Acute generalized peritonitis from gastrointestinal hollow viscus perforation is a potentially life threatening condition. The prognosis of peritonitis remains poor despite development in diagnosis and management. Early identification of patients with severe peritonitis may help in selecting patients for aggressive surgical approach [1–3]. Grading the severity of acute peritonitis has assisted in no small way in decision making and has improved therapy in the management of severely ill patients [4]. Empirically based risk assessment for important clinical events has been extremely useful in evaluating new therapies, in monitoring resources for effective use and improving quality of care [5,6].
Many scoring systems have been designed and used successfully to grade the severity of acute peritonitis like, Acute physiology and chronic health evaluation (APACHE) II score, Simplified acute physiology score (SAPS), Sepsis severity score (SSS), Ranson score, Imrite score, Mannheim peritonitis index (MPI) [7,8]. MPI was developed by Wacha and Linder in 1983 [9]. It was developed based on the retrospective analysis of data from 1253 patients with peritonitis, in which 20 possible risk factors were considered. Of these only 8 proved to be of prognostic relevance and were entered into the Mannheim Peritonitis Index, classified according to their predictive power. Patients with a score exceeding 26 were defined as having a high mortality rate [9] The Mannheim Peritonitis Index (MPI) is a specific score, which has a good accuracy and provides an easy way to handle with clinical parameters, allowing the prediction of the individual prognosis of patients with peritonitis [10]. There are no published Indian studies to assess the validity of this scoring system.
Materials and Methods
Prospective study of 50 patients conducted in JSS Medical college Hospital, Mysore, Karnataka, India, from November 2011 – May 2013. Patients presenting with peritonitis secondary to hollow viscus perforation were included in the study. Patients with primary peritonitis, peritonitis due to trauma, age less than 15 years and patients who were managed conservatively were excluded from the study. Initial preoperative work up and resuscitation with intravenous fluids, antibiotics, analgesics, nasogastric decompression was done in all the cases. Site of peritonitis secondary to hollow viscus perforation was diagnosed during surgery and was dealt with appropriate surgical procedure. Peritoneal lavage was given in all cases. The MPI [Table/Fig-1] was applied along with other clinical and biochemical parameters recorded in pre-structured proforma. Prediction was categorized into 3 groups: i) score ≤ 20 ii) Score 21-29 iii) score ≥ 30. Further resuscitation and ICU care was given as and when was necessary. Patients were followed up postoperatively till the outcome i.e. mortality, morbidity or discharge. Data obtained was analysed for predicting mortality and morbidity.
Mannheim Peritonitis Index [9,11]
| Risk Factor | Weightage, if any |
|---|
| Age >50 years | 5 |
| Female Gender | 5 |
| Organ Failure* | 7 |
| Malignancy | 4 |
| Preoperative duration of peritonitis >24 hours | 4 |
| Origin of sepsis not colonic | 4 |
| Diffuse generalised peritonitis | 6 |
| Exudates | |
| Clear | 0 |
| Cloudy, Purulent | 6 |
| Faecal | 12 |
*Definitions of organ failure: Kidney: creatinine >177 μmol/L, urea >167 μmol/L, oliguria <20 ml/h; Lung: pO2 <50 mmHg, pCO2 >50 mmHg; Shock: hypodynamic or hyperdynamic; Intestinal obstruction (only if profound): Paralysis >24 h or complete mechanical ileus
Statistical Analysis
Statistical analysis was done using EPIINFO and SPSS (Version 16). Chi-squared test was used for intergroup comparisons. Risk ratio and 95% confidence interval (CI) were calculated for each group. ROC analysis was performed to identify the threshold with highest sensitivity and specificity and that threshold was used for classification in univariate and binary logistic regression analysis. The level of significance was fixed at p-value of < 0.05.
This study was conducted after obtaining the clearance from the ethical committee of the institute and informed written consent from the patients included in the study.
Results
Mean age in our study was 43.8 (± 15.8) years (range 18–85). For those who survived, Mean days of hospitalization was 15.5 days.
Simple closure of perforation was done in 24% cases, closure with omental graft was done in 46% cases, laparoscopic perforation closure was done in 8% cases, resection anastomosis in 2%, resection with ileostomy in 4% appendicectomy in 12%, ileo-transverse anastomosis in 2% and colostomy was done 2% case. Outcome has been summerized in [Table/Fig-2].
Site of perforation and outcome
| Site | Survived (%) | Death (%) | Total |
|---|
| Stomach | 2(100) | 0 | 2 |
| Duodenum | 26(96) | 1(4) | 27 |
| Jejunum | 0 | 1(100) | 1 |
| Ileum | 8(73) | 3(27) | 11 |
| Jejunum & ileum | 1(100) | 0 | 1 |
| Appendix | 5(83) | 1(17) | 6 |
| Colorectal | 1(50) | 1(50) | 2 |
There were seven deaths (14%) in our study, five patients died of multiple organ dysfunction and two patients died of cardiogenic shock. Only one patient in the study had perforation in the rectum due to malignancy but expired on POD 6th due to septicaemia and ARF. Mortality was 5% in patients who presented within 24 h, 13% in patients who presented between 2 to 5 d and 50% in patients who presented after 5 d.
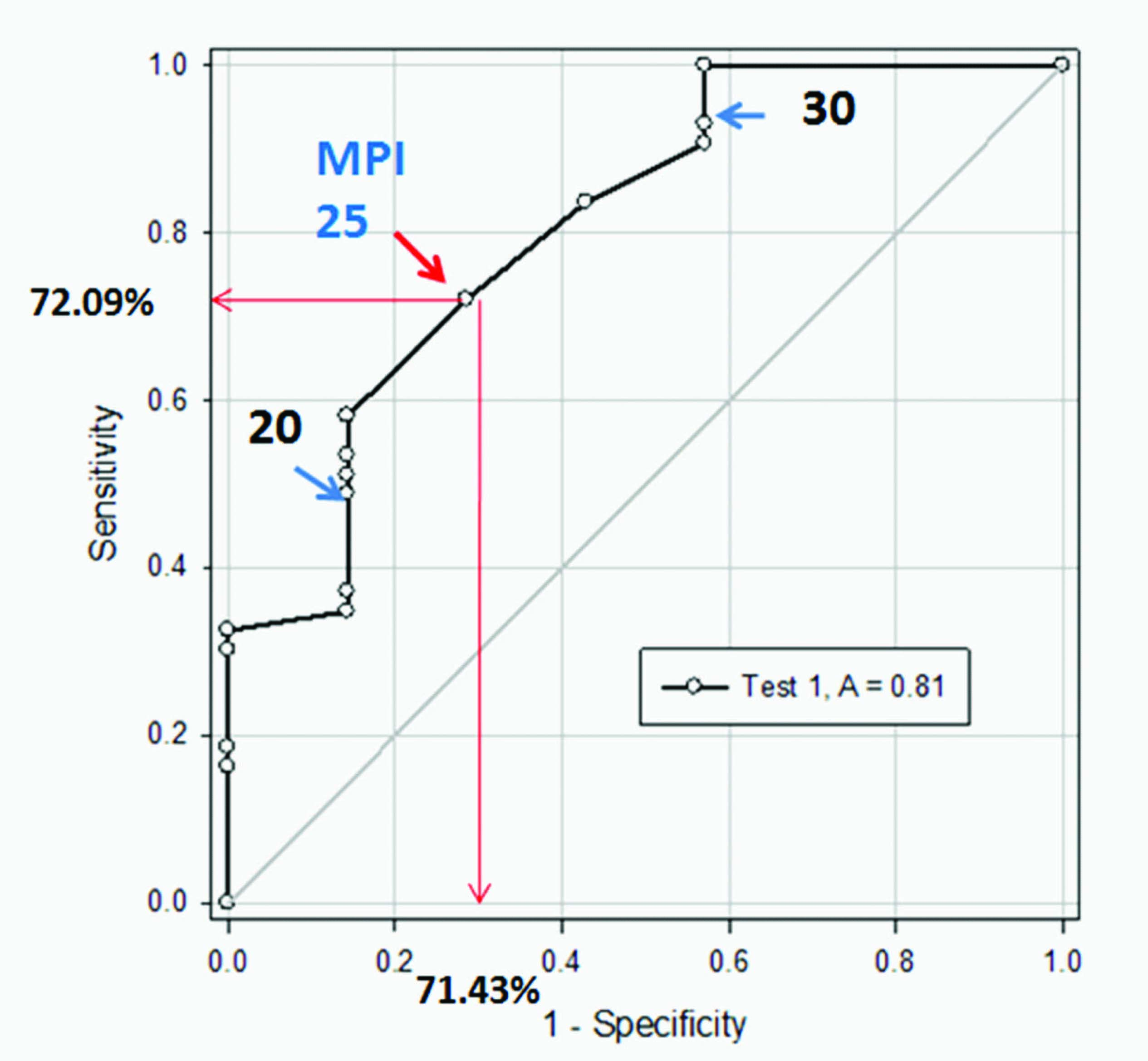
MPI score was analysed with the mortality [Table/Fig-3]. With highest sensitivity of 72.09% and specificity of 71.43% MPI score of 25 was taken as a threshold value for dichotomous analysis using ROC curve [Table/Fig-4]. MPI score of 26 and more were associated with 29.4% mortality compared to patients with MPI score of 25 and less which was 6.1% mortality and was statistically significant (p=0.03). Summary of the MPI in our study has been depicted in [Table/Fig-5].
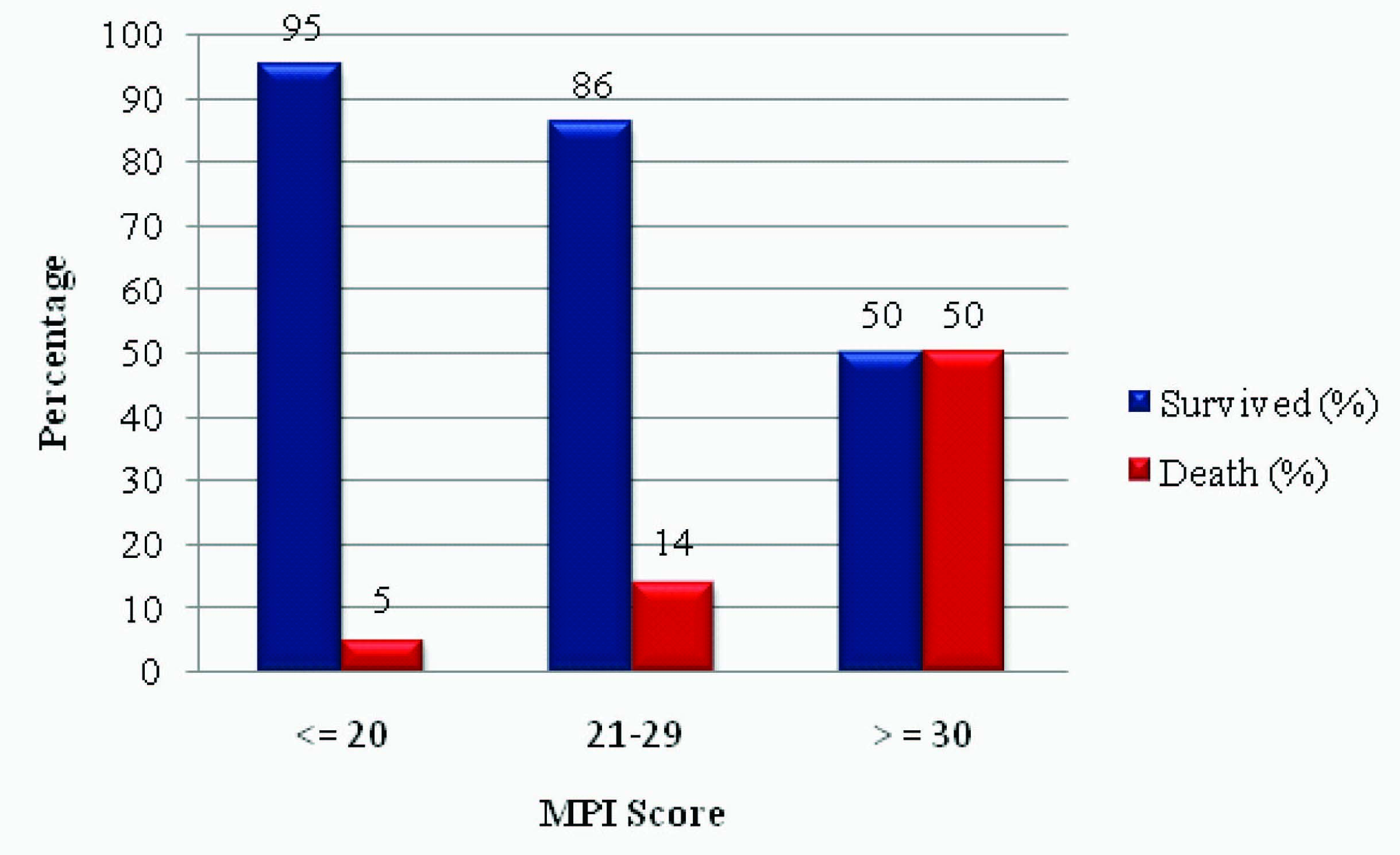
Outcome distribution according to MPI score
ROC curve of sensitivity and specificity of MPI score for mortality
Summary of MPI in our study (50 cases)
| Summary of MPI | Survived (%) | Death (%) | Total | p-value |
|---|
| Age >50 y | 15 (83) | 3 (17) | 18 | p=0.69 |
| Female sex | 3 (75) | 1 (25) | 4 | p=0.46 |
| Organ Failure | 25 (78) | 7 (22) | 32 | p=0.04 |
| Malignancy | 0 | 1 (100) | 1 | p=0.14 |
| Preoperative duration >24 h | 30 (81) | 7 (19) | 37 | p=0.17 |
| Origin of sepsis not colonic | 37 (88) | 5 (12) | 42 | p=0.31 |
| Diffuse generalised peritonitis | 40 (87) | 6 (13) | 46 | p=0.46 |
| Exudates |
| Clear | 12 (100) | 0 | 12 | p=0.17 |
| Cloudy/Purulent | 24 (89) | 3 (11) | 27 | p=0.68 |
| Faecal | 7 (64) | 4 (36) | 11 | p=0.03 |
MPI score was also evaluated with morbidity. Overall morbidity in our study was 38%. Pulmonary complications were seen in 18% cases, surgical site infection (SSI) was seen in 16% cases, Hypotension in 6% cases, wound dehiscence was in 4% cases, Intra-abdominal abscess and ARF was observed in 2% cases respectively. According to the analysis MPI score of ≥ 26 had 5.72 times higher risk of morbidity than MPI score of ≤ 25 (CI 1.60 – 20.48, p=0.005).
Discussion
Peritonitis secondary to hollow viscus perforation is one of the commonest reasons for emergency surgery done even today. Various factors like age, sex, organ failure, malignancy, extent of peritonitis, type of contamination, site of perforation, surgical interventions are all known to influence mortality and morbidity. Effective preoperative management, timely surgery and proper post-operative care will decide the outcome.
Different studies have mortalities ranging from 6.4% to 17.5% [12–15]. According to the literature MPI is an independent, objective and effective scoring system in predicting mortality and has advantages over the other scoring systems [15–18].
Kusumoto yoshiko et al., evaluated the reliability of the MPI in predicting the outcome of patients with peritonitis in 108 patients. A comparison of MPI and mortality showed patients with a MPI score of 26 or less to have mortality of 3.8%, where as those with a score exceeding 26 had mortality of 41.0% [19].
In a study conducted by Qureshi AM et al., score of < 21 had mortality of 1.9%, score of 21-29 had 21.9% and score > 30 had mortality of 28.1%. Mortality rate for MPI score more than 26 was 28.1% while for scores less than 26 it was 4.3% [20].
Malik AA et al., did prospective study using 101 consecutive patients having generalized peritonitis over a two-year period. In the MPI system, mortality was 0 in the group of patients with a score of less than 15, while it was 4% in the patients scoring 16-25 and 82.3% in those with scores of more than 25 [21].
In our study patients with MPI scores of ≤ 20, 21-29, ≥ 30 had a mortality of 5%, 14%, and 50% respectively. Greatest sensitivity and specificity for the MPI score as a predictor of mortality was at the score of 25. We found, on dividing the patients into two groups around this threshold score a statistically significant difference in mortality with 6.1% mortality for ≤ 25 and 29.5% mortality for MPI > 25 (p=0.03).
In order to quantify the risk of mortality based on MPI scores further analysis was done by grouping the patients around the threshold MPI scores of i) 20 ii) 25 and iii) 29. We found, i) Patients with MPI score > 20 had 5.72 times higher risk of mortality compared to patients with score ≤ 20 (CI 0.63-51.6, p=0.117). ii) Patients with MPI score > 25 had 6.45 times higher risk of mortality than patients with MPI score of ≤ 25 (CI 1.1-37.9, p=0.03). iii) MPI score of > 29 had 10 times increased risk of mortality compared to MPI score ≤ 29 (CI 1.49-66.9, p=0.02). This clearly suggests increasing risk of mortality with increasing MPI score, however to determine if this relationship is linear or exponential a larger study is required.
Conclusion
MPI is disease specific, easy scoring system for predicting the mortality in patients with secondary peritonitis. Increasing scores are associated with poorer prognosis, needs intensive management and hence it should be used routinely in clinical practice.
*Definitions of organ failure: Kidney: creatinine >177 μmol/L, urea >167 μmol/L, oliguria <20 ml/h; Lung: pO2 <50 mmHg, pCO2 >50 mmHg; Shock: hypodynamic or hyperdynamic; Intestinal obstruction (only if profound): Paralysis >24 h or complete mechanical ileus