Treating a particular ailment with effective, safe and good quality drugs is the basic aim of drug therapy [1]. Irrational drug therapy use can lead to reduction in quality of drug therapy, increased risk of side effects, drug resistance [2]. Fixed dose combinations (FDCs) is a combination product of two or more active pharmacological ingredients (APIs) in a single dosage form. FDCs enhance the efficacy of individual drugs, decrease the chance of drug resistance, improve patient compliance and also decrease the pill burden on the patients [3].
The Seventeenth WHO Model List of essential medicines (March 2011) contains only 25 approved FDCs whereas the National list of essential drugs of India has 354 essential drugs including 14 FDCs [4,5]. Still there has been increase in the irrational FDCs in the recent past by leaps and bounds and many of them available as over the counter (OTC) drugs.
For any educational intervention to be successful and for the changes to be sustained, it should change the knowledge, attitudes and practices (KAP) of the target group. Tertiary care teaching hospitals have a dual role to play in terms of educating the students and simultaneously providing health care facility to the patients. Since dental clinicians and residents are primarily involved in patient management, so their awareness about prescribing medicines is of paramount importance. Thus, the present study was conducted to evaluate the knowledge, attitude and practices about the different fixed dose combinations among the clinicians from different department at a tertiary care teaching dental hospital in Jaipur city.
To evaluate knowledge, attitude and practice regarding FDCs among clinician at a tertiary care teaching dental hospital.
Materials and Methods
The present study was carried out with the dental clinicians working in conservative dentistry, orthodontics, prosthodontics, oral & maxillofacial surgery, periodontics, oral medicine & radiology, pedodontics. Prior to this survey, Institutional Ethics Committee (IEC) approval and written informed consent from clinicians of various departments of the tertiary care teaching dental hospital, Jaipur was taken. A prevalidated questionnaire, with details such as the resident's information about their respective department, year of study and questions regarding knowledge, attitude and prescribing practice of fixed dose combinations was used as a tool, administrated to all the resident doctors and the collected data was analysed.
Results
The present study was carried out in dental residents and clinicians of various departments of tertiary care teaching dental hospital, Jaipur. A total of 60 resident doctors and 77 dental clinicians were involved. Improved efficacy was the main advantage of FDCs mentioned by the residents (85%) and the dental clinicians (72%).
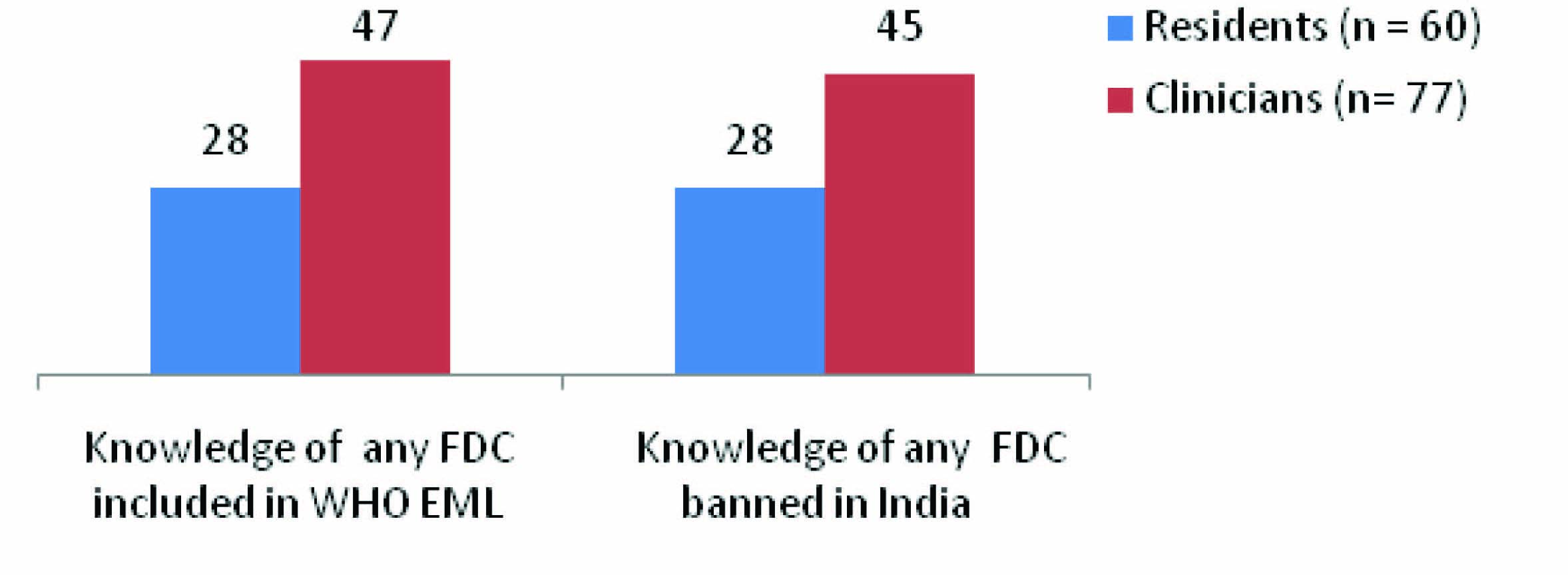
Difficulty in dose adjustments was the common disadvantage of prescribing FDCs mentioned by the study population [Table/Fig-1]. Knowledge about the rationality of commonly prescribed FDCs in dentistry was lacking in 80% of residents and 61.6% dental clinicians [Table/Fig-2]. On an average, only 47% of residents and 61% clinicians were aware of FDC included in WHO Essential Medicines List (EML).
Knowledge of advantages and disadvantages about FDCs*
| Advantages |
|---|
| Residents (n = 60) | Clinicians (n = 77) |
|---|
| Agree N (%) | Disagree N (%) | Uncertain N (%) | Agree N (%) | Disagree N (%) | Uncertain N (%) |
|---|
| Improvement in patient compliance | 39 (65%) | 15 (25%) | 6 (10%) | 70 (90.9%) | 7 (9.1%) | 0 |
| Enhancement of drug effect | 42 (70%) | 0 | 18 (30%) | 60 (77.9%) | 4 (5.2 %) | 13 (16.9%) |
| Lower manufacturing cost | 33 (55%) | 9 (15%) | 18 (30%) | 58 (75.3%) | 19 (24.7%) | 0 |
| Side effect of one can be reduced by combining it with another in FDC | 36 (60%) | 18 (30%) | 6 (10%) | 68 (88.3%) | 9 (11.7%) | 0 |
| Improvement in efficacy | 51 (85%) | 3 (5%) | 6 (10%) | 72 (93.5%) | 3 (3.9%) | 2( 2.6%) |
| Disadvantages |
| Titration of dose not possible | 60 (100%) | 0 | 0 | 74 (96.1%) | 0 | 3 (3.9%) |
| One of the drugs may be superfluous or wasteful | 20 (33.3%) | 30 (50%) | 10 (16.7%) | 15 (19.5%) | 60 (77.9%) | 2 (2.6%) |
| Financial burden on the patient | 45 (75%) | 10 (16.7%) | 5 (8.3%) | 30 (39%) | 47 (61.0%) | 0 |
| Increased incidence of adverse effects | 30 (50%) | 20 (33.3%) | 10 (16.7%) | 48 (62.3%) | 27 (35.1%) | 2 (2.6%) |
| Difficult to identify which medicine has caused adverse effects | 48 (80%) | 10 (16.7%) | 2 (3.3%) | 73 (94.8%) | 0 | 4 (5.2%) |
* FDC = Fixed dose combination
Analysis of knowledge of rationality of commonly prescribed FDCs in dentistry
| FDCs | Residents (n= 60) | Clinicians (n = 77) |
|---|
| Rational | Irrational | Rational | Irrational |
|---|
| Amoxicillin+Clavulanic Acid | 58 (96.7%) | 2 (3.3%) | 76 (98.7%) | 1 (1.3%) |
| Ampicillin+ Cloxacillin | 45 (75%) | 15 (25%) | 70 (90.9%) | 7 (9.1%) |
| Ofloxacin+Ornidazole | 55 (91.7%) | 5 (8.3%) | 60 (77.9%) | 17 (22.1%) |
| Mutivitamin+Antioxidants | 56 (93.3%) | 4 (6.7%) | 60 (77.9%) | 17 (22.1%) |
| Nimesulide+Diclofenac | 50 (83.3%) | 10 (16.7%) | 20 (26%) | 57 (74%) |
| Diclofenac+Paracetamol+Serratiopeptidase | 48 (80%) | 12 (20%) | 48 (62.3%) | 29 (37.7%) |
| Nimesulide+Paracetamol | 30 (50%) | 30 (50%) | 24 (31.2%) | 53 (68.8%) |
| Pantoprazole+Domperidone | 49 (81.7%) | 11 (18.3%) | 50 (64.9%) | 27 (35.1%) |
Only 47% residents and 58% dental clinicians could recall a single banned FDC in India [Table/Fig-3].
Analysis of knowledge about FDCs included in WHO Essential Medicines List (EML) and banned FDCs
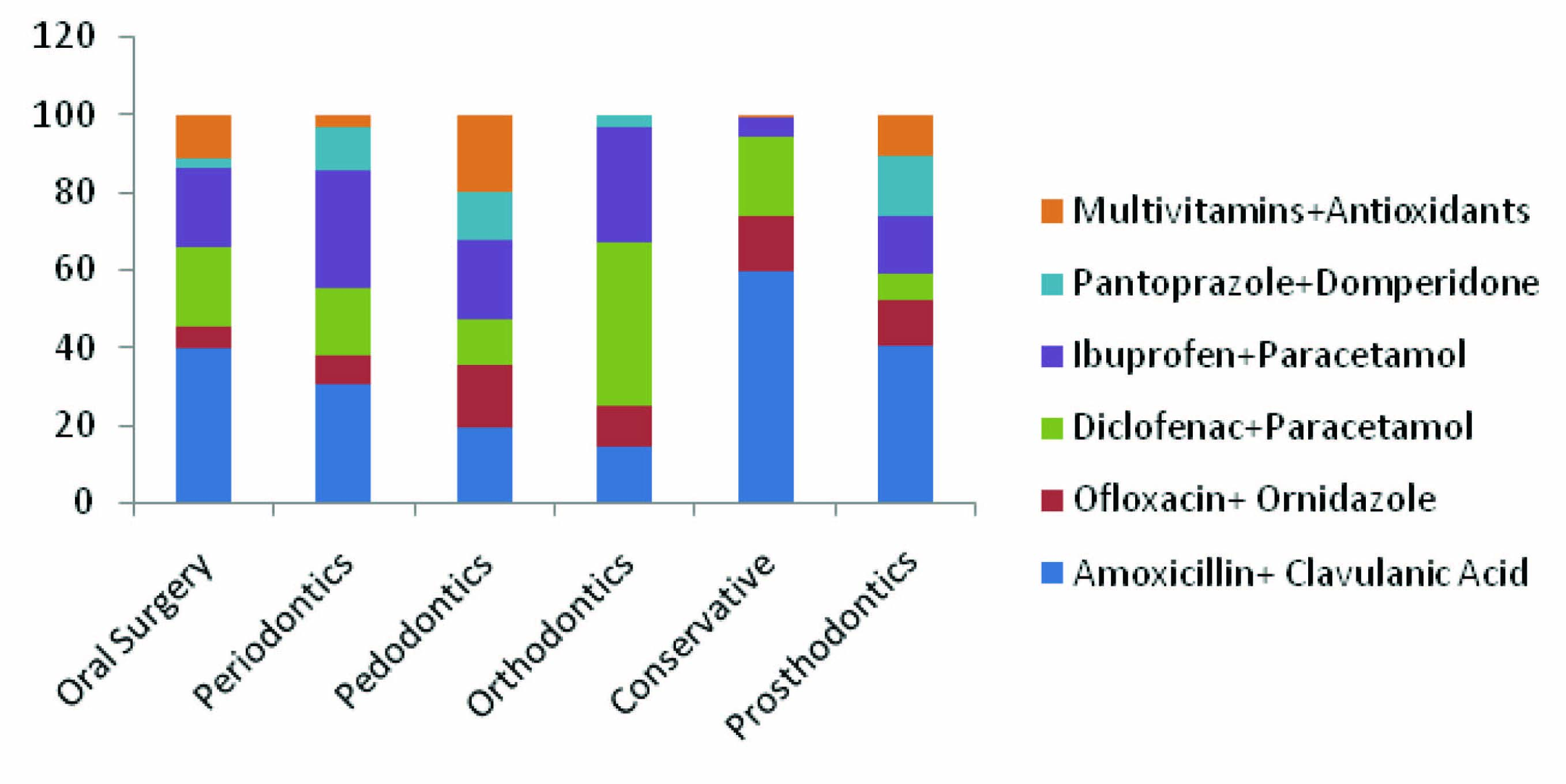
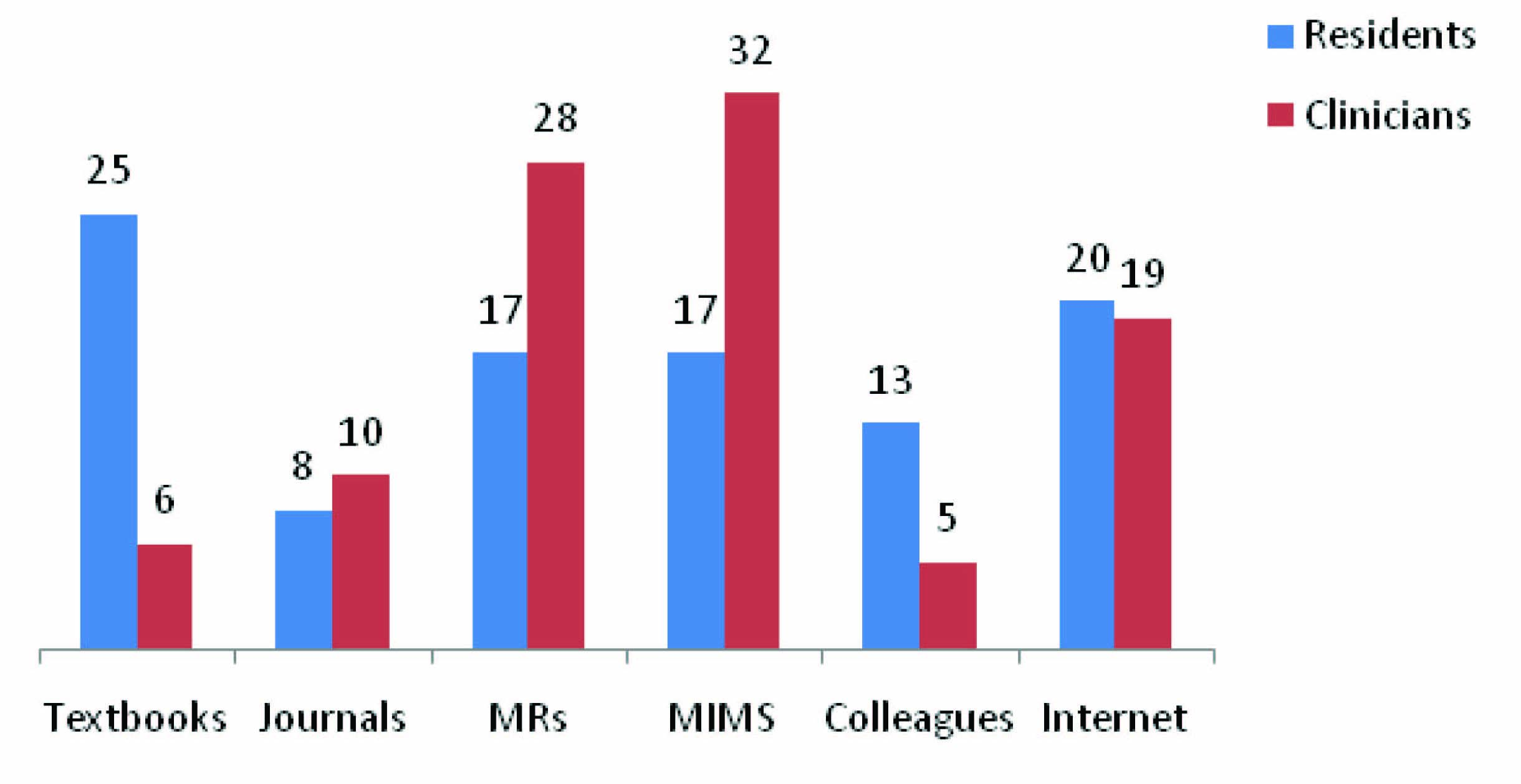
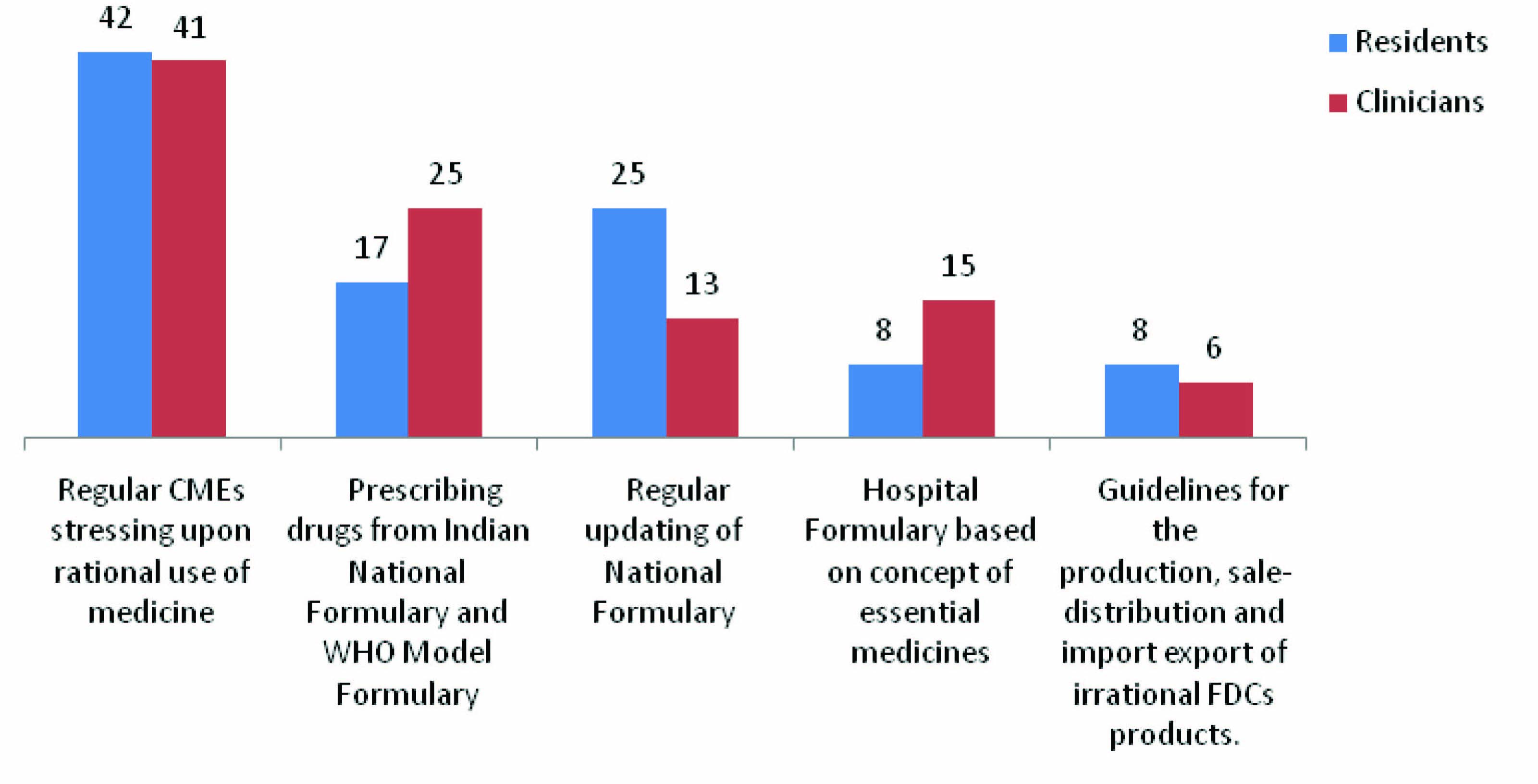
Antimicrobials (amoxicillin + clavulanic acid) were the most commonly prescribed FDCs (60%), followed by diclofenac and paracetamol combination (42%). The detailed results about most commonly prescribed FDCs in various dental departments are mentioned in [Table/Fig-4]. Textbooks (25%), internet(20%), Monthly Index of Medical specialities (MIMS) (17%) were the most common sources of information of FDCs for the residents whereas Monthly Index of Medical Specialities (MIMS) (32%), Medical representatives (MRs) (28%), internet (19%) were the most common sources of information of FDCs for the clinicians [Table/Fig-5]. Most of the dental clinicians (41%) and residents (42%) believed that regular Continuous Medical Education (CMEs) stressing upon rational use of medicine could sensitize them to the rational FDCs [Table/Fig-6].
Commonly prescribed FDCs in various dental departments
Sources of information about FDCs
Analysis of the perception of various interventions to reduce irrational FDCs *, * FDC = Fixed Dose Combination
Discussion
Earlier, studies have been conducted to assess the understanding levels of clinicians and pharmacists regarding irrational fixed dose combinations (FDCs) [6,7]. This study is unique and novel in the sense that no effort has been made earlier to assess the level of understanding among working dental clinicians and residents. The trend of prescribing FDCs is increasing in clinical practice [8,9]. The uncontrolled growth of the combinations with no therapeutic rationale has been the brainwave of many pharmaceutical companies in the recent years for their sustenance in the market place. The most imperative concern with irrational FDCs is that they expose patients to unnecessary risk of adverse drug reactions, antibiotic FDCs are responsible for increasing the chances of resistance [10].
It was observed from the study that improved efficacy and enhancement of the drug effect were the most common advantages mentioned by the residents and clinicians respectively. But, according to World Health Organization (WHO) guidelines there are a number of other advantages like decreased chances of adverse drug reactions, improvement in patient compliance, convenience of prescribing.
Titration of doses to suit the needs of individual patient, incompatible pharmacokinetics, drug interactions, potential quality problems are the other disadvantages of using FDCs [6,10]. Knowledge about the availability of WHO Essential Medicines List (EML) was lacking in residents and dental clinicians. 53% of the residents were not aware of any FDCs in WHO EML and unfortunately 25% among these residents were unaware about the mere existence of Essential Medicines List (EML). 39% of the dental clinicians also were unaware of any FDCs in WHO EML. WHO introduced the concept essential drug list in 1977 and updates the model list every year. The government of India, under the Ministry of Health and Family Welfare has also recommended the list of essential medicines in India. Knowledge about Essential Medicines List and its updates helps the prescribers to select the drugs and use them rationally for better treatment outcome. The lack of knowledge about EML may be due to lack of sensitization of the residents and may be one of the important causal factors for prescribing errors.
India has banned a total of 69 drugs and their combinations with other drugs for manufacturing and marketing in India [11]. Knowledge about the banned drugs/FDCs is very important as lack of this knowledge and prescribing of these agents may lead to serious, adverse drug reactions. In our study only 47% residents and 58% dental clinicians could recall a single banned FDC in India.
The knowledge about rationality of commonly prescribed FDCs in dentistry was lacking in 80% of residents and 61.6% dental clinicians. On asking the respondents to mention about the rationality of most commonly used FDCs (ampicillin + cloxacillin, ofloxacin + ornidazole, amoxicillin + clavulanic acid, multivitamins + antioxidants, nimesulide + diclofenac, diclofenac + paracetamol +serratiopeptidase, nimesulide+paracetamol, pantoprazole+ domperidone) most of the respondents could not do so. There are number of FDCs which are not rational and still available in the market. Hence, there is need to educate resident doctors about the basis of rationality of each component of the FDCs [8,12,13].
Ampicillin/Amoxicillin are effective only against gram negative bacilli but not against beta lactamase producing staphylococci. while cloxacillin is antistreptococcal penicillin with no effect on gram negative bacilli, since both these infections rarely co-exist, so combining them is irrational [14,15]. Adding paracetamol to another nonsteroidal antiinflamatory drug (NSAID) like diclofenac, aceclofenac, and ibuprofen does not offer additional benefit, but increases the chances of nephrotoxicity [16]. Serratiopeptidase is a proteolytic enzyme supposed to relieve inflammation. This claim is not based on controlled clinical trials and FDCs containing this compound with NSAIDs offer no additional anti-inflammatory advantage except higher cost to the patient [17].
Combinations of NSAIDS/analgesics with antispasmodic agents are irrational and they can result in dangerous elevation of the body temperature. As per WHO guidelines, the combination of vitamins are part of nutrition, and vitamin combinations should not be used indiscriminately [14]. H2 blockers and proton pump inhibitors are effective in peptic ulcer and it is irrational to combine these drugs with an antiemetic as peptic ulcer is not always associated with vomiting.
It is staggering to state that over 70 dangerous FDCs are being sold in India under more than 1000 brand names [18]. In our country the pipeline of development of a new drug molecule is nearly dry. In addition lack of profitability and arduous, meticulous drug development factors have forced the pharmaceutical industry to create and manufacture so called novel products by just mixing two or more drugs.
FDCs of cardiovascular drugs like Ramipril + Telmisartan are associated with more adverse events without any additional benefit [19]. Likewise combining two antihypertensives affecting the same pathway (Enalapril + Losartan) is irrational as it does not add to efficacy. In FDCs of cough and cold remedies such as cetirizine + phenylpropanolamine + dextromethorphan; phenylpropanolamine is a banned drug due to its potential to cause stroke. Phenylpropanolamine can also aggravate diabetes, glaucoma and prostate enlargement.
There is no justification in combining mucolytic agent (Ambroxol) with antibacterial (Ciprofloxacin or Cefadroxil or Roxithromycin), as thick secretions in respiratory tract are not always because of respiratory infections. Also, the antibacterial therapy always does not require an associated dose of mucolytic agent. Hypolipidemic drugs such as atorvastatin and nicotinic acid in fixed dose combinations have increased probability of myopathy [20].
On the other hand injudicious use of antibiotic FDCs is rapidly giving rise to resistant strains of organisms which is becoming a lethal problem and the pipeline for new antimicrobials remains meagre. A glaring example is the emergence of ciprofloxacin resistant strains of Salmonella typhi which has made the treatment of typhoid fever not only difficult but also expensive [14,17]. Metamizole should not be used as fixed-dose combination with antibiotics, though this drug might have a place in therapy as a single substance but its benefits need to be carefully weighed against its severe haematological adverse effects: agranulocytosis [21].
In the present study, we observed that Monthly Index of Medical specialities (MIMS), medical representatives were the most common sources for information about FDCs while use of Essential Medicines Lists, journals and CMEs was very less, which shows that the use of authentic sources of drug information was less and could also be a factor for lack of knowledge and irrational/unjustifiable FDC prescription by both the residents and the dental clinicians. Both the residents and clinicians in our study favoured regular CMEs stressing upon the rational drug use to deal with the current problem.
Conclusion
We observed that both the residents and dental clinicians had poor knowledge about FDCs. Moreover, dependence on medical representatives for medical information by the prescribers, ultimately leads to an irrational use of medicines. It is urgently required that concepts of rational drug use should be implemented in pragmatic and field situations. It is the need of the hour to raise our voice against the growing list of irrational FDCs and to reduce the magnitude of this problem by sensitizing the residents as well as the dental clinicians regarding the efficacy, safety, suitability, rationality and cost benefits of commonly prescribed FDCs.
* FDC = Fixed dose combination