A Novel Esthetic Approach using Connective Tissue Graft for Soft Tissue Defect Following Surgical Excision of Gingival Fibrolipoma
Aruna Balasundaram1, Harinath Parthasarathy2, Praveenkrishna Kumar3, Priyalochana Gajendran4, Devapriya Appukuttan5
1 Professor, Department of Periodontics, SRM Dental College and Hospital, Ramapuram, Chennai, India.
2 Professor, Department of Periodontics, SRM Dental College and Hospital, Ramapuram, Chennai, India.
3 Post Graduate, Department of Periodontics, SRM Dental College and Hospital, Ramapuram, Chennai, India.
4 Post Graduate, Department of Periodontics, SRM Dental College and Hospital, Ramapuram, Chennai, India.
5 Lecturer, Department of Periodontics, SRM Dental College and Hospital, Ramapuram, Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Aruna Balasundaram, SRM Dental College and Hospital, Ramapuram, Chennai-89, India. Phone : 9840162966, E-mail : bbaallaa2002@yahoo.co.in
The aim of the present case report is to evaluate the adjunctive use of a connective tissue graft to overcome soft tissue defects following excision of a gingival fibrolipoma in the aesthetic region. Connective tissue graft has been well documented for treating defects of esthetic concern. However, the literature does not contain many reports on the esthetic clinical outcome following the use of connective tissue graft secondary to excision of soft tissue tumours. A 28-year-old male patient reported with a complaint of a recurrent growth in relation to his lower front tooth region. The lesion which was provisionally diagnosed as fibroma was treated with a complete surgical excision, following which a modified coronally advanced flap and connective tissue graft was adopted to overcome the soft tissue defect. The excised growth was diagnosed histologically as fibrolipoma. One year follow up showed no recurrence of the lesion and good esthetics.The adjunctive use of the connective tissue graft and modified coronally advanced flap predictably yields optimal soft tissue fill and excellent esthetics. Hence, routine use of this procedure may be recommended for surgical excision of soft tissue growths in esthetically sensitive areas.
Connective tissue graft, Esthetics, Fibrolipoma, Keratinised gingiva, Modified coronally advanced flap
Case Report
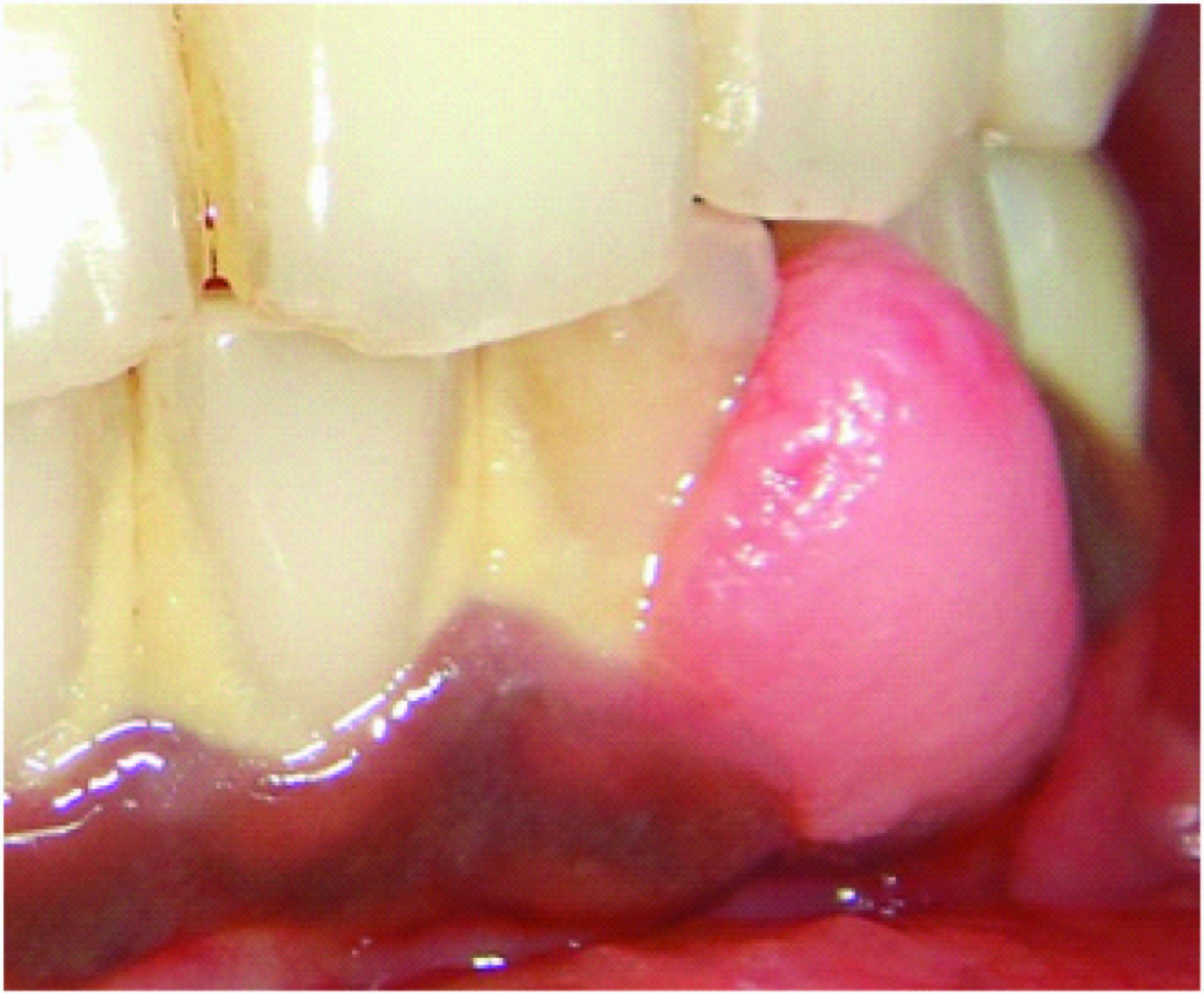
A 28-year-old systemically healthy, male patient reported to the Department of Periodontology, SRM Dental College, Chennai, India, with the chief complaint of painless, non-bleeding, gradually increasing growth in relation to his lower front teeth for the past one year. The patient gave a history of a similar growth in the same region four years back, which was diagnosed histopathologically as a fibro-epithelial polyp and managed by surgical excision. On intra oral clinical examination, a single painless oval shaped well circumscribed growth, measuring about 9 mm by 12 mm in the inter dental region of 32 and 33 involving the buccal attached gingiva and interdental papilla was noticed. The overlying mucosa was pale pink in color with a smooth surface. The growth was soft to firm in consistency, immobile, sessile and non-tender on palpation with spacing between 32 and 33 as shown in [Table/Fig-1]. Based on the patient’s history and clinical findings the lesion was provisionally diagnosed as a fibroma. A treatment plan comprising of complete phase I therapy and surgical excisional biopsy of the growth was proposed. Additionally, we planned for a connective tissue graft to manage the anticipated esthetic compromise. Informed consent was obtained from the patient.
Baseline picture of fibrolipoma in relation to 32 and 33 region
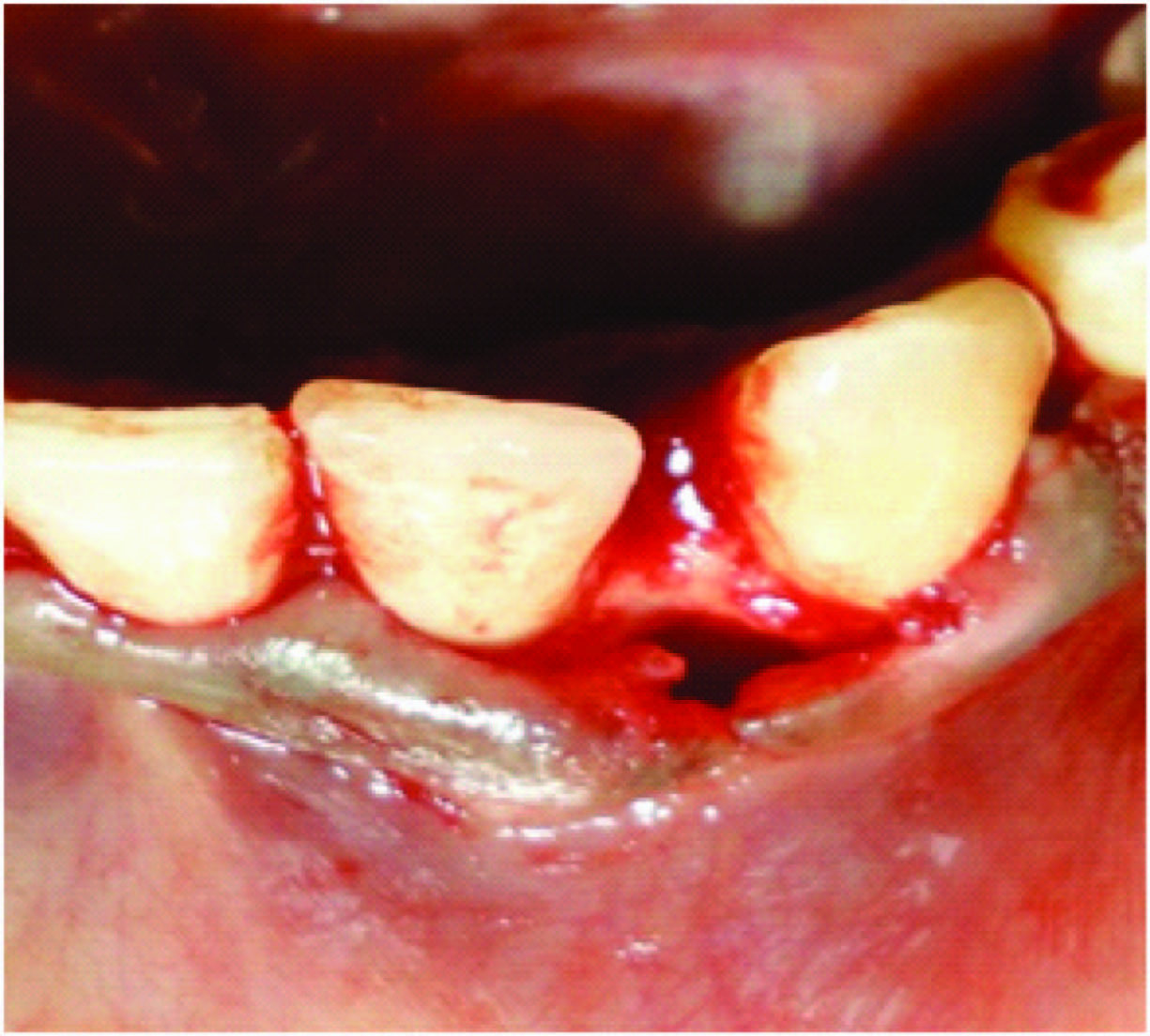
Under aseptic conditions, after achieving adequate local anaesthesia an incision was given extending 2mm beyond the growth on the facial side and continued as interdental incisions between 32 and 33 and completed with a paracrestal incision on the lingual side. A complete excision of the growth was achieved along with the periosteum which was immediately transferred to a container with 10% buffered formalin for routine histopathological evaluation. The surgical excision led to a soft tissue defect in the interdental area as shown in [Table/Fig-2]. To overcome this, a full thickness flap was elevated from the mid-buccal region of tooth number 31 to 34 extending upto and beyond the mucogingival junction. On the lingual side the incisions were limited to the adjacent teeth and were not extended. The root surface was planed and granulation tissue was debrided. Following this, the previously elevated buccal full thickness flap was further continued as a split thickness flap so as to achieve coronal displacement with tension free suturing. A connective tissue graft of optimal thickness [Table/Fig-3] was harvested from the palate and was placed in the interdental area between 32 and 33. The buccal flap was advanced coronally over the CTG and stabilized with 4-0 vicryl interdental direct sutures as shown in [Table/Fig-4]. Periodontal dressing was placed and the patient was given routine postsurgical medications and instructions.The patient was followed for a period of one year which showed satisfactory esthetic outcome without any recurrence of the tumour as shown in [Table/Fig-5].
Soft tissue defect following excision of fibrolipoma
Harvested connective tissue graft
Modified coronally advanced flap sutured over connective tissue graft

One year follow up showing no recurrence of the growth with adequate gingival thickness and keratinized tissue

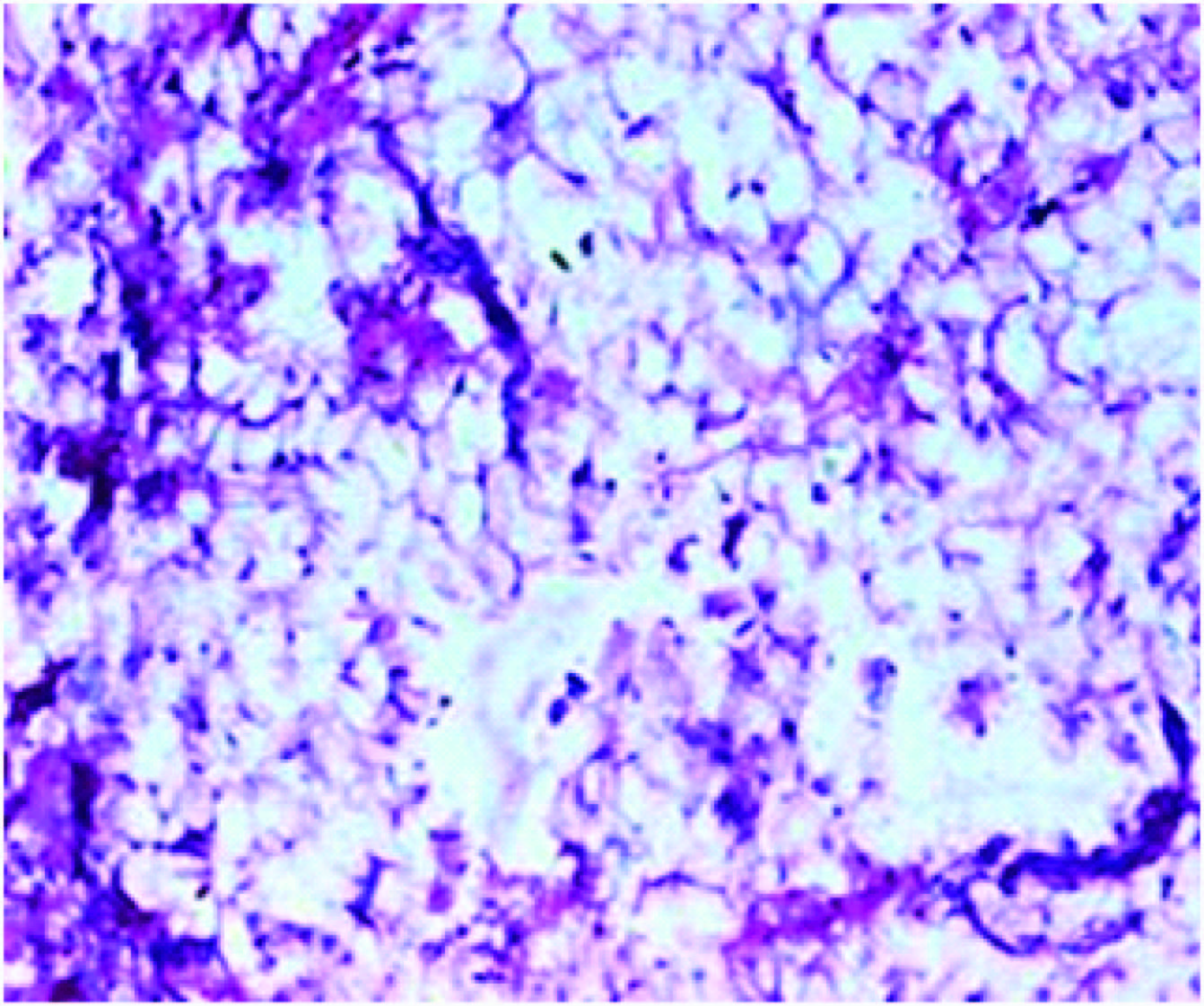
Histopathological analysis of the excised tissue revealed circumscribed mass of connective tissue comprising of dense collagen fibers with relatively less inflammation covered by para-keratinised stratified squamous epithelium. Interestingly collection of fat cells was seen in the connective tissue separated by thin fibrous septa and the above findings were suggestive of fibrolipoma as shown in [Table/Fig-6].
Histopathological picture showing collection of fat cells separated by thin fibrous septa
Discussion
Lipoma is a benign tumour composed of mature fat cells and arises from the superficial soft tissues [1], representing by far the most common mesenchymal neoplasm, with rare occurrence in the oral cavity accounting to 1-4% [2]. A fibrolipoma is a fibrous tumour that contains fatty material [3], which can occur due to fatty degeneration of fibromas and also due to lipogenesis observed in fibroblasts. Although fibrolipoma of oral cavity has been documented in the literature, its occurrence in the gingiva is rare [4]. Occurrence of such gingival tumours in the anterior maxillary and mandibular region is of greater clinical importance as it compromises esthetics, phonetics, mastication, and interferes with routine oral hygiene maintenance. The conventional treatment for fibroma is complete excision and curettage [5]. In the present case report, the lesion was clinically diagnosed as fibroma, as it appeared as a smooth surfaced sessile pink firm growth but histologically it was confirmed as fibrolipoma a variant of lipoma [1]. The patient gave a history of similar lesion in the same site four years back which was excised using electrocautery. Currently to prevent recurrence, a surgical method to completely excise the lesion along with the underlying periosteum was planned and executed; such excisions usually result in compromised esthetics and gingival contour which favour plaque accumulation. To overcome such defects, an additional use of connective tissue grafts (CTG) is frequently recommended to predictably increase the soft tissue volume and optimal esthetic outcome.
In this current case the treatment plan included complete surgical excision of the lesion and Modified Coronally Advanced Flap (MCAF) with Connective Tissue Graft(CTG) for esthetic management. The initial step in the surgical treatment was complete excision of the lesion.
John et al., [6] presented a series of three cases with peripheral ossifying fibroma of the gingiva, which were treated by surgical excision of the lesion followed by complete removal of the underlying soft tissue including the periosteum. A similar method of excision was done in our case to prevent the further recurrence of this lesion. CTG has been documented for managing soft tissue esthetics, for increasing the thickness of the soft tissue [6–8] and width of attached gingival [9]. In our case, the excision of the lesion led to a large soft tissue defect with only a minimal amount of keratinized gingiva and no attached gingiva, inorder to overcome this, a connective tissue graft was used. Zucchelli et al., [10] reported the use of a connective tissue platform for soft tissue augmentation in which an envelope technique was used and horizontal incisions were extended to the adjacent teeth on either side of the defect for coronally advancing the flap. This technique was a modification of coronally advanced flap (MCAF) whereby vertical incisions were not used [11]. As the defect was in the aesthetic region, the use of conventional coronally advanced flap technique would lead to discrepancies in the contour of gingival margin after healing. Additionally a recent systematic review [12] concluded that the use of MCAF provides superior results than a regular coronally advanced flap with vertical releasing incisions. Hence in the present study MCAF was used.
Conclusion
To conclude, the adjunctive use of the CTG and MCAF predictably yields excellent soft tissue esthetics and routine use of this procedure may be recommended for surgical excision of soft tissue growths in esthetically sensitive areas.
[1]. Weiss SW, Goldblum JR, Enzinger and Weiss’s soft tissue tumours. F. M. Enzinger 2008 5th edElsevier Health Sciences Division:430-36. [Google Scholar]
[2]. Manjunatha BS, Patel GS, Shah V, Oral fibrolipoma-a rare histological entity: report of 3 cases and review of literatureJ Dent 2010 7:226-31. [Google Scholar]
[3]. Mosby’s Dental Dictionary 2008 2nd edMosby:250 [Google Scholar]
[4]. Graham GS, Brannon RB, Houston GD, Fibrolipoma of the Gingiva- A Case ReportJ Periodontol 1988 59:118-20. [Google Scholar]
[5]. Hupp JR, Tucker MR, Contemporary oral and maxillofacial surgery 2008 5th edMosby:449-68. [Google Scholar]
[6]. Walters JD, Will JK, Hatfield RD, Cacchillo DA, Raabe DA, Excision and repair of the peripheral ossifying fibroma: a report of 3 casesJ Periodontol 2001 72:939-44. [Google Scholar]
[7]. Thoma DS, Beni GI, Zwahlen M, Hämmerle CH, Jung RE, A systematic review assessing soft tissue augmentation techniquesClin oral implants Res 2009 20:146-65. [Google Scholar]
[8]. Azzi R, Etienne D, Takei H, Fenech P, Surgical thickening of the existing gingiva and reconstruction of interdental papillae around implant-supported restorationsInt J Periodontics Restorative Dent 2002 22:71 [Google Scholar]
[9]. Edel A, Clinical evaluation of free connective tissue grafts used to increase the width of keratinised gingivaJ Clin Periodontol 1974 1:185-96. [Google Scholar]
[10]. Zucchelli G, Mazzotti C, Bentivogli V, Mounssif I, Marzadori M, Monaco C, The connective tissue platform technique for soft tissue augmentationInt J Periodontics Restorative Dent 2012 32:665-75. [Google Scholar]
[11]. Zucchelli M, De Sanctis, Treatment of Multiple Recession –Type defects in patients with esthetic demandsJ Periodontol 2000 71:1506-14. [Google Scholar]
[12]. Hofmanner P, Alessandri R, Laugisch O, Aroca S, Salvi GE, Stavropoulos A, Predictability of surgical techniques used for coverage of multiple adjacent gingival recessions-A systematic reviewQuintessenceint 2012 43:545 [Google Scholar]