Context: Low socio-economic group patients from rural areas often opt for free cataract surgeries offered by charitable organisations. SICS continues to be a time tested technique for cataract removal in such patients. In recent times, camp patients are sometimes treated by clear corneal phacoemulsification with implantation of a rigid IOL, which being more cost effective is often provided for camp patients. This study was undertaken to find out which surgical technique yielded better outcomes and was more suited for high volume camp surgery.
Aim: To find the better surgical option- phacoemulsification with rigid IOL or SICS, in poor patients from rural areas.
Settings and Design: A prospective randomised controlled trial of cataract patients operated by two different techniques.
Materials and Methods: One hundred and twelve eyes were selected and were randomly allocated into two groups of 56 eyes each. At completion of the study, data was analysed for 52 eyes operated by clear corneal phacoemulsification and implantation of a rigid IOL, and 56 eyes operated by SICS.
Statistical Analysis Used: Unpaired t-test was used to calculate the p- value.
Results: The results were evaluated on the following criteria. The mean post-operative astigmatism at the end of four weeks
- was significantly higher in phacoemulsification group as compared to SICS group
The BCVA (best corrected visual acuity) at the end of four weeks
- was comparable in both groups.
Subjective complaints and/ or complications: In phaco group two patients required sutures and seven had striate keratitis , while none in SICS group. Complaint of irritation was similar in both groups. Surgical time- was less for SICS group as compared to phaco group.
Conclusion: SICS by virtue of being a faster surgery with more secure wound and significantly less astigmatism is a better option in camp patients from rural areas as compared to phacoemulsification with rigid IOL.
Introduction
Cataract mostly being an elective surgery, many poor patients from rural areas choose to get operated in the free camps that are organised by charitable organisations. While SICS by virtue of being fast, safe and non-machine dependent, continues to be a preferred option by surgeons, in many centres where phacoemulsification is being done routinely, surgeons do a clear corneal phaco, enlarge the incision and put a rigid IOL which, by virtue of being more cost effective than a foldable IOL, is mostly provided for charitable camps. Also, many patients from rural areas do not adhere to the follow up schedule or the postoperative precautions and treatment. This study was undertaken to find out the preferred surgical option in such patients - Clear corneal phaco emulsification with implantation of a rigid IOL, versus SICS with respect to visual outcome and safety.
Materials and Methods
One hundred and twelve eyes were selected from rural patients admitted in our IPD over a period of three months November 2013 to January 2014. Criteria for selection were- clear corneas, cataract of not more than grade three, no or minimal (0.25D) with the rule astigmatism, and no other ocular disease. All patients were between the ages of 45 to 78 years. Patients were divided by simple random sampling into Group A- Phacoemulsification group- 56 eyes, and Group B-SICS group – 56 eyes.
Informed consent was taken from all patients prior to surgery.
Patients in Group A were operated by clear corneal superior (11o’clock) phaco incision of 2.8mm, which was enlarged to 5.2mm at the end of surgery and a rigid 5.25 mm lens was implanted.
Patients in Group B were operated with SICS- a superior straight incision 1.5mm from the limbus was used, extending it to 5.5 to 6.5 mm at the end of surgery, and implanting a rigid 5.25mm IOL.
All operations were done by the same surgeon (author).
The patients were followed up on day one, week 1, and week 4 following surgery. Four patients from Phaco group A did not complete the follow up schedule, and were therefore excluded from the study
Patients were evaluated on the following criteria:
1. Surgically induced postoperative astigmatism at week 4.
2. Best corrected visual acuity at week 4.
3. Any subjective complaints and/or complications during and following the surgery.
Statistical Analysis Used
Unpaired t-test was used to calculate the p-value.
Results
The mean surgically induced astigmatism at the end of four weeks in Group A (Phaco group) was 2.06D; (SD=0.52D), while the mean astigmatism in Group B (SICS group) was 0.98D (SD=0.39D).
The p-value was calculated using the unpaired t test, and it was p= < 0.0001 which was statistically significant.
The best corrected visual acuity in the two groups at the completion of four weeks was
- 47/52 patients (90.38%) had 6/18 or better vision in Phaco group, as compared to 53/56 (92.85%) patients in SICS group.
Complications and/or subjective complaints following surgery- Two patients in the phaco group required suturing for secure wound closure, while none in the SICS group required sutures.
Striate keratits was seen in seven patients in Phaco group A which resolved within 1 week with standard treatment, while none in SICS group B had striate keratitis.
Complaints of grittiness and foreign body sensation were similar in both groups with 23/52 patients (44%) complaining of these symptoms in phaco group as compared to 27/56 patients (48.2%) in SICS group.
The average operative time in the Phaco group was 16 min as compared to 10 min in the SICS group.
Discussion
Cataract remains a major cause of visual impairment in India, and free, hospital based cataract surgery camps continue to be held to deal with the problem [1]. Rural patients opting for charitable cataract surgeries present multiple challenges to the surgeon. Most patients are elderly and illiterate, and come with a mind-set of free and quick surgery [2-4]. Besides being a high volume surgery, ensuring adherence to follow up schedule and medication/ hygiene requires constant supervision and high vigilance on the part of the care giver. Other studies have emphasised the need to improve long term follow up of rural patients with regular monitoring, and to not only increase surgical volume, but to also improve the qualitative aspect of cataract surgery outcome [5-8].
Phacoemulsification and SICS are both good options for high volume camp surgery. But rigid IOLs are generally made available for camp patients, being more cost effective as compared to foldable IOLs. In such a scenario, a surgical option that is faster, safer, and gives good visual outcome will be the preferred one.
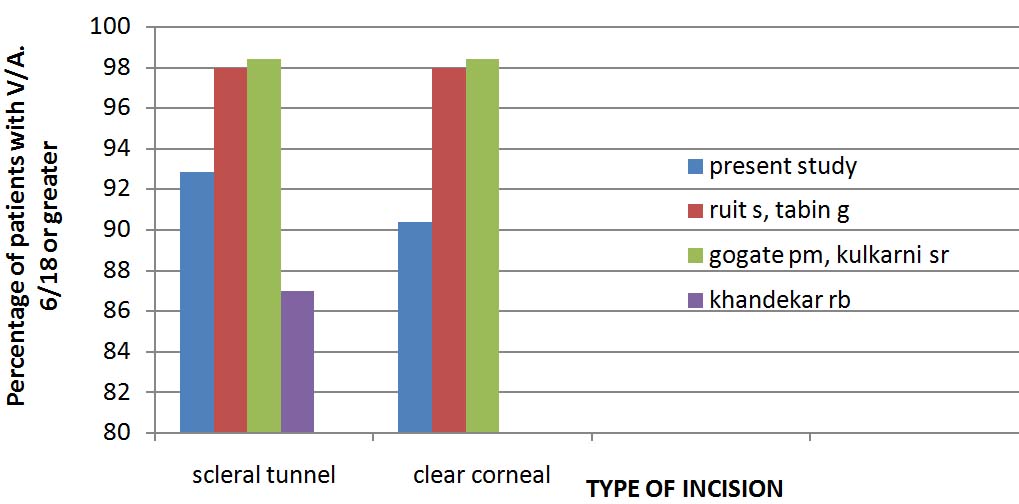
It is established that the smaller phacoemulsification wound gives lesser astigmatism than ECCE [9,10]. Of studies comparing phacoemulsification to SICS, Ruit S, Tabin G, et al., [11] compared the efficacy and visual results of phacoemulsification vs. SICS for the treatment of cataracts in Nepal. While both procedures gave similar visual results (98% patients in both groups achieving BCVA of 6/18 or better at 6 months), they concluded that SICS is significantly faster, less expensive, and less technology dependent than phacoemulsification. Similar result was obtained in our study. [Table/Fig-1].
In a study in central India [12] analysing data of SICS retrospectively, they concluded that 87% patients had BCVA of 6/18 or better six weeks after surgery [Table/Fig-1] .
Gogate PM, Kulkarni SR, [13] compared the safety and efficacy of phacoemulsification with manual small-incision cataract surgery by a randomized controlled clinical trial. They concluded that both the techniques are safe and effective for visual rehabilitation of cataract patients (98.4% patients in both groups achieving a BCVA of 6/18 or better at six weeks), but phacoemulsification gives better uncorrected visual acuity in a larger proportion of patients at 6 weeks [Table/Fig-1].
A study conducted in Nepal by Hennig A et al., [14] compared the results of phacoemulsification done using foldable versus rigid IOL’s, in which the foldable lens was inserted using a 2.5mm clear corneal incision, while the rigid lens was inserted using a 5mm sclerocorneal incision. They found no significant difference in the visual outcome of phacoemulisfication using either a rigid intraocular lens (PMMA PC IOL) or a foldable PC IOL (hydrophilic acrylic). But the cost of foldable IOL was mentioned as eight times higher than a rigid IOL. In our study in which the phaco incision was being enlarged to 5.2mm (clear corneal) at the end of surgery, visual results were similar in both groups but post-operative astigmatism was significantly higher in the phacoemulsification with rigid IOL group.
Also, in our study in both groups the astigmatism noted was against the rule, which corroborates well with similar findings of a study by Reddy B et al., [15]. Mallik VK et al., [16] comparing superior vs temporal scleral tunnel incisions, found the superior incisions to give higher degrees of astigmatism, with a mean of 1.45D. The mean astigmatism in our study from superior sclerocorneal tunnel was found to be 0.98D.
In another study by Olsen T et al., [17] comparing clear corneal and scleral tunnel incisions in phacoemulsification, they concluded that clear corneal incisions yielded higher postoperative astigmatism [Table/Fig-2]. Similar result was obtained in our study.
Another study [18] using 4mm and 6.5mm scleral tunnels to implant foldable and rigid IOLs respectively after phacoemulsification, reported SIA of 0.98D and 1.44D at the end of one month, which correlates well with our study, difference being that we have compared a scleral tunnel incision in SICS with a clear corneal phaco incision [Table/Fig-2].
In a study carried out in Rohtak (India) [19], comparing sclerocorneal and clear corneal tunnel incisions in cataract surgery (SICS), the mean SIA at one month was 2.03D in clear corneal tunnels and 1.35 D in sclerocorneal tunnels, and they concluded that safety and visual acuity was better with sclero-corneal incision a finding which corresponds well with our study [Table/Fig-2].
While no cases in our study had post- operative enophthalmitis, a study by Cooper et al., [20] comparing the safety of clear corneal to scleral tunnel incisions concluded that clear corneal incisions were found to be a statistically significant risk factor for acute postcataract surgery endophthalmitis when compared with scleral tunnel incisions.
Showing BCVA after cataract surgery, comparing present study with previous studies [11,12,13]
Showing postoperative astigmatism after cataract surgery with different site and size of incision [17-19]
| Name of study | Type of surgery | Sample size | Site of incision | Size of incision | Post-operative astigmatism |
| Archana S Khurana AK [19] 2011 | SICS (rigid IOL) SICS (rigid IOL) | 60 | Clear corneal Sclero corneal | 6mm 6mm | 2.03D (at 1month) 1.35D (at 1month) |
| Steinert RF Brint SF [18] 1991 | Phaco (foldableIOL) Phaco (Rigid IOL) | 130 | Sclerocorneal Sclerocorneal | 4mm 6.5mm | 0.98D (at 1month) 1.44D (at 1month) |
| Olsen T Dam Johansen 1997 [17] | Phaco (foldableIOL) Phaco (foldableIOL) | 100 | Clear corneal Sclero corneal | 3.5-4mm 3.5-4mm | 0.72D (at 6 months) 0.36D (at 6 months) |
| Present study 2014 | SICS( rigid IOL) Phaco (rigid IOL) | 108 | Sclerocorneal Clearcorneal | 5.5-6.5mm 5.25mm | 0.98D (at 1month) 2.06D (at 1month) |
Conclusion
SICS may be the more appropriate surgical procedure for the treatment of cataract in high volume camp surgery of rural, low socio economic group patients in the developing world as compared to clear corneal phaco with rigid IOL. It is quicker, cost effective, and gives good visual results, while being non machine dependent. Enlarging the clear corneal incision to implant a rigid IOL is not a good surgical option, as it gives higher astigmatism, as well as a less secure wound. SICS should be the preferred option in rural patients who cannot afford a foldable IOL.
[1]. H Limburg, R Kumar, D Bachani, Monitoring and evaluating and cataract intervention in IndiaBr J Ophthalmol 1996 80:951-55. [Google Scholar]
[2]. RD Thulasiraj, R Rahamathulla, A Saraswati, S Selvaraj, LB Ellwein, The Sivaganga eye survey: I. Blindness and cataract surgeryOphthalmic Epidemiol 2002 9:299-312. [Google Scholar]
[3]. PK Nirmalan, RD Thulasiraj, V Maneksha, R Rahmathullah, R Ramakrishnan, A Padmavathi, A population based eye survey of older adults in Tirunelveli district of south India: blindness, cataract surgery and visual outcomesBr J Ophthalmol 2002 86:505-12. [Google Scholar]
[4]. SK Gupta, GVS Murthy, Where Do Persons With Blindness Caused by Cataracts in Rural Areas of India Seek Treatment and Why?Arch Ophthalmol 1995 113(10):1337-40. [Google Scholar]
[5]. R Anand, A Gupta, J Ram, U Singh, R Kumar, Visual outcome following cataract surgery in rural PunjabIndian J Ophthalmol 2000 48:153-58. [Google Scholar]
[6]. Lindfield Robert, Vishwanath Mehta, Ngounou Kalluru, Khanna Rohit C, The challenges in improving outcome of cataract surgery in low and middle income countriesIndian J Ophthalmol 2012 60(5):464-69. [Google Scholar]
[7]. H Limburg, A Foster, K Vaidyanathan, GVS Murthy, Monitoring visual outcome of cataract surgery in IndiaBull WHO 1999 77(6):455-60. [Google Scholar]
[8]. GV Murthy, LB Ellwein, S Gupta, K Tanikachalam, M Ray, VK Dada, A populationbased eye survey of older adults in a rural district of Rajasthan: II. Outcomes of cataract surgeryOphthalmology 2001 108(4):686-92. [Google Scholar]
[9]. A Watson, P Sunderraj, Comparison of small incision pharoemuloification with standard extracapsular cataract surgery: post-operative astigmation and visual recoveryEye 1992 6:626-29. [Google Scholar]
[10]. L Werblin, PJ Sheridan, Astigmation after cataract extraction: 6 year follow up of 6.5 and 12 mm incisionsRefract Corneal Surg 1992 8:448-58. [Google Scholar]
[11]. S Ruit, G Tabin, D Chang, L Bajracharya, DC Kline, W Richheimer, A prospective randomized clinical trial of phacoemulsification vs manual sutureless small-incision extracapsular cataract surgery in NepalAm J Ophthalmol 2007 143(1):32-38. [Google Scholar]
[12]. RB Khandekar, BK Jain, AK Sudhan, KP Pandey, Visual acuity at 6 weeks after small incision cataract surgery and role of audit in predicting visual acuityEur J Ophthalmol 2010 20(2):345-52. [Google Scholar]
[13]. PM Gogate, SR Kulkarni, S Krishnaiah, RD Deshpande, SA Joshi, A Palimkar, Safety and efficacy of phacoemulsification compared with manual smallincision cataract surgery by a randomized controlled clinical trial: six-week resultsOphthalmology 2005 112(5):869-74. [Google Scholar]
[14]. A Hennig, LR Puri, H Sharma, JR Evans, D Yorston, Foldable vs rigid lenses after phacoemulsification for cataract surgery: a randomised controlled trialEye (Lond) 2014 28(5):567-75. [Google Scholar]
[15]. B Reddy, A Raj, VP Singh, Site of Incision and Corneal Astigmatism in Conventional SICS versus PhacoemulsificationAnn Ophthalmol 2007 39(3):209-16. [Google Scholar]
[16]. VK Mallik, S Kumar, R Kamboj, C Jain, K Jain, S Kumar, Comparison of astigmatism following manual small incision cataract surgery: superior versus temporal approachNepal J Ophthalmol 2012 4(1):54-58. [Google Scholar]
[17]. T Oslen, M Dam- Johanson, T Bek, JO Hjortdal, Corneal versus scleral tunnel incision in cataract surgery: a randomized studyJ Cataract Refract Surg 1997 23:337-41. [Google Scholar]
[18]. RF Steinert, SF Brint, SM White, IH Fine, Astigmatism after small incision cataract surgery. A prospective, randomized, multicenter comparison of 4- and 6.5-mm incisionsOphthalmology 1991 98(4):417-23. [Google Scholar]
[19]. S Archana, AK Khurana, U Chawla, A comparative study of sclero-corneal and clear corneal tunnel incision in manual small-incision cataract surgeryNepal J Ophthalmol 2011 3(1):19-22. [Google Scholar]
[20]. BA Cooper, NM Holekamp, G Bohigian, PA Thompson, Case-control study of endophthalmitis after cataract surgery comparing scleral tunnel and clear corneal woundsAm J Ophthalmol 2003 136(2):300-05. [Google Scholar]