%) | 0.00 | 1.00 NS, p>0.05 |
| TL | 202 (67.33%) | 190 (63.33%) | 0.35 | 0.55 NS, p>0.05 |
Statistical analysis of whorls
| Parameter | Controls | Primary amenorrhoeasubjects (%) | Chi Square | p Value |
|---|
| TSW | 52 (17.33%) | 58 (19.33%) | 0.13 | 0.71,NS,p>0.05 |
| TWcomp | 27 (9%) | 44 (14.67%) | 1.70 | 0.19,NS,p>0.05 |
| TW | 79 (26.33%) | 102 (33.99%) | 1.52 | 0.21,NS,p>0.05 |
Statistical analysis of arches
| Parameter | Controls | Primary amenorrhoea subjects (%) | Chi Square | p Value |
|---|
| TAP | 18 (6%) | 8 (2.67%) | 1.04 | 0.30,NS,p>0.05 |
| TAt | 1 (0.33%) | 0 | 1.00 | 0.31,NS,p>0.05 |
| TA | 19 (6.33%) | 8 (2.67%) | 1.04 | 0.30,NS,p>0.05 |
Primary amenorrhoea subjects:
Loops: Loops were the most frequent pattern in primary amenorrhoea subjects (190/300). The frequency was 63.33% [Table/Fig-4]. The proportion of ulnar loops to radial loops in primary amenorrhoea females was186:4 [Table/Fig-5]. Thus, there was increased percentage of total ulnar loops (62%) as compared to total radial loops (1.33%) in cases.
Whorls: 102 out of 300 fingertips of 30 primary amenorrhoea subjects had whorls. The frequency was 33.99% [Table/Fig-4]. The proportion of total simple whorl to total whorl composite in primary amenorrhoea females was 58:44 [Table/Fig-6]. Thus there was increased percentage of total simple whorl (19.33%) as compared to total whorl composite (14.67%)
Arches: 8 out of 300 fingertips of 30 primary amenorrhoea subjects had arches. The frequency was 2.67% [Table/Fig-4]. The proportion of total arch plain to total arch tented in primary amenorrhoea females was 8:0 [Table/Fig-7]. Thus there was increased percentage of total arch plain (2.67%) as compared to total arch tented (0).
We observed decrease in total loops and total arches and increase in total whorls in primary amenorrhoea cases as compared to controls but the difference was found to be statistically insignificant [Table/Fig-8].
Statistical analysis of fingertip pattern
| Parameter (out of 300 fingertips) | Controls(%) | Cases (%) | Chi Square value | p Value |
| TL | 202 (67.33%) | 190 (63.33%) | 0.35 | 0.55, NS |
| TW | 79 (26.33%) | 102 (33.99%) | 1.52 | 0.21, NS |
| TA | 19 (6.33%) | 8 (2.67%) | 1.04 | 0.30, NS |
Comparative analysis of fingertip pattern between control females and primary amenorrhoea subjects:
Loops: Considering overall distribution of fingertip patterns, there was decreased percentage of total loops (TL- 63.33%) as well as total ulnar loops (TUL- 62 %) in primary amenorrhoea subjects as compared to that of control females (TL- 67.33% and TUL- 66.33%)[Table/Fig-4,5]. Whereas percentage of total radial loops (TRL-1.33 %) was increased in primary amenorrhoea subjects as compared to that of control females (TRL- 1%).
Whorls: Regarding overall distribution of whorls, it was observed that the percentage of total simple whorl (19.33%), total whorl composite (14.67%) and total whorls (33.99%) in primary amenorrhoea subjects were increased as compared to total simple whorl (17.33%), total whorl composite (9%) and total whorl (26.33%) in control females [Table/Fig-6].
Arches: When overall digital distribution of arches was analysed on both hands, we observed that total arch plain (2.67%), total arch tented (0) and total arches (2.67%) were decreased in primary amenorrhoea subjects as compared to total arch plain (6%), total arch tented (0.33%) and total arches (6.33%) of control females [Table/Fig-7].
Finger ridge count
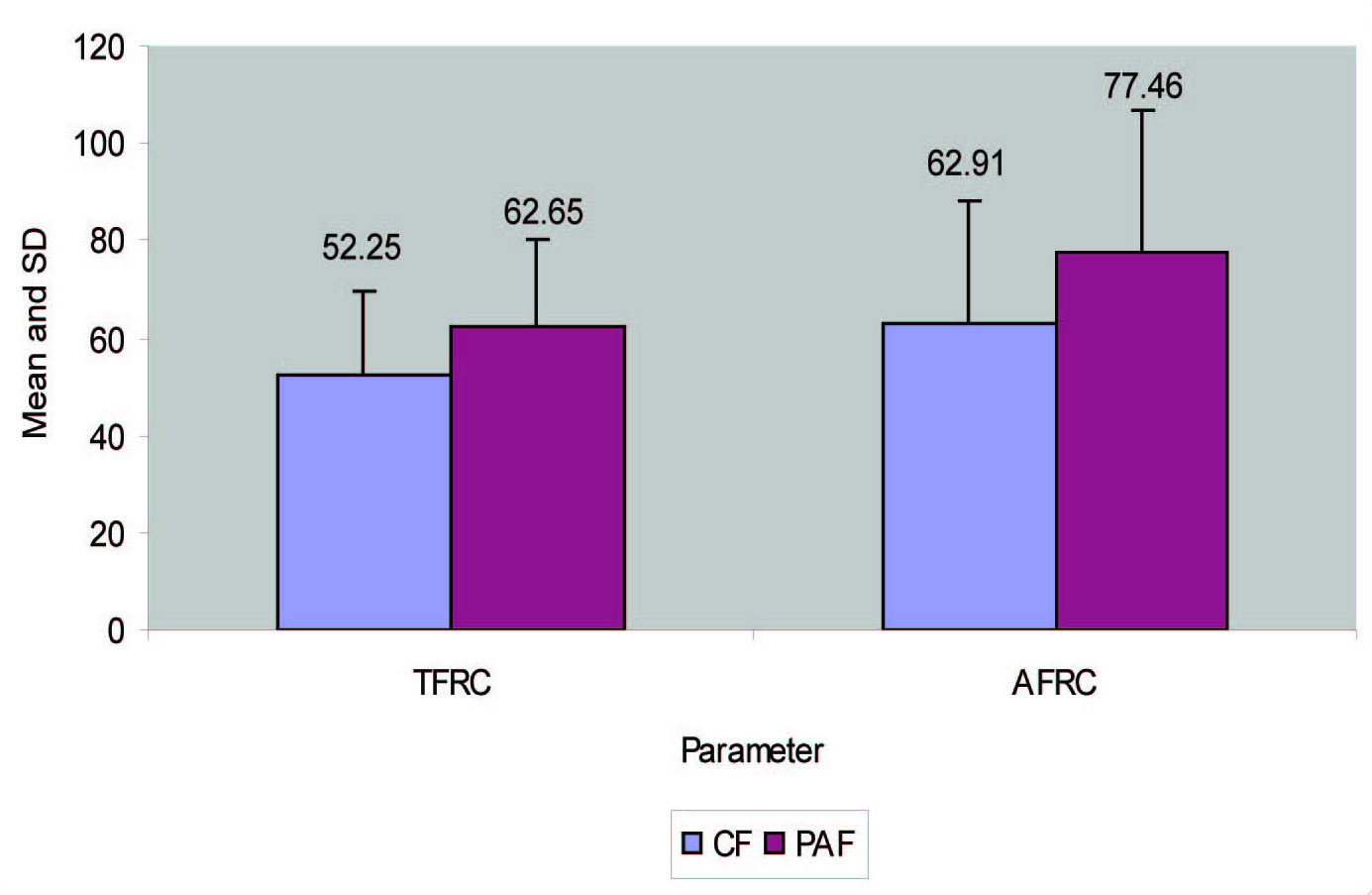
It was observed that the mean total finger ridge count (TFRC= 62.65) and absolute finger ridge count (AFRC= 77.46) in primary amenorrhoea subjects were increased when compared with the mean of TFRC (52.25) and AFRC (62.91) in control females. Increase in TFRC was found to be statistically significant [Table/Fig-9,10].
Statistical analysis of finger ridge count (TFRC and AFRC)
| Parameter | Controls | Cases | z Value | p- value |
|---|
| TFRC | 52.25 | 62.65 | 2.39 | 0.017,S |
| AFRC | 62.91 | 77.46 | 1.82 | 0.068,NS |
Total finger ridge count and absolute finger ridge count inprimary amenorrhoea and control females
Karyotype analysis (performed in ‘cases’ only)
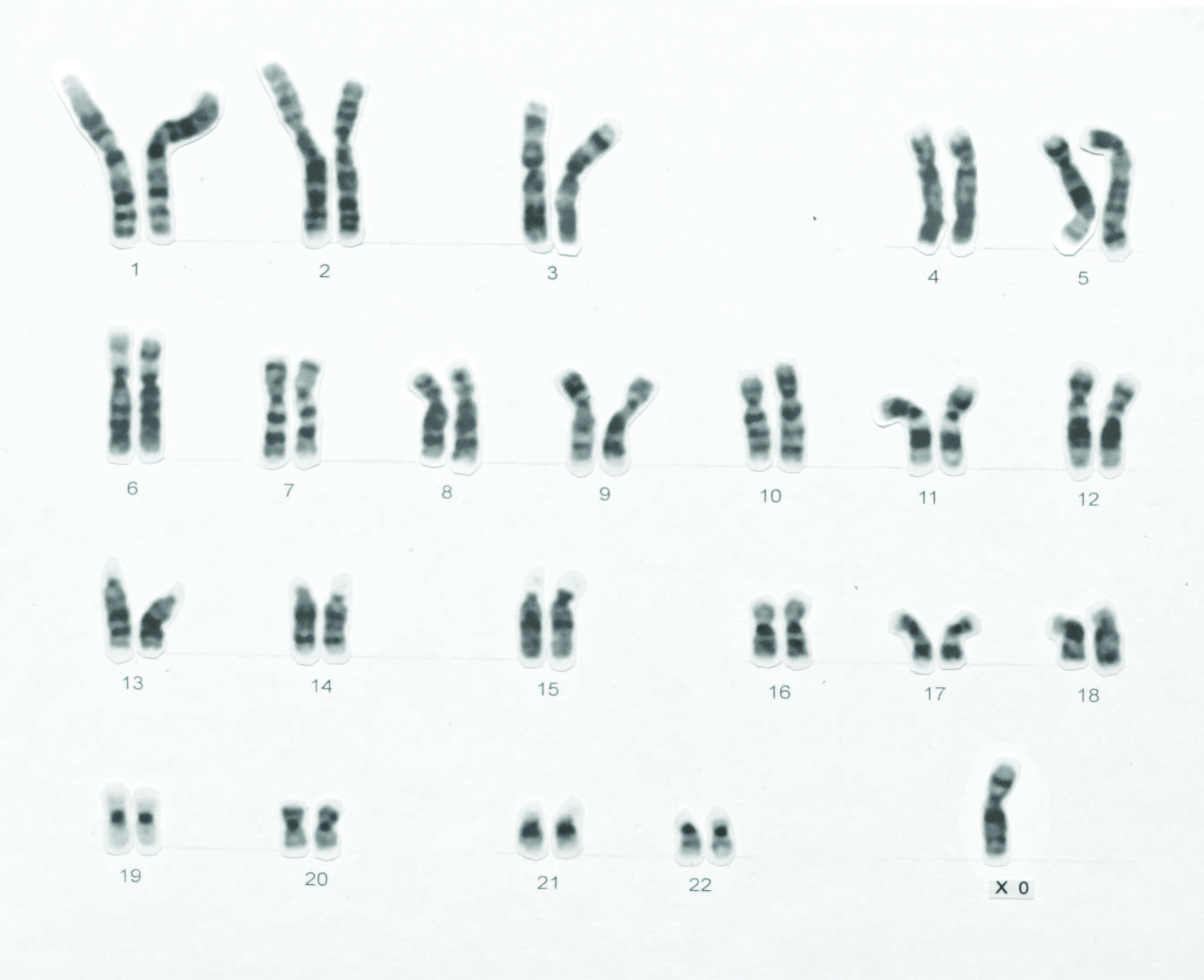
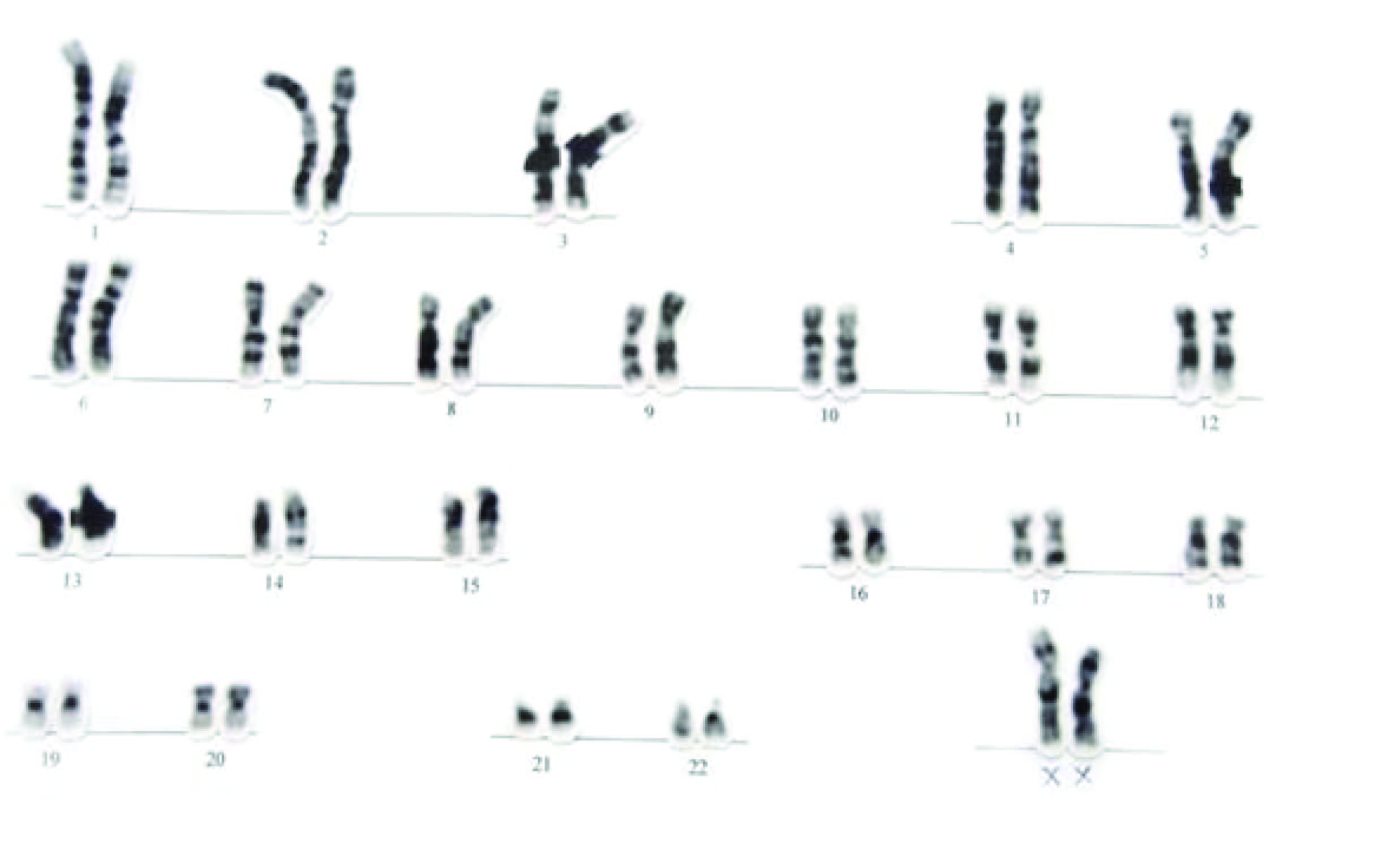
In the present study, out of 30 primary amenorrhoea subjects there were two subjects with abnormal karyotype- one subject with Turner syndrome, karyotype 45, XO [Table/Fig-11] and second of Mosaic Turner (Karyotype 45, XO/46, XX) [Table/Fig-12a&b]. When overall digital distribution of fingertip pattern (FTP) of these subjects was analysed on both hands, we observed that loops seemed to be of higher frequency in primary amenorrhoea females with abnormal karyotype (80%) as compared to primary amenorrhoea females with normal karyotype (62.14%). Arches seemed to be of higher frequency in primary amenorrhoea with abnormal karyotype (5%) as compared to primary amenorrhoea with normal karyotype (2.5%). But the frequency of whorls in primary amenorrhoea females with abnormal karyotype (15%) was decreased as compared to primary amenorrhoea with normal karyotype (35.35%) [Table/Fig-13].
G-Banded Karyotype of a Subject with Primary Amenorrhoea Karyotype: 45, XO (Turner Syndrome)
G-Banded Karyotype of a Subject with Primary Amenorrhoea-Mosaic Turner, Karyotype: 45, XO

G-Banded Karyotype of a Subject with Primary Amenorrhoea-Mosaic Turner, Karyotype: 46, XX
Finger tip pattern in primary amenorrhoea subjects along with Karyotype correlation
| Control F(n=30) | PAF(n=30) | PAF with normal karyotype (n=28) | PAF with abnormal karyotype (n=2) | Chi square | P value |
|---|
| Arch | 19(6.33%) | 8(2.67%) | 7(2.5%) | 1(5%) | 0.52 | 0.47, NS,p>0.05 |
| Loop | 202(67.33%) | 190(63.33%) | 174(62.14%) | 16(80%) | 7.86 | 0.005, S,p<0.05 |
| Whorl | 79(26.33%) | 102(33.99%) | 99(35.35%) | 3(15%) | 10.67 | 0.001, S,p<0.05 |
Discussion
Dermatoglyphics has been a useful tool in understanding basic biological questions in medicine, genetics and evolution since the past 150 y, apart from its wide application for personal identification. Dermatoglyphic analysis is now beginning to prove itself as an extremely useful tool for preliminary investigations into conditions with a suspected genetic basis [14].
In the present study we found reduction in total loops (TL) and total arches (TA) in ‘cases’ of primary amenorhoea group. Some authors found increased ulnar loops (6 of 10 cases) and increased whorls (3 of 10 cases with Turner’s syndrome) when dermatoglyphic study was carried out in ten female patients with sex chromatin abnormalities and genital tract anomalies complaining of primary amenorrhoea [15]. We also found increased total whorls (TW). Another author reported increased percentage of total loops and decreased percentage of arches in primary amenorrhoea subjects as compared to controls [16]. When dermatoglyphic analysis of 29 patients of classical gonadal dysgenesis was done it was observed that there was increased incidence of ulnar loops on the first digit of both hands [17]. Some authors found increased frequency of ulnar loops on first finger of right hand when study was carried out in 52 women with the Ullrich-Turner syndrome [18]. Dermatoglyphic study of the females having children with Trisomy 21 showed more arches and less whorls [19]. Increased ulnar loop was observed in schizophrenics with Down’s syndrome [20].
In our study frequency of loops and arches was highest in primary amenorrhoea subjects with abnormal karyotype (2 cases) when compared with primary amenorrhoea subjects with normal karyotype. Some workers observed an increase in ulnar loops and whorls but decrease in radial loops and arches in a study carried on Swedish cases of Turner’s syndrome showing the symptoms of ovarian dysgenesis [21]. Another author found higher frequency of loops in both controls and primary amenorrhoea cases frequency was especially higher in subjects with abnormal karyotype [9]. Some authors studied total finger ridge count (TFRC) in primary amenorrhoea cases. They found increased total finger ridge count in cases of primary amenorrhoea which coincides with our study [15,21].
Conclusion
Dermatoglyphics has been considered as a growing science with an immense practical value and it has been emphasized as one of the diagnostic tool which aids the cytogeneticist to look for specific abnormalities and identification of abnormal chromosomes.
In the present study, we found statistically significant increase in mean total finger ridge count in primary amenorrhoea cases. We also observed increased mean absolute finger ridge count, increased total radial loops and total whorls which were statistically insignificant. While total ulnar loops, total arches were decreased which were also statistically insignificant.
Thus the utility of dermatoglyphics is not to diagnosis, but to prognosis of disease and also the identification of people with the genetic predisposition to develop certain disease. Dermatoglyphics may be a useful screening method to identify the population at risk and referral of such individuals for karyotyping so that a watch may be kept for the early onset of symptoms.
[1]. Gibbs RC, Fundamentals of DermatoglyphicsArch Derm 1967 96:721-25. [Google Scholar]
[2]. Sadler TW, Integumentary systemIn: Langman’s Medical embryology 2010 11th edUSALippincott Williams and Wilkins:346 [Google Scholar]
[3]. Rajangam S, Janakiram S, Thomas IM, Dermatoglyphics in Down’s syndromeJ Indian Med Assoc 1995 93(1):10-13. [Google Scholar]
[4]. Sontakke BR, Ghosh SK, Pal AK, Dermatoglyphics of fingers and palm in Klinefelter’s syndromeNepal Med Coll J 2010 12(3):142-44. [Google Scholar]
[5]. Seltzer MH, Plato CC, Fox KM, Dermatoglyphics in the identification of women either with or at risk for breast cancerAm J Med Genet 1990 37(4):482-88. [Google Scholar]
[6]. Mathew I, Dermatoglyphic peculiarities in children with oral cleftsJ Indian Soc pedod prev dent 2005 :179-82. [Google Scholar]
[7]. Ravindranath R, Thomas IM, Finger ridge count and finger print pattern in maturity onset diabetes mellitusIndian J Med Sci 1995 49(7):153-56. [Google Scholar]
[8]. Metin Atasu, Dermatoglyphic findings in dental caries: a preliminary reportJ Clin Pediatr Dent 1998 22(2):147-49. [Google Scholar]
[9]. Meenakshi S, Balasubramanyam V, Rajangam S, Dermatoglyphics in amenorrhea- qualitative analysisJ Obstet Gynecol India 2006 56(3):250-54. [Google Scholar]
[10]. Padubidri VG, Daftary SN, Disorders of MenstruationIn: Hawkins & Bourne Shaw’s Textbook of Gynaecology 2011 15th edNew DelhiElsevier:284-85. [Google Scholar]
[11]. Datta DC, AmenorrhoeaIn: Textbook of Gynaecology 2008 5th edKolkataNew Central Book agency:437-38. [Google Scholar]
[12]. Ambulkar PS, Ghosh SK, Ingole IV, Pal AK, Genotoxic and cytotoxic effects of antibacterial drug, ciprofloxacin, on human lymphocytes in vitroNepal Med Coll J 2009 11(3):147-51. [Google Scholar]
[13]. Cummins Harold, Midlo Charles, HistoryIn: Finger Prints, Palms and Soles- An Introduction to Dermatoglyphics 1943 New YorkDovar:4-37. [Google Scholar]
[14]. Ramani P, Abhilash PR, Sherlin HJ, Anuja N, Premkumar P, Chandrasekar T, Conventional Dermatoglyphics- Revived Concept: A ReviewInt J Pharm Biol Sci 2011 2(3):B446-58. [Google Scholar]
[15]. Mutalik GS, Lokhandwala VA, Anjeneyulu R, Dermatoglyphical findings in primary amenorrhoeaJ Obstet Gynecol India 1968 18:738-43. [Google Scholar]
[16]. Kalpana VL, Satyanarayana M, Dermatoglyphical studies in Primary AmenorrheaJ Hum Ecol 1999 10(3):219-21. [Google Scholar]
[17]. Forbes A P, Fingerprints and Palm Prints and Palmar-Flexion creases in Gonadal Dysgenesis, Pseudohypoparathyroidism and Klinefelter’s syndromeNew Eng J Med 1964 270(24):1268-77. [Google Scholar]
[18]. Otto PA, Otto PG, The Importance of A’-d Ridge Count in Dermatoglyphic Diagnosis of the Ullrich-Turner SyndromeAm J Med Genet 1980 6:145-52. [Google Scholar]
[19]. Matsuyama N, Ito Y, The frequency of fingerprint type in parents of children with Trisomy 21 in JapanJ Physiol Anthropol 2006 25(1):15-21. [Google Scholar]
[20]. Singh Sardool, Dermatoglyphics of schizophrenics, patients with Down’s syndrome and mentally retared males as compared with Australian Europeans using multivariate statisticsAmerican Journal of Physical Anthropology 2005 42(2):237-40. [Google Scholar]
[21]. Holt SB, Lindsten J, Dermatoglyphic anomalies in Turner’s syndromeAnn Hum Genet. London 1964 28:87 [Google Scholar]