Fibre Reinforced Composite: Post and Core Material in a Pediatric Patient - An Alternative to Usual
Sonu Acharya1, Shobha Tandon2
1Reader, Department of Pediatric and Preventive Dentistry, Institute of Dental Sciences,SOA University, Bhubaneswar, Orissa, India.
2Former Dean Professor and Head, Department of Pediatric and Preventive Dentistry, Manipal College of Dental Sciences, Manipal, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sonu Acharya, Reader, Department of Pediatric and Preventive Dentistry, Institute of Dental Sciences, SOA University, Bhubaneswar, Orissa, India. Phone : 9937793095,
E-mail: sonu_ain@yahoo.com
Fractured teeth are always a challenge to the dentist. The root canal therapy today can retain even very badly broken teeth. One of the most accepted techniques involve restoration of extensively carious or badly fractured teeth by the fabrication of a post and core while utilizing the root canal space for anchorage. So far, the only materials that are available to the dentist for this procedure have been a variety of metallic alloys. These materials are hard and need to be cast precisely so that they can fit the canals. Today materials are available which usually eliminates all the intermediate steps which are done in laboratories and the total control is rendered in the hands of the dentist, to fabricate on the chair, a resilient, aesthetic and bonded post and core. One such material is discussed here in a pediatric permanent anterior tooth.
Post and core, Fibre-reinforced composite, Pediatric, Ribbond
Case Report
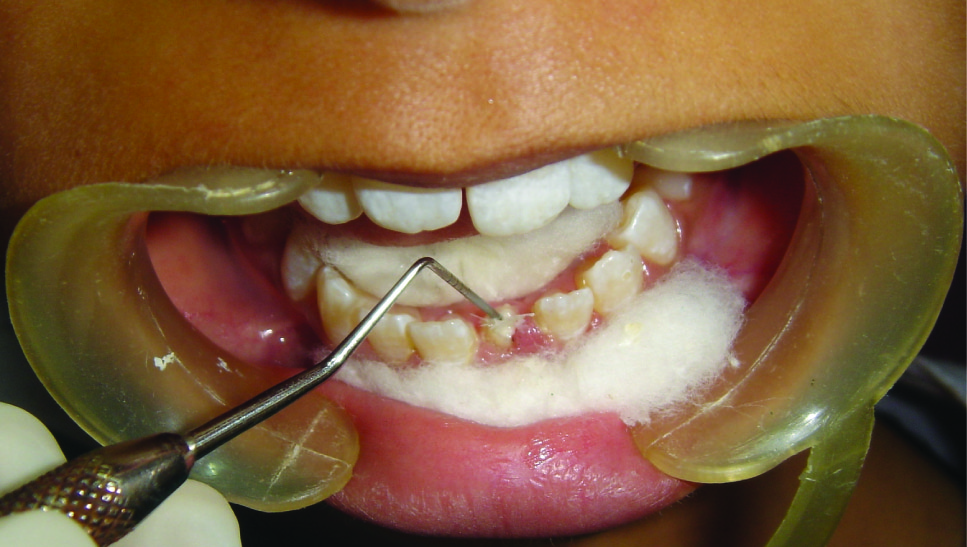
A 12-year-old female patient visited the Department of Pediatric Dentistry with a complain of broken left lower front tooth since four months. The patient did not complain of any pain [Table/Fig-1]. The parent of the patient told that the girl had a fall two years back in which the lower front tooth got broken. There was pain and tenderness reported at that time and they had visited a dentist for the same. On further enquiry it was revealed that the mentioned tooth had been root canal treated six months back and restored but the restoration came out within a month. The re-restoration also did not last more than 15 days. On examination lower left central incisor was fractured and there was neither pain reported nor tenderness to percussion. The tooth structure was less for a composite make-up or a crown. After thorough examination it was decided to go for a post and core and composite make up. As it was an anterior tooth in a young patient it was decided to go for fibre-reinforced composite (Ribbond, Ribbond THM, Ribbond inc.Seattle,WA) as post and core material as it is esthetic and has adequate strength. As the tooth was adequately obturated [Table/Fig-2], preparation of the canal space was done [Table/Fig-3,4]. The use of ribbond does not require additional tooth preparation as is required for metal posts. The remaining tooth structure being less, rubber dam isolation could not be accomplished and we decided for high suction evacuation with cotton rolls to be suitable for isolation. Gutta percha was removed using gutta percha solvent until the desired length for post was achieved. The post hole was shaped using Gates Glidden drills (Roydent, West Palm Beach, FL), cleaned with 5% sodium hypochlorite and dried. The width of Ribbond is to be decided on the root canal space available. The depth of the post space was measured using a periodontal probe, and a 3-mm-wide Ribbond was cut using special scissors provided with the kit (Ribbond starter kit, Ribbond THM, Seattle), measuring twice the depth of the post space and 3–4 times the height of the core build-up [Table/Fig-5] and placed in dual cure adhesive resin and set aside in light protected container. The root canal wall was etched, washed thoroughly and then air-dried gently. Excess water was removed from the post space using paper points . The dual cure adhesive resin (Ed Primer II A&B) was applied using a microbrush and gently air-dried to evaporate the solvent. Dual cure resin cement was then placed inside the canal space. The Ribbond was removed from the resin and the excess resin was removed using a hand instrument [Table/Fig-6], folded in a V-shape and coated with dual-curing resin cement (Panavia, Kuraray Medical Inc., Japan). The piece of ribbond was then placed in the post space in a labial-lingual direction with a periodontal probe [Table/Fig-7]. Excess resin cement was removed, and the cement was cured for 20 s. The two protruding ends of the Ribbond strips formed the reinforcement for the core build up to replace the lost coronal portion of the tooth. The remaining resin mix from the syringe was extruded onto this framework to create a core resembling almost like the shape of a lower central incisor. The space between the protruding ribbon ends was filled with resin so as not to leave any voids. Composite resin was also placed so as to cover the ribbon ends completely and leave none of them exposed on the outer surface of the core. All the material was thoroughly light cured to create a set surface. The material was left in the mouth for a couple of hours to ensure complete set of the self curing component of the resin mix. The result of this procedure came out to be a single piece post and core, which was bonded onto the root, creating a solid structure without any wedging effect on the root. Moreover, the resin conforming to the inside shape of the canal space ensured no voids and eliminated “fitting” problems normally associated with cast posts. The bands of Ribbond reinforced the resin material and made it extremely strong and durable. Bonding of the entire material also created a single block of post and core, which is the essence sought for favourable occlusal force transmission and for resistance against debonding of the entire unit. The best thing was, there was no metal to mask with the crown since the base shade of the composite was a close enough match to the tooth and was translucent. These strips, although opaque, were white in colour and after being completely encased in the composite, were not visible. However, they did not contribute to the colour of the core in any adverse way. The restorative procedure was completed by building up the tooth using dual cure hybrid composite resin following technique of small progressive build up without any matrix [Table/Fig-8,9]. All these increments were fully light cured. Finishing and polishing procedures were performed using composite contouring and polishing discs. The patient was advised for a crown at a later stage after complete development of occlusion. The patient has been under follow up for two years now with six month follow up intervals and the restoration is still in good condition [Table/Fig-10,11]. As because the occlusion is not yet established we have decided to give crown on a later date.
Discussion
Fibre-reinforced composite (FRC) is a bondable, biocompatible, esthetic, translucent and easy-to-use reinforced material. Because of its wide spectrum of properties, it is utilised multiple cases in clinical dentistry. The development of fiber-reinforced composite technology has brought a new material into the arena of metal-free, adhesive esthetic dentistry [1]. The combined use of composite resin and FRC has given significant benefits in terms of mechanical properties as well as the possibility of direct chairside application and the ability of this material to bond to tooth structure, makes it an attractive choice for a variety of dental applications [2,3]. The restoration for an endodontically treated tooth should be as conservative as possible so that it does not increase horizontal and vertical forces on tooth. So far, the only materials that have been available to the dentist for this procedure have been a variety of metallic alloys. These metals which are hard and unyielding have to be cast in the precise shape of the prepared canals and cemented into place. If too tight they can wedge the root and if too loose they can usually come out. Several intermediate steps in their fabrication (impression, poured cast, wax pattern, casting, finishing), are extremely conducive to errors being committed [4]. A recently developed bondable reinforcement fiber, Ribbond, (Ribbond THM, Ribbond inc. Seattle, WA) is reported to be an alternative to conventional post materials because of its esthetic qualities, mechanical properties, and the neutral color of the reinforcing material [5]. First introduced to the market in 1992, Ribbond consists of bondable, reinforced ultra-high-strength polyethylene fibers [1]. The open and lace like architecture of ribbond allows it to adapt closely to the teeth and dental arch. This is an advantage over pre-fabricated fibre posts where the adaptability to root canals is difficult. Apart from this feature the ribbond can be condensed properly in the canals with little microleakage. The incorporation of a fibre layer increases the load bearing capacity of the restoration and prevents crack propagation from the restoration to tooth. When pre-fabricated fibre post is placed in flexure, crack appears on the tensile face and due to brittleness of the material rapidly propagates causing failure [1]. The purpose of using Ribbond as post and core material in the present case report stems from the above said features of Ribbond which made our choice for this material to be used as post and core. FRC can be used in stabilizing traumatized teeth, restoring fractured teeth and creating a fixed partial denture and for direct-bonded endodontic posts and cores, orthodontic fixed lingual retainers and space maintainer [6]. Despite this versatility, there are few reports on the use of Ribbond in pediatric dentistry [7]. The relative flexibility of fibre composite laminate post minimizes crack propagation in the roots. Thus we have a very good option of utilizing Ribbond as post and core material. Compared to preformed posts, there is no additional tooth removal after endodontic treatment. This maintains the natural strength of the tooth, Eliminates the possibility of root perforation because it is made when the Ribbond is in a pliable state, it conforms to the natural contours and undercuts of the canal and provides additional mechanical retention. There are no stress concentrations at the tooth-post interface [7]. The Ribbond post and core is passive and highly retentive. Furthermore, because Ribbond’s translucent fibers take on the color characteristics of the composite it allows for the natural transmission of light through teeth and crowns. This provides an exceptionally esthetic result [1]. The use of fibre-reinforced posts are even better than fibre post systems available as they take less chairside time, better adaptation in canals and less stress induced on tooth structure [7-9]. The biggest advantage of FRC over fibre posts are its manageability and shape memory. FRC can be adapted to any surface of tooth inside or outside. Apart from this the cementation of FRC is easier inside canals than fibre posts [8]. Although, there are so many advantages discussed in favour of FRCs there are certain limitations also [1]. There have been some reported cases of fibre-ribbons being used as post and core material in primary teeth [10-12]. The results suggested that this material is quite good as post and core material when used in primary teeth for pediatric patients. Traumatized permanent anterior teeth in children need quick esthetic and functional repair because of psychological damage they can create in children. Esthetic requirements of most complex cases, can be used in association with fibers so as to improve their mechanical resistance. The authors considered parameters such as physical properties, water absorption, ease of cutting and of laying. Polyethylene fibers appear to have the best properties in elasticity, translucency, adaptability, tenaciousness, resistance to traction and to impact. This material also has been utilized in permanent anterior teeth in adult patients but few have reported the use in children [12]. Hence, we tried to use fiber ribbons as post and core in permanent anterior tooth in a child and obtained reasonably good result. Although many cases have discussed the use of Ribbond as post and core material in primary teeth till date no case has discussed its use in permanent anterior dentition [11,12].

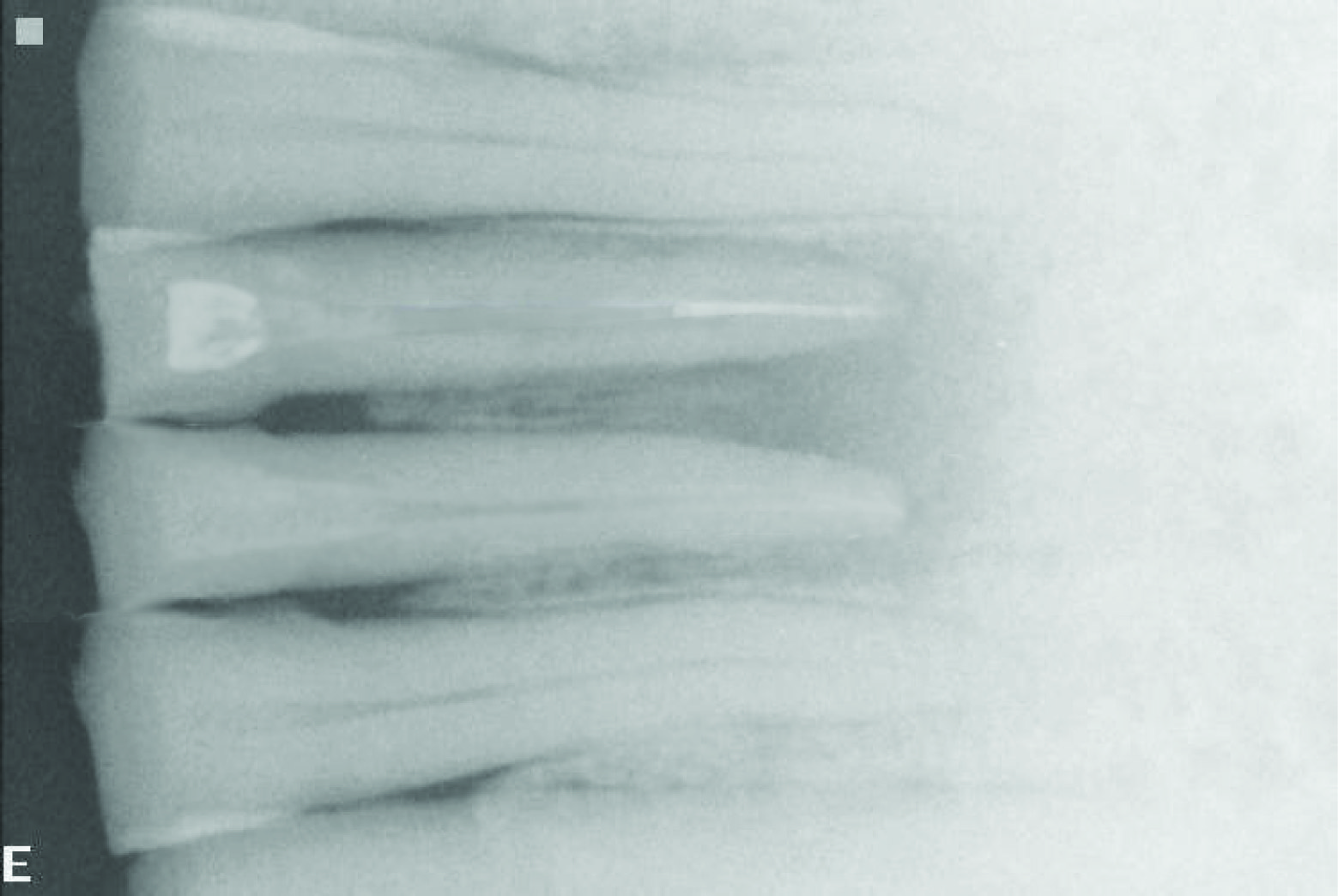
Radiograph showing good obturation
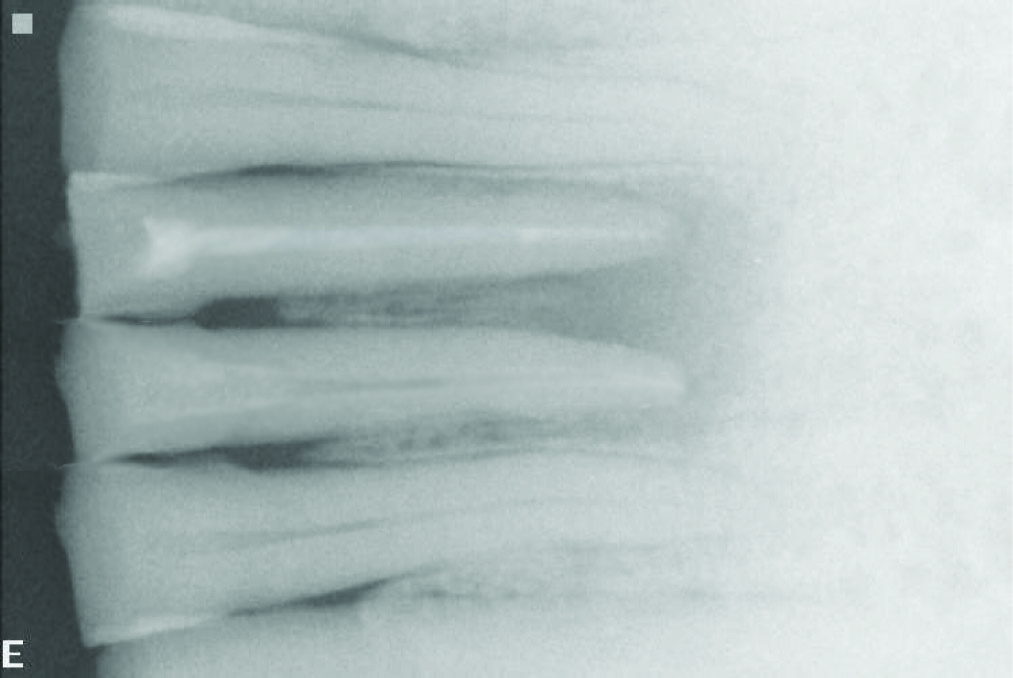
Radiograph showing post space

Measured amount of ribbond prepared

Ribbond prepared to be inserted in canal

Ribbond packed inside canal
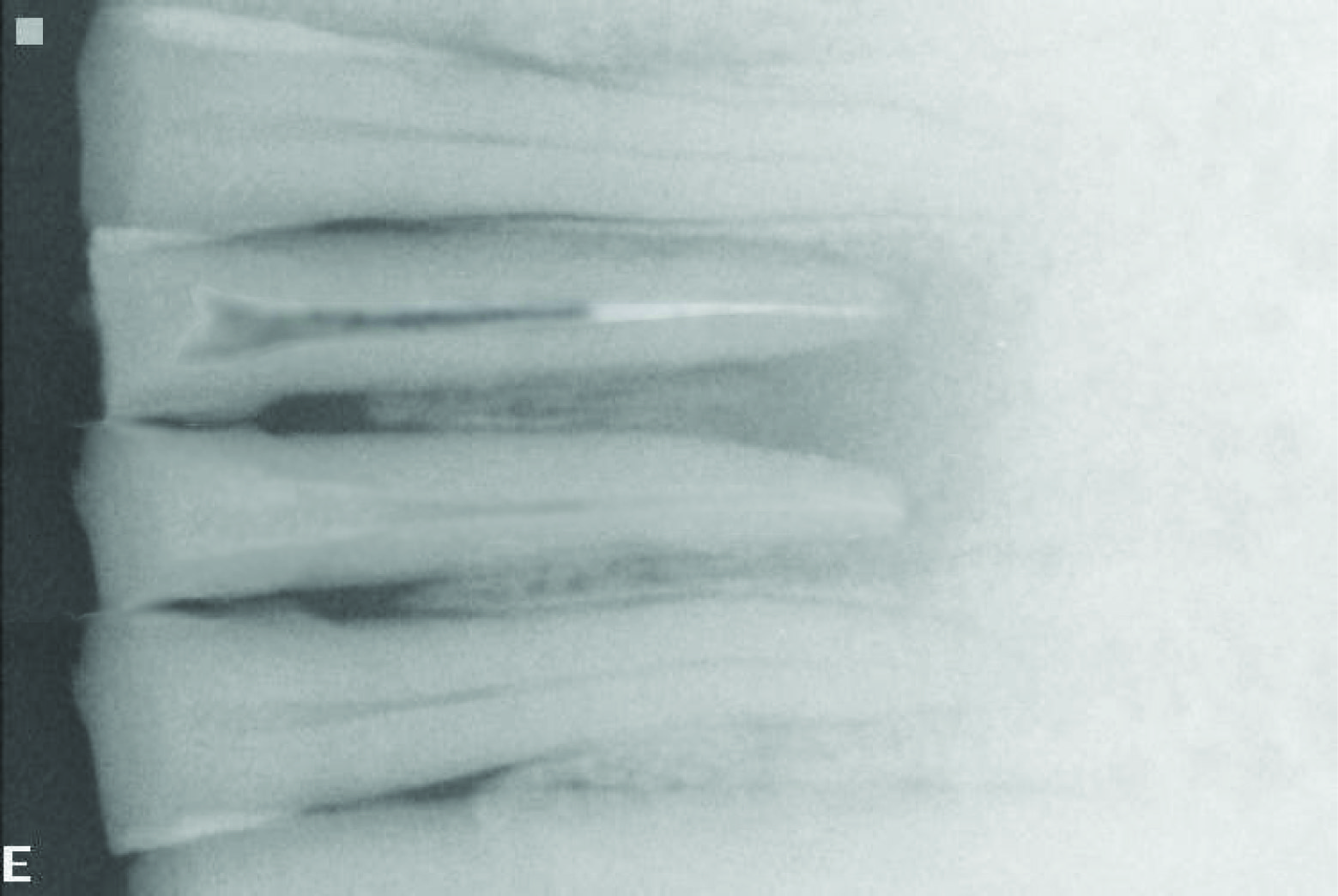
Radiograph showing ribbond inside canal



Conclusion
In recent times the number of endodontic procedures have increased with exceedingly good results. Therefore, restoration of teeth after endodontic treatment is becoming an integral part of the restorative practice in dentistry even when the teeth are in bad shape.This material comes as a boon to the esthetic dentistry. Fibrereinforced composites have been used for similar cases in pediatric dentistry in deciduous teeth but there are very few cases reported for permanent anterior teeth in pediatric patients. The authors have tried to use this as a post and core material in a permanent tooth for a pediatric patient with satisfying esthetic results and improved mechanical properties. Long term follow-up of more cases is required for this material to become more popular especially in pediatric dentistry.
[1]. Ribbond Inc. “Post and Core Restored Tooth after Endodontic Treatment"Dental Products Report 1995 [Google Scholar]
[2]. S Acharya, S Tandon, “Fiber-Reinforced Composites as a Fixed Space Maintainer in Case of Primary Tooth Loss”Compend Contin Edu Dent 2011 32:6 [Google Scholar]
[3]. J Blank, “A Novel Approach for a Single-Tooth Provisional,”Dentistry Today 2012 2:134-39. [Google Scholar]
[4]. M Ganesh, S Tandon, Versatility of ribbond in contemporary practiceTrends Biomater Artif Organs 2006 20:53-58. [Google Scholar]
[5]. MC Vitale, C Caprioglio, A Martignone, U Marchesi, AR Botticelli, Combined technique with polyethlene fibers and composite resins in restoration of traumatized anterior teethDent Traumatol 2004 20:172-77. [Google Scholar]
[6]. B Gerald, M K Gregori, “An Indirect Matrix Technique for Fabrication of Fiber- Reinforced Direct Bonded Anterior Bridges”Compendium 2010 31(1):60-64. [Google Scholar]
[7]. N Adanir, S Belli, O Eraslan, G Eskitascioglu, Effect of post length on stress distribution under functional forces in a glass fibre-post-restored maxillary central incisor modelJ Dent Res 2003 82:253 [Google Scholar]
[8]. Viera CL, Ribeiro CC, Polyethylene fiber tape used as a post and core in decayed primary anterior teeth: a treatment optionJ Clin Pediatr Dent 2001 26(1):1-4. [Google Scholar]
[9]. A Esghi, RK Eshfahan, MA Khorousi, Simple method for reconstruction of severely damaged primary anterior teethDent Res J (Isfahan) 2011 8(4):221-25. [Google Scholar]
[10]. S Bayrak, ES Tunc, N Tuloglu, Polyethylene fiber-reinforced composite resin used as a short post in severely decayed primary anterior teeth: A case reportOral Surg Oral Med Oral Pathol Oral Radiol Endod 2009 107:e60-64. [Google Scholar]
[11]. P Subramaniam, KL Babu, R Sunny, Glass fiber reinforced composite resin as an intracanal post-clinical studyJ Clin Pediatr Dent 2008 32:207-10. [Google Scholar]
[12]. L Verma, S Passi, Glass Fibre-Reinforced Composite Post and Core Used in Decayed Primary Anterior Teeth: A Case ReportCase Rep Dent 2011 :864254 [Google Scholar]