Materials and Methods
A prospective study of 11 cases of FNAC (fine needle aspiration cytology) of breast lumps was done in ESIC Medical College & Post Graduate Institute of Medical Sciences and Research, Bangalore, from July 2013 to December 2013. Clinical details regarding age, symptoms, size of the lesion and lymph node involvement was noted in all cases [Table/Fig-1]. FNAC was performed by pathologists using 22 gauge needles and 10 ml syringes. FNAC was done by conventional procedure. Direct smears were made from the material aspirated. In some cases where fluid was aspirated, the fluid was subjected to cytospin (thermoscientific) at a speed of 600 rpm (revolution per minute) for 5 min and smears were prepared. Two smears from each case were fixed in 95% isopropyl alcohol and were stained with PAP (Papanicolonue stain) and H & E (Hematoxylin & Eosin). One smear from each case was air dried and stained with Leishman stain. AFB (acid fast bacilli) stain was done in all cases of cytologically diagnosed as granulomatous mastitis and acute suppurative granulomatous mastitis. Two smears in each case were screened with Toludine blue stain for presence of multinucleated giant cells, fixed with 95% isopropyl alchohol and subjected to immunocytochemistry for vimentin(vimentin 6 ml, Rabbit, clone SP20 Ref:A00105, Lot-23526 SCYTEK Laboratories, Logan Utah USA) and CD34 (Endothelial cell, 6 ml, Mouse, Clone QBEnd/10 Ref-A00070, Lot-23384 SCYTEK Laboratories, Logan Utah USA). Standard Protocol for immunocytochemistry is explained in brief. Firstly the slide was washed in TRIS buffered saline, 10 min each for three changes. Then the slide was treated with 3% hydrogen peroxide methanol for 10 min, then again washed in TBS, followed by protein blocking for 10 min. Then it was incubated with primary antibody at room temperature for one hour. It was then washed in TBS. Then post primary blocking was done for 30 min. The slides were washed in TBS. Then it was treated with Polymer for 30 min, which was followed by washing in TBS. Then it was treated in with DAB-chromogen for 5-10 min (till appearance of brown colour). The after washing in distilled water, counter staining was done with haematoxylin for 1 min. Finally, it was washed under running tap water followed by graded dehydration in alcohol, cleared in xylene and mounted with DPX. Only the breast aspirates having multinucleate giant cells were considered for the study which included infections/inflammatory and benign lesions. Malignant lesions were excluded. Stromal type multinucleate giant cells were differentiated from histiocytic type multinucleate giant cells cytomorphologically. Multinucleated giant cells with ill-defined cell border, vacuolated/foamy cytoplasm and vesicular nucleus with prominent nucleoli were considered as histiocytic type multinucleate giant cells. Multinucleated giant cells with definite cell border, homogenous cytoplasm with bland nucleus were considered as stromal type multinucleated giant cells. Langhan’s type of giant cells was also considered. Vimentin was used as marker for stromal type multinucleated giant cells and CD34 for histiocytic type multinucleated giant cells. In all cases various cytological parameters like the presence of stromal type multinucleate giant cells, histiocytic type multinucleate giant cells, epithelioid cells, necrosis, inflammatory cells and duct epithelial cells were evaluated [Table/Fig-2]. Cases with granulomatous component along with dense neutrophils were classified as acute suppurative granulomatous mastitis. AFB stain was done in all cases of granulomatous mastitis and acute suppurative granulomatous mastitis. Radiological findings, culture of the aspirate and histopathology of the lesion was considered in the available cases.
Clinicopathologic spectrum of cases with breast lesions
| Case No. | Age yrs | Sex M/F | O/E | C P D | FNAC D | HPE | ICC |
|---|
| R/L | S | N |
| 1 | 20 | F | B/L | 2x2 | WD | FA | GM | FCD with TA | Vimentin +ve CD34 focal +ve |
| 2 | 50 | F | R | 2x2 | ID | Carcinoma | GM | – | Vimentin +ve CD34 focal +ve |
| 3 | 35 | F | L | 3X2 | WD | Fibroadenosis | GM | – | Vimentin +ve CD34 focal +ve |
| 4 | 23 | F | B/L | 3X2 | ID | Fibroadenosis | GM | | Vimentin +ve CD34 focal +ve |
| 5 | 29 | F | B/L | 2X1 | WD | Benign breast lesion | RT-GM LT-BBL | B/L FA | Vimentin +ve CD34 focal +ve |
| 6 | 40 | F | L | 5X3 | ID | Benign breast lesion | GM | | Vimentin +ve CD34 focal +ve |
| 7 | 49 | F | L | 3x2 | ID | Benign breast lesion | ASGM | | Vimentin +ve CD34 focal +ve |
| 8 | 42 | M | L | 3x2 | ID | Mastitis | ASGM | | Vimentin +ve CD34 focal +ve |
| 9 | 28 | F | L | 2x2 | WD | FA | FA | | Vimentin +ve CD34-ve |
| 10 | 32 | F | R | 3x2 | WD | FA | FA | | Vimentin +ve CD34-ve |
| 11 | 43 | F | L | 3x1 | ID | Benign breast lesion | FN | | Vimentin +ve CD34-ve |
M: male, F: female, O/E: on examination, WD: well defined, ID: ill defined, FA: fibroadenoma, ASGM: acute suppurative granulomatous mastitis, FN: fat necrosis, R: right, L: left, FN: fat necrosis
Cytology findings in breast lesions with multinucleate giant cells on FNAC
| CN | MNGC | EH | N,L, P | Necrosis | Duct epithelial | AFB | Diagnosis |
|---|
| 1 | Histiocytic type | A | L | A | P | A | GM |
| 2 | Histiocytic type | P | L | A | A | A | GM |
| 3 | Histiocytic type | P,TB | L,P | A | P | A | ASGM |
| 4 | Stromal type | N | – | A | P | A | FA |
| 5 | Histiocytic type ,FB Type | P | L,P | Focal P | P | A | ASGM |
| 6 | Histiocytic type | P | N | P | A | A | FN |
| 7 | FB,Langerhans | P | N | P | A | A | ASGM |
| 8 | Histiocytic type | P | N | P | P | A | GM |
| 9 | Histiocytic type | P | N | A | P | A | ASGM |
| 10 | Histiocytic type/stromal type | P | NIL | A | P | A | FA |
| 11 | Histiocytic type | P | NIL | A | P | A | FA |
MNGC: multinucleate giant cells, EH: Epithelioidhistiocytes, N: neutrophils, L: lymphocytes, P: plasma cells, AFB: Acid fast bacilli, GM: granulomatous mastitis, A: absent, P: present, ASGM: acute suppurative granulomatous mastitis, FN: Fat necrosis
Results
Here, we report 11 cases of breast lesions which showed multi-nucleate giant cells on FNAC. Ten of these cases were females and one was a male patient. Age of the patients ranged from 20-50 y. Nine cases presented with unilateral lesion and three cases have bilateral breast lesion. The size of the lesion in most of the cases varied from 3-6 cm [Table/Fig-1]. One case was clinically diagnosed as carcinoma. Later, it was diagnosed as granulomatous mastitis. Radiology findings and culture reports were available in only two cases. Culture sent for mycobacterium bacilli was negative in both the cases. Ultrasonography of one case was reported as suggestive of suspicious lesion, ACR BIRADS category 4- low grade suspicious lesion. Another case showed sonological features suggestive of breast abscess with possibility of infective aetiology. Regional lymphadenopathy was not present in any of these cases. Cytologically six cases showed granuloma debris with relative proportion of component cells including epithelioid histiocytes, lymphocytes, neutrophils and multinucleate giant cells. The number of nucleus in these multinucleate giant cells ranged from 5-15. They were arranged irregularly or occasionally in a horse shoe manner [Table/Fig-3,4,56]. In our series well-formed granuloma’s were not present in any of the cases but most cases showed epithelioid histiocytes and multinucleate giant cells. So, a diagnosis of granulomatous mastitis was given. Two cases with granulomatous component also showed acute suppurative inflammation composed of dense polymorphs, these cases were diagnosed as acute suppurative granulomatous mastitis. AFB was negative in all the cases. Stromal type giant cells were present in two cases of fibroadenoma [Table/Fig-7]. One case of fat necrosis showed histiocyte type multinucleate giant cells [Table/Fig-2]. Immunocytochemistry showed vimentin positivity in both stromal and histiocytic type of multinucleate giant cells and in isolated histiocytes. CD34 was focally positive in histiocytic type of giant cells [Table/Fig-8&9]. Histopathology of two cases turned out to be fibrocystic disease with tubular adenosis and fibroadenoma. Remaining cases were lost for followup.
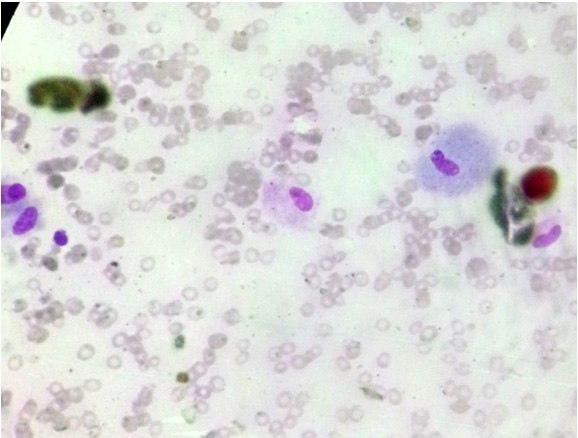
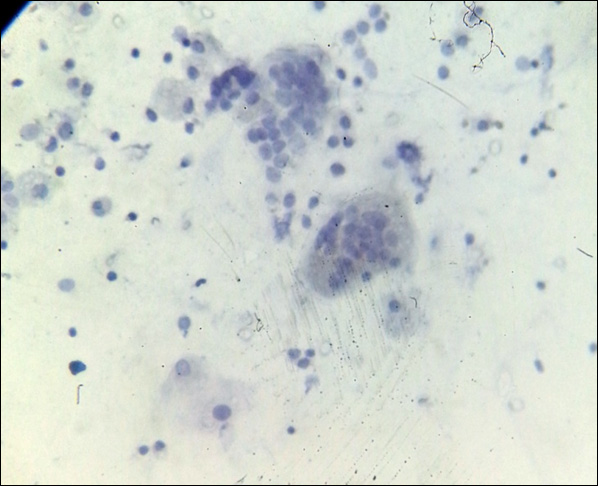
Microphotograph of leishman stained smear showing scattered epithelioidhistiocytes in a background of erythrocytes and lipid
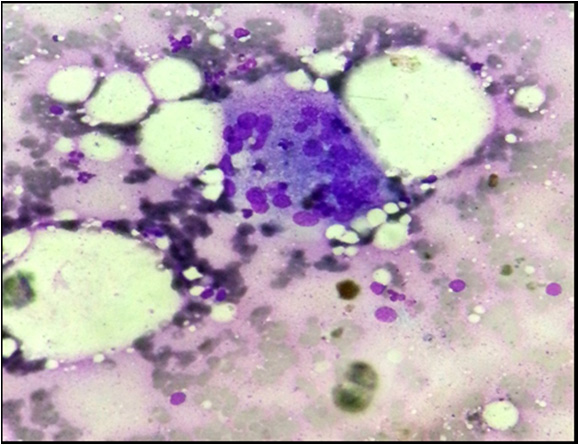
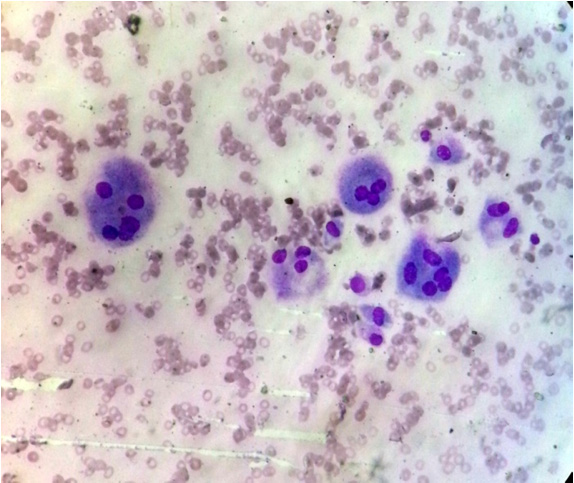
Microphotograph of leishman stained smear showing histiocytic type of multinucleate giant cells surrounded by few lymphocytes
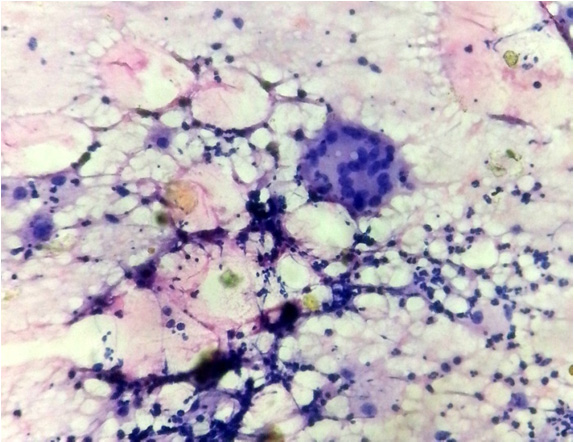
Microphotograph of leishman stained smear show histiocytic type of multinucleate giant cell surrounded by polymorps and lyphocytes
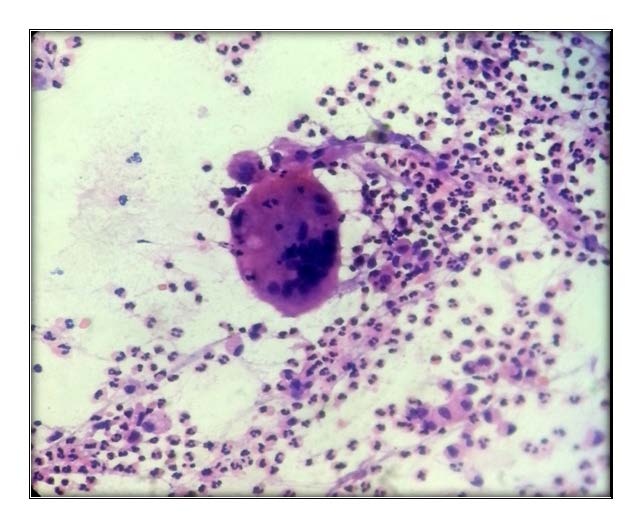
Microphotograph of leishman stained smear shows langhans type of multinucleate giant cells background of dense polymorphs
Microphotograph of leishman stained smear shows scattered stromal type of multinucleate giant cells
Microphotograph of Vimentin stained smear shows positivity in stromal type of multinucleate giant cells
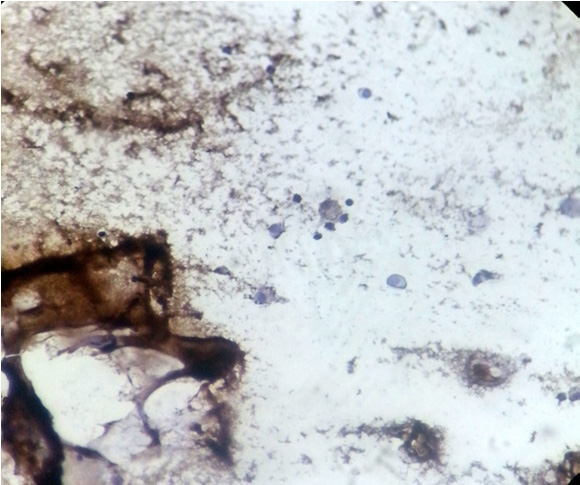
Microphotograph of CD34 stained smear show focal positivity in histiocytic type of multinucleate giant cell
Discussion
FNAC breast is a safe OPD procedure with a sensitivity of 96% and specificity of 100% in identifying benign and malignant lesions. FNAC diagnosis of inflammatory breast lesion is a useful tool in directing management and treatment of the patient and avoiding unnecessary surgeries. Cytological findings correlated with microbiological cultures gives better results. Multinucleate stromal giant cells have been infrequently described in a number of benign and malignant breast lesions, including fibroepithelial lesions [1].
Due to its rarity only a few cases of multinucleate giant cells have been reported cytologically. The histogenesis of multinucleate giant cells remains obscure and controversial, with several conflicting reports in literature the most consistent finding with IHC studies is multinucleate giant cell stain strongly positive for vimentin which is one of the type 2 IF protein in the cytokeratin and is known to play a significant role in maintaining cell shape integrity of the cytoplasm and stabilizing cytoskeletal interaction. Lei and Gilcrease [4] who reported on the histopathological and IHC features of breast spindle cell tumours suggested that vimentin, and CD34, was positive in fibroblast of mammary stroma which could be the result of differentiation from pluripotent mesenchymal precursor cell with a potential to differentiate towards several mesenchymal cell lines. Multinucleate stromal giant cells show inconsistent focal positive staining with histiocytic markers such as alpha 1 anti-trypsin, HAM 56, CD 34, and CD 68. These markers of histiocyte differentiation more consistently found positive in osteoclast like giant cells [5]. In our study vimentin was positive in all stromal and histiocytic multinucleate giant cells and CD34 showed focal positivity for histiocytic multinucleate giant cells.
The causes of granulomatous mastitis includes TB, fungus, aspergillus, blastomycosis, coccidiodomycosis, histoplasmosis, actinomyces, Cat scratch disease, foreign bodies (including suture and silicone injection or leaking breast implants), subareolar abscess, duct ectasia, and idiopathic causes. The cytological diagnosis of granulomatous mastitis is difficult because the features overlap with other aetiologies including tuberculosis. Tse et al., [6] have described granulomatous mastitis cytologically in cases having predominantly neutrophils and epithelioid histiocytes even in the absence of characteristic features of granulomas and necrosis.
Multinucleate giant cells engulfing lipid has been described in fat necrosis of breast. Cytomorphology showed histiocytes and multinucleate giant cells. The degenerated RBCs conglomerate in the setting of high levels of free fat released by the necrotic adipocytes. These conglomerations are referred to as “myospherulosis”, which is characteristic of fat necrosis on cytology. In the late stage of fat necrosis, usually hemosiderin deposition and the development of fibrosis is seen. We present one case of fat necrosis with numerous multinucleate giant cells [7].
Breast tuberculosis should be considered in the differential diagnosis of granulomatous mastitis in Indian scenario. Breast is considered to be a rare sight of extra-pulmonary mycobacterial infection, comprising 0.1 % of all tuberculosis cases. FNAC establishes the diagnosis in most cases. Khanna et al., reported a success rate of 100% in his series while Khakker et al., reported a success rate of 73% and stated that FNAC diagnosis rest on cytological findings of granuloma having multinucleate giant cells with or without demonstrable AFB organisms. TB mastitis can be associated with acute inflammation, particularly early in the course of disease; therefore part of the aspirate should be cultured for TB [8]. However, in our series the sample was sent for culture in two cases and they were negative.
Multinucleate stromal giant cells are rarely identified in fine needle aspiration of fibroadenoma. Recognition of this peculiar finding may help to avoid misdiagnosis of other sinister conditions, such as phyllodes tumour and metaplastic carcinoma [9]. The typical benign cytoarchitecture of a fibroadenoma in a back ground of naked multinucleate cells indicate the benign nature of the lesion. We present two cases of fibroadenoma with stromal multinucleate giant cells.
FNAC is a well established method for the diagnosis of breast lesions in males also. However, little attention has been focused on inflammatory lesion in male’s. Silverman et al., [10] and Lopez et al., [11] have reported one and two cases of subaeriolar abscess respectively. In our series only one case presented with features of acute suppurative granulomatous mastitis in male.
Conclusion
Multinucleate giant cells are found in inflammatory, benign and malignant breast lesions. An attempt is made to study various types of multinucleate giant cells on cytology which facilitate accurate diagnosis and appropriate management of the patient. A distinction should be made between the stromal giant cells and those of histiocytic origin to know and think about their histogenesis and role in these lesions. Further molecular studies have to confirm these findings.
M: male, F: female, O/E: on examination, WD: well defined, ID: ill defined, FA: fibroadenoma, ASGM: acute suppurative granulomatous mastitis, FN: fat necrosis, R: right, L: left, FN: fat necrosis
MNGC: multinucleate giant cells, EH: Epithelioidhistiocytes, N: neutrophils, L: lymphocytes, P: plasma cells, AFB: Acid fast bacilli, GM: granulomatous mastitis, A: absent, P: present, ASGM: acute suppurative granulomatous mastitis, FN: Fat necrosis