Extra-Oral Approach for Removal of Ectopic Impacted Lower Third Molar: A Case Report
Vandana Shenoy K1, Priya Vishnu2, Kamal Kannadasan3, Srivatsa Kengagsubbiah4, Senthil Kumar5
1 Reader, Department of Oral and Maxillofacial Surgery, Thai Moogambigai Dental College and Hospita, Chennai, India.
2 Reader, Department of Orthodontics, Thai Moogambigai Dental College and Hospital, Chennai, India.
3 Professor and Head, Department of Oral and Maxillofacial Surgery, Thai Moogambigai Dental College and Hospital, Chennai, India.
4 Professor, Department of Oral and Maxillofacial Surgery, Thai Moogambigai Dental College and Hospital, Chennai, India.
5 Reader, Department of Oral and Maxillofacial Surgery, Thai Moogambigai Dental College and Hospita, Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vandana Shenoy K, Reader, Department of Oral and Maxillofacial Surgery, Thai Moogambigai Dental College and Hospita, Chennai-600107, India. Phone : +919962252588, E-mail : drvandanashenoy@yahoo.com
Extra oral approach for removal of the lower third molar is uncommon. This case report illustrates an example of removal of lower third molar by extra-oral approach preserving the inferior dental nerve.
Ectopic lower third molar, Extra-oral approach, Impacted third molar
Case Report
A 38-year-old male was referred to Maxillofacial Surgery Department by an Orthodontist with pain and swelling on the left side of the jaw along with the difficulty of opening the mouth. Pain was sharp, intermittent and radiating to the temple and to the back of the neck. He gave a history of similar episode previously twice and resolved with the antibiotic therapy. On examination swelling was present on the left side near the angle, which was diffused and extending to the neck region. The mouth opening was reduced to 22mm. The OPG [Table/Fig-1] showed obliquely and deeply impacted left third molar (Class 3, Position C) immediately related to the inferior dental nerve and above the angle of the mandible. There was increase in the size of the follicular space associated with the crown of the tooth. Lateral oblique view [Table/Fig-2] shows the mesioangularly impacted third molar which is Class III, positioned 1.5cm distal to the roots of the second molar and close to the left angle with bulky roots. All other teeth on left quadrant were healthy and case was diagnosed to be odontogenic infection from the mesioangular Class III, Position C impacted left lower third molar.
OPG showing impacted left lower left third molar

Lateral Oblique view showing ectopic impacted third molar in the angle of the mandible

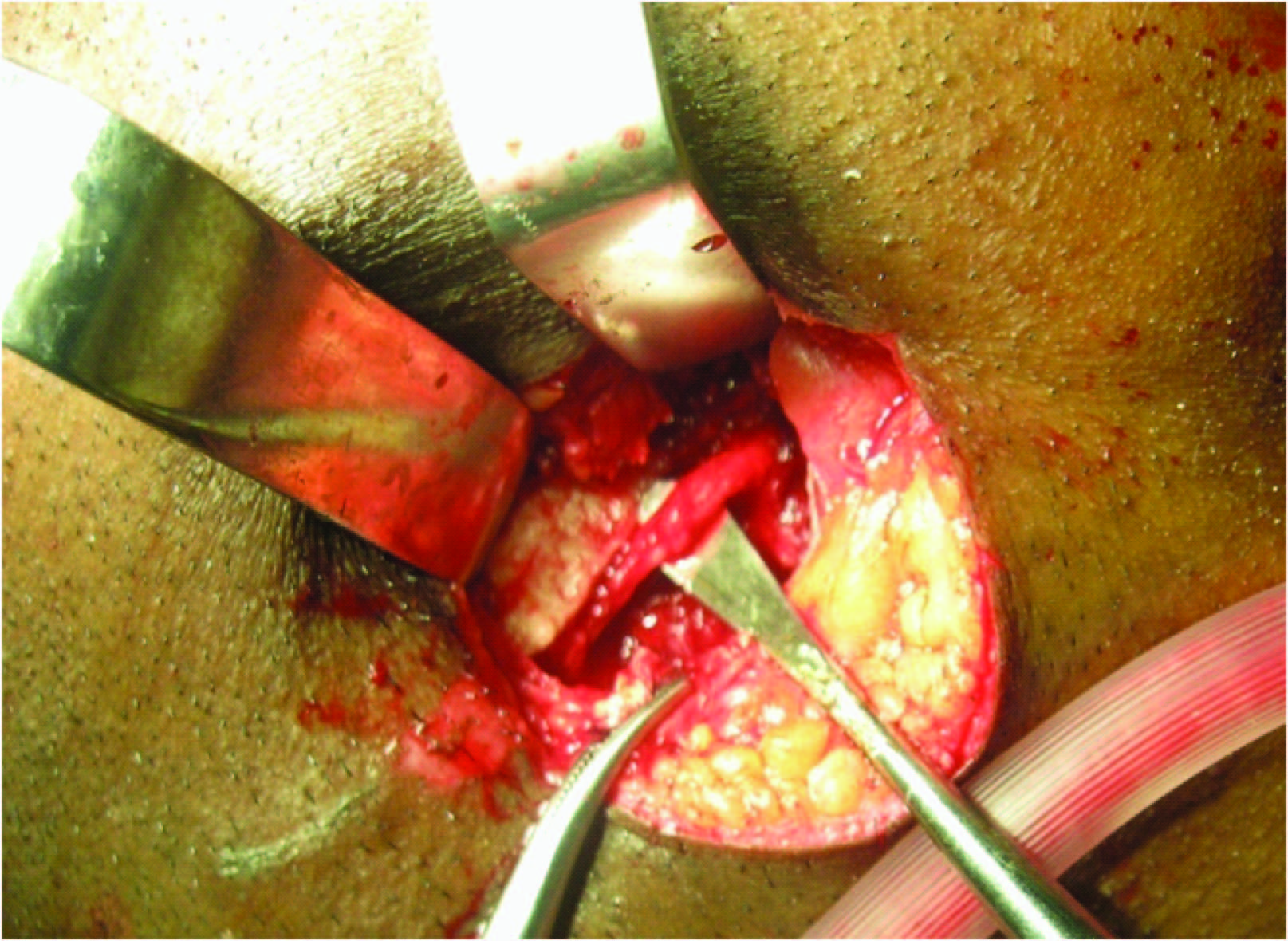
As the patient was continuing with the symptoms, the decision was to remove the impacted ectopically placed mandibular left lower third molar tooth under general anaesthesia with antibiotic cover (Cefotaxim 1gm BD and inj Metronidazole 500mg TID through intravenous route for seven days). As the position was not favourable for trans-oral procedure, extra-oral approach was planned. Patient was taken for extra oral approach after explaining the benefits of procedure which will prevent the damage to the inferior alveolar nerve, possibility of mandibular angle fracture and difficulties arise due to the limited accessibility and visibility to perform the procedure intra orally. The written informed consent was taken prior to general anaesthesia. A standard submandibular approach was used with Risdon incision [Table/Fig-3]. Platysma divided the marginal mandibular nerve branch of facial nerve identified and retracted. After dividing the masseter muscle, through the sub periosteal reflection the lateral surface of the ramus was exposed. The site of impacted tooth presented as smooth elevation, guttering was done using the bur taking the advantage of follicular space crown was exposed. The neurovascular bundle was placed just above the crown of the impacted tooth [Table/Fig-4] carefully dissected out of the canal. The buccal surface of the crown exposed used as a guide for entire tooth removal. The follicle was removed and thoroughly copious irrigation done after smoothing the sharp margins with bur and bone file. Inferior dental nerve replaced in the bed again [Table/Fig-5] and soft tissue closure done in layers. Postoperative recovery was good, and symptom free, mouth opening improved to 53mm on 7th postoperative day. The follicle was sent for histopathologic examination, the report was free of any tumour or cystic transformation.
Extra oral submandibular approach via Risdon’s incision for impacted lower left third molar tooth

Placement of inferior dental nerve superior to the impacted teeth crown position, picture after removal of the teeth

Dissected protected inferior dental nerve which placed back in to the wound bed
Discussion
Impacted mandibular molars occur in 20-30% of the population [1]. The cause for malposition of the tooth is still unclear [2,3]. There have been number of theories put forward for the same. When the tooth is grossly displaced, it may be referred to as ectopic [2,3], for example up into the ramus or down below the level of mandibular nerve. In this case the tooth was found inferio-lingual to the inferior dental nerve in the left angle of the mandible and found to be ectopic [2].
Investigations commonly used for the impacted lower third molar are IOPA and OPG. In our case we used OPG and lateral oblique view of the mandible, impacted lower third molar was placed immediately adjacent to the inferior dental (I D) canal on the left angle and lower border of the mandible. We did not get more information from radiographs, exact position of inferior dental nerve was confirmed only during surgery. CT, 3D CT, would have given more details, but cone beam CT [2,4] nowadays more commonly used to locate the position of an ectopic lower third molar with better resolution and less radiation exposure than conventional CT scans. In our case patient was not financially affordable so further investigations like CT or cone beam CT was not taken to locate the exact position of tooth and its relation to the inferior dental canal.
Pell and Gregory [5] is widely used classification for predicting the difficulty of the removal of lower third molar based on the spatial relationships as revealed by the radiographs with the ramus and the occlusal plane. According to A Garcia Garcia et al., [6], Pell and Gregory classification is unreliable as predictor of difficulty in extracting impacted lower third molars and has little value in clinical practice. In our case the tooth was located in class 3 position C and was ectopic. Impacted mandibular third molars –operative classification by Naaj IA et al., [7] has classified in relation to the mandibular canal and suggested indications for the use of each surgical approach for its extraction. In this operative third molar classification (TMC) [7] TMC III refers to third molars that are completely localized below the mandibular canal. This study suggested TMC III were treated with the extra oral approach. So, when we approached extraorally we found inferior alveolar nerve was just above the crown of the tooth traversing antero-posteriorly. The proximal and distal nerve segments relieved for about 1.5cm from the inferior alveolar canal for better lateralization before removal of left lower third molar.
Surgical approaches [2] to impacted lower third molar are three; they are intra or transoral, extraoral and endoscopically assisted. In transoral conventional method either buccal or lingual approach or sometimes through sagittal split osteotomy procedure. Extra oral approach usually used either submandibular or pre-auricular depending on the location of impacted tooth. In endoscopically assisted techniques fibre optic technology used with endoscope for the surgical removal.
Intra oral approach [2,7] is the most common approach for the lower impacted third molar. Advantageous with this approach is aesthetically good without any extra oral scar. However, in case of deeply impacted teeth there is increased risk of damage to inferior alveolar nerve, significant alveolar bone loss and risk of damaging the adjacent teeth. Intra oral sagittal split osteotomy [2,7,8] is introduced to overcome the extensive removal of alveolar bone. This approach allows direct visualisation and good exposure of the surgical site but incidence of post operative inferior alveolar nerve damage been reported. Endoscope assisted [2,9] surgical approach may not be indicated in all cases because of its limitation, but it is more conservative and gives access to the surgical site which would otherwise be difficult to reach via conventional trans-oral approach. This gives good illumination, magnification of the surgical site, smaller scar and decreased risk of damage to the facial nerve.
Extra oral approach [2,7,10–12] is used in cases where teeth placed high in the ramus, neck of the condyle, sigmoid notch or at the lower border of the mandible. This allows the good exposure, less amount of bone removal and gives three dimensional orientation of the impacted tooth which prevents inadvertent fracture of the mandible. However, there will be minimal external scar and risk to damage the facial nerve branches with this approach. The practice of extraoral approach to remove the impacted tooth is very rare. Going through the literature indications [6,11] for this approaches given as:
Deeply impacted tooth and its very close proximity to the ID canal (in this case), on the lower border or at a higher level at the neck of the condyle.
Deeply imacted tooth with dilacerated and hypercementosed roots
In cases of severe trismus
Third Molar Classification (TMC) III like in our case.
Conclusion
Prior to the removal of lower third molars which are placed under TMC III, it is mandatory to educate the patient regarding the extraoral approach under general anaesthesia for better completion of the procedure. A meticulous handling of inferior dental nerve (IDN) and extra oral soft tissues and skin will invariably recover absolutely without any morbidity.
[1]. Andersen JO, Petersen JK, Laskin DM, Textbook and color atlas of tooth impactions1st edSt. LouisMosby year book:222-26. [Google Scholar]
[2]. Ahmed NM, Speculand B, Removal of ectopic mandibular third molar teeth: literature review and a report of three casesOral Surgery 2012 5:39-44. [Google Scholar]
[3]. Lee YK, Park SS, Myoung H, Surgical extraction of mandibular third molar in pterygomandibular space: a case reportJ Korean Assoc Oral Maxillofac Surg 2013 39:242-45. [Google Scholar]
[4]. Bortoluzzi CM, Manfro R, Treatment for ectopic third molar in the subcondylar region planned with cone beam computed tomography: a case reportJ Oral Maxillofac Surg 2010 68:870-72. [Google Scholar]
[5]. Hupp JR, Ellis E III, Tucker MR, Contemporary Oral and Maxillofacial Surgery 2011 5th edElesevier publication Reprint:160-64. [Google Scholar]
[6]. García GA, Sampedro FG, Rey JG, Vila PG, Martin SM, Pell–Gregory classification is unreliable as a predictor of difficulty in extracting impacted lower third molarsBr J Oral Maxillofac Surg 2000 38:585-87. [Google Scholar]
[7]. Naaj IA, Braun R, Leiser Y, Peled M, Surgical approach to impacted mandibular third molars-operative classificationJ Ora Maxillofac Surg 2010 68:628-33. [Google Scholar]
[8]. Jones TA, Garg T, Monaghan A, Removal of a deeply impacted mandibular molar through a sagittal split ramus osteotomy approachBr J Oral Maxillofac Surg 2004 42:365-68. [Google Scholar]
[9]. Cunqueiro SMM, Schoen R, Schramm A, Gellrich NC, Schmelzeisen R, Endoscopic approach to removal of an ectopic mandibular third molarBr J Oral Maxillofac Surg 2003 41:340-42. [Google Scholar]
[10]. Singh Y K, Adamo AK, Parikh N, Buchbinder D, Transcervical removal of an impacted third molars: an uncommon indicationJ Ora Maxillofac Surg 2014 72:470-73. [Google Scholar]
[11]. Milner N, Backer A, Extraoral removal of lower third molar toothBritish Dental Journal 2005 199:345-46. [Google Scholar]
[12]. Wang CC, Kok SH, Hou LT, Yang PJ, Lee JJ, Cheng S J, Kuo RC, Chang HH, Ectopic mandibular third molar in the ramus region : report of a case and literature reviewOral Surg Oral Med Oral Pathol Oral Radiol Endod 2008 105:155-61. [Google Scholar]