Hepatitis B & C Among Farmers – A Seroprevalence Study
Ravinder Garg1, Shaminder Kaur2, Rakesh Aseri3, Simmi Aggarwal4, Jatinder Pal Singh5, Simarpreet Mann6, Sumit Kumar7, Sarabjot Kaur8
1 Associate Professor, Department of Medicine, GGS Medical College & Hospital, Faridkot, Punjab, India.
2 Assistant Professor, Department of Medicine, GGS Medical College & Hospital, Faridkot, Punjab, India.
3 PG Resident, Department of Medicine, GGS Medical College & Hospital, Faridkot, Punjab, India.
4 Professor & Head, Department of Radio- Diagnosis, GGS Medical College & Hospital, Faridkot, Punjab, India.
5 Intern, GGS Medical College & Hospital, Faridkot, Punjab, India.
6 Consultant Physician, Apex hospital, RampuraPhul, Bathinda, India.
7 Senior Resident, Department of Medicine, GGS Medical College & Hospital, Faridkot, Punjab, India.
8 PG Resident, Department of Medicine, GGS Medical College & Hospital, Faridkot, Punjab, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ravinder Garg, Associate Professor, Department of Medicine, GGS Medical College & Hospital, Faridkot, Punjab – 151 203, India. Phone : +91-9988863800, E-mail : drravindergarg@gmail.com
Background: Hepatitis B & C are the two major causes of chronic liver disease, having the similar parenteral route of transmission, thereby responsible for significant morbidity and mortality.
Objective: Agriculture being the backbone of this part of country, the present study was undertaken to assess the seroprevalence of these diseases among the farmers which form the major occupation class in the Malwa belt of Punjab, India.
Materials and Methods: Screening camp was organized at Kisan Mela at the regional station of Punjab Agriculture University at Faridkot, Punjab. Blood samples were collected, and tested for HBsAg and anti-HCV.
Results: Total of 1219 subjects, 63% being in the age group of 30-50 years, were screened of which the seroprevalence of HCV & HBV was 5% and 0.32% respectively, and 72% of HCV positive cases were between 30-50 years of age.
Conclusion: The study stresses on the need of safe injection practices especially in villages and control on addiction, a more effective vaccination program for HBV, strict check on commercial blood banks, and community education regarding tattooing and sexual behaviour.
Farmers, Farmers and hepatitis, Hepatitis prevalence, Hepatitis prevention, Liver disease
Introduction
Since its discovery in 1989, Hepatitis C virus (HCV) has been recognized as a major cause of chronic liver disease worldwide. The most recent WHO estimate of the prevalence of HCV infection is 2%, representing 123 million people [1]. HCV infection has both acute and chronic forms, most of the morbidity associated with infection is realized through the development of chronic liver disease in a subset of infected people years after initial acquisition of the infection. HCV is the leading cause of liver transplantation in developed countries.
Although HCV is endemic worldwide, there is a large degree of geographic variability in its distribution. Countries with the highest reported prevalence rates are located in Africa and Asia; areas with lower prevalence include the industrialised nations in North America, Northern and Western Europe, and Australia. China, whose citizens account for one fifth of the world’s population, has a reported seroprevalence of 3.2% [2]. In India, which holds an additional one-fifth of the world’s population, one community-based survey reported an overall rate of 0.9% [3]. In Pakistan, most reported seropositivity rates range between 2.4% and 6.5% [4]. Egypt, with an estimated population of 73 million, has the highest reported seroprevalence rate of 22% [5].
Hepatitis B virus (HBV) is the other leading cause of acute and chronic liver disease. The average estimated carrier rate of HBV in India is 4%; professional blood donors constitute the major high risk group for HBV infection in India, with a hepatitis B surface antigen positivity rate of 14%.HBV is reported to be responsible for 70% of cases of chronic hepatitis and 80% of cases of cirrhosis of the liver. About 60% of patients with hepatocellular carcinoma are HBV marker positive [6]. Major risk factor for HBV infection transmission among adults is professional blood donors and among children is horizontal spread due to poor hygiene and overcrowded living conditions.
Both HCV and HBV are transmitted primarily through the parenteral route and source of infection include injection, intravenous drug abuse, needle stick accidents and transfusion of blood and especially blood products in patients with hemophilia, solid-organ transplant, chronic renal failure or cancer patients requiring chemotherapy. Professional blood donors constitute nearly 40% of all blood donors in India and represent the major high risk group for HBV infection in this country, with an HBsAg positivity rate of 15% - about five times the prevalence of HBsAg in healthy volunteer blood donors [7].
Since ages the state of Punjab is known for agriculture as its base and farming constitutes the main occupation in the Malwa belt of Punjab. Agriculture being the backbone of this part of country, it is important to study the seroprevalence of these silent killer viruses in this subset of population.
Aims and Objectives
To find out the seroprevalence of Hepatitis B and C in farmers in Malwa belt of Punjab.
Materials and Methods
Screening camp for Hepatitis B & C was organized at the Kisan Mela at the Regional station of Punjab Agriculture University at Faridkot, Punjab, on 10th September 2013 and 4th March 2014. Farmer population gathered at the mela without any prior announcement or advertisement regarding screening for Hepatitis B and C. The subjects were unaware of the screening camp for these diseases. Blood samples were collected; HBsAg and anti-HCV tested by in-vitro immunochromatographic one step assay designed for qualitative determination. A total of 1219 subjects were screened and all were males.
Results
Total 1219 subjects were screened for hepatitis B and C. The age wise break-up of the subjects is as shown in [Table/Fig-1], with maximum number in the age group of 30-39 y (25%), 40-49 y (38%), and 50-59 y (22%). So, 63% were in the age group of 30-50 y and 85% between 30-60 years.
Age wise break-up of the subjects
| Age Group (in years) | No. of Subjects |
|---|
| < 10 | 11 (0.08%) |
| 10-19 | 18 (1.5%) |
| 20-29 | 123 (10%) |
| 30-39 | 306 (25%) |
| 40-49 | 464 (38%) |
| 50-59 | 268 (22%) |
| >60 | 39 (3.2%) |
| Total | 1219 |
Discussion
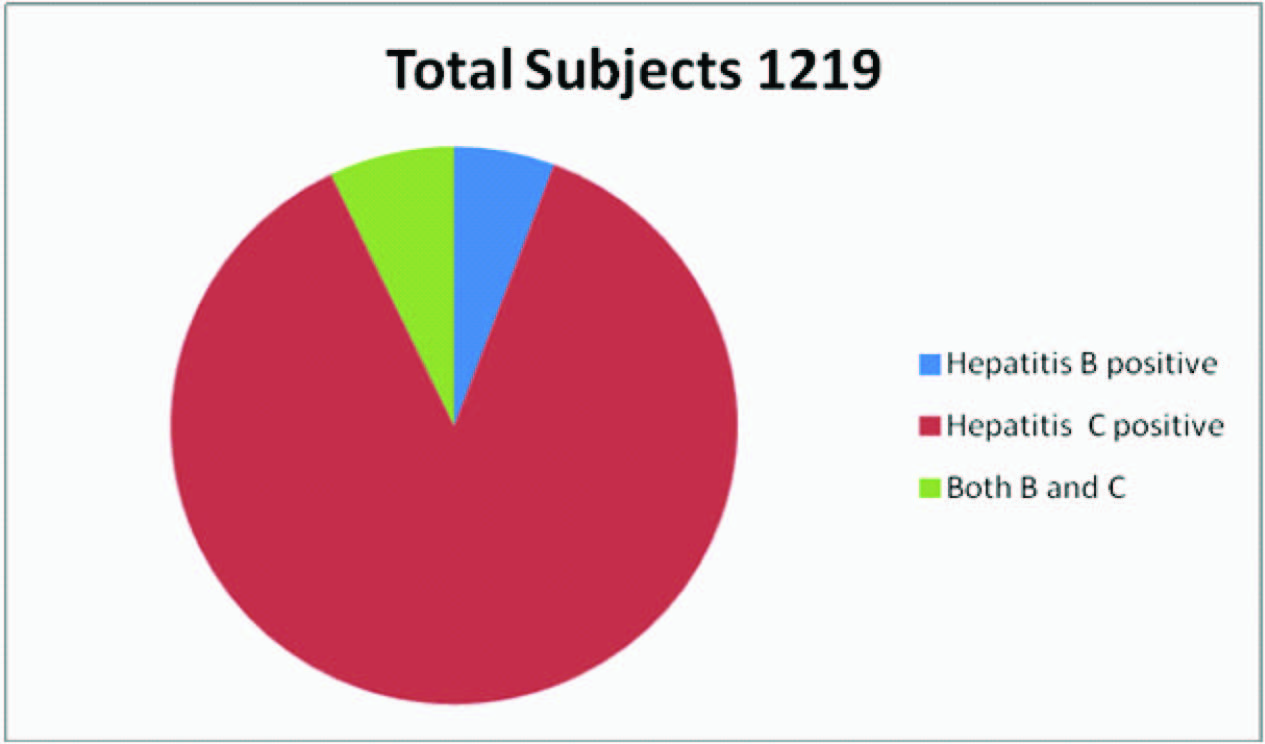
HCV infection is a leading cause of cirrhosis, liver failure and hepatocellular carcinoma. Most chronic hepatitis C patients are asymptomatic and unaware of their liver disease prior to diagnosis. However, chronic hepatitis C patients report a consistent and significant reduction in quality of life, even in the absence of severe liver disease, whether this is because of the uncertainty of living with a chronic illness which has a potential life threatening complications or to other psychosocial factors which are still unclear. The present survey highlights the importance of screening for hepatitis B and C in farmers. 1219 farmers were screened and prevalence of anti HCV seropositivity was found to be 5%, and that of Hepatitis B was 0.32% [Table/Fig-2]. Maximum number of subjects who were found to be HCV positive was in the age group of 40-50 years [Table/Fig-3]. Not much data, pertaining to the seroprevalence of HBV and HCV among this subset of population i.e. farmers, is available till date.
Out of 1219 subjects , 61 (5.0%) subjects were positive for hepatitis C and 4 (0.32%) for hepatitis B; 5 (0.41%) subjects were positive for both hepatitis B & C
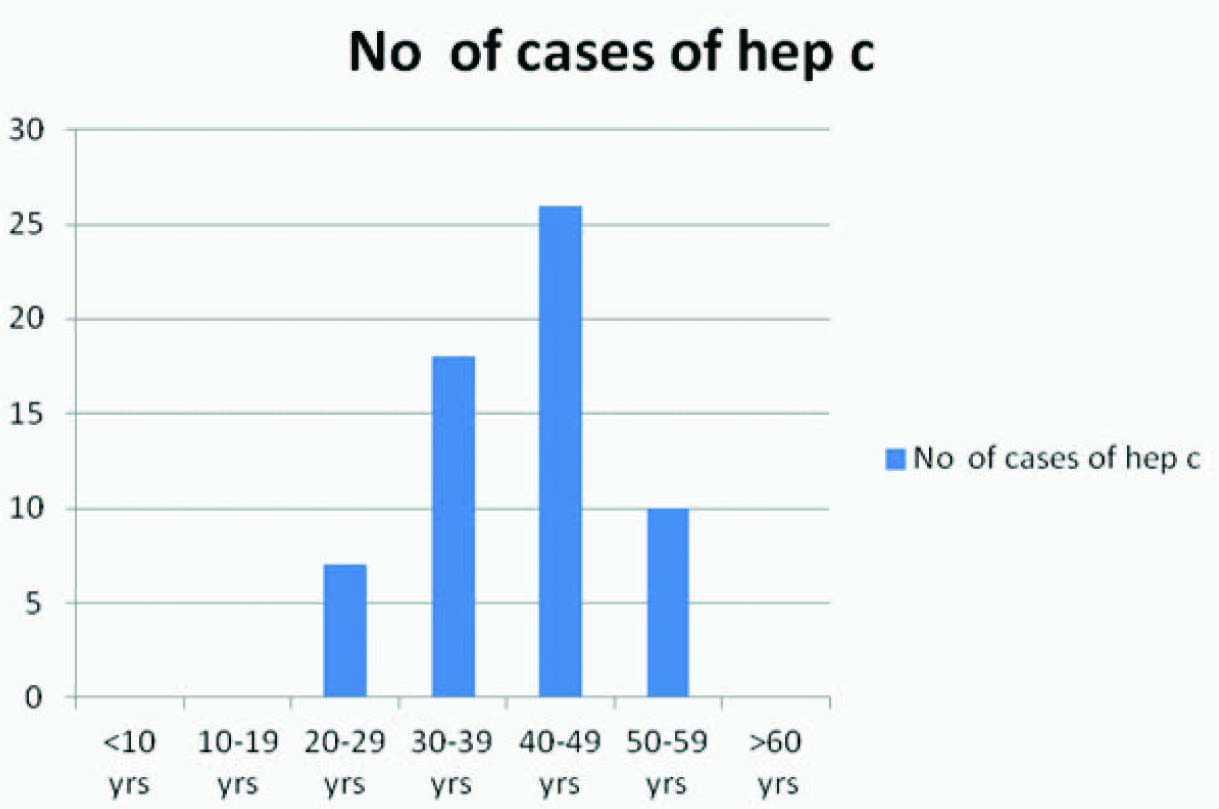
Of the 61 seropositive cases of HCV, 18 (30%) were in the age group of 30-39 years, 26 (42%) of 40-49 years, and 10 (16%) of 50-59 years. So, 44 (72%) seropositive cases were in the age group of 30-50 years
The burden of HCV infection seen in this study is consistent with the data from India and other countries [Table/Fig-4]. Study conducted by Chowdhury et al., showed anti-HCV positivity rate of 5% [8]. Similarly, in the study by Sood et al., in which 5258 subjects were screened, 272 (5.2%) were found to be anti-HCV positive, with highest prevalence in the age group of 41-60 y [9]. These findings are totally in tune with those of the present study indicating a high seroprevalence of HCV in the most dynamic age group of a nation. Thakral et al., showed a positivity of 0.44% among healthy blood donors [10]. Age-wise seroprevalence of HCV was studied by Rajani M and Jais M in 600 subjects at a tertiary care hospital in Delhi where overall 5.5% samples tested positive for anti-HCV [11]. This figure is the same as in the present study but the maximum seropositivity was in 11-20 years age group which is different from our analysis because of the fact that the present study was done at a kisan mela which was not attended by under 20 y years aged subjects.
| Ref no | Author/year | Study | HBV | HCV |
|---|
| [7] | Irshad M et al., 1992 | HBV Status in Professional blood donors. | 0.53-5.1% | - |
| [6] | Tandon et al., 1996 | Hep B carriers in India | 4.0% | - |
| [5] | Frank et al., 2000 | HCV seroprevalence in Egypt | - | 22% |
| [4] | Khattak et al., 2002 | HCV seropositivity in Pakistan | - | 2.4% - 6.5% |
| [8] | Chowdhary et al., 2003 | HCV infection in general population | - | 5% |
| [1] | Perz et al., 2004 | Global HCV Prevalence | - | 2% |
| [10] | Thakral et al., 2006 | Prevalence & significance of HCV seropositivity in blood donors | - | 0.44% |
| [16] | Uppal et al., 2009 | HBV & HCV infection in an urban slum of Northern India | 10.38% | 1.15% |
| [14] | Saravanan et al., 2009 | HBV & HCV infection in chronic liver disease | 44.60% | 26.70% |
| [13] | Supekar Shilpa N & Patel Harshid L 2012 | Prevalence of HBV infection in young students of Anand | 0.694% | - |
| [12] | Shyamala R & Rao J 2012 | Prevalence of HBsAg in a tertiary care hospital | 1.06% | - |
| [9] | Sood et al., 2012 | HCV Prevalence in slected geographical area of North India | 1.3% | 5.2% |
| [17] | Chandra N et al., 2013 | HBV and/or HCV Co-infection in HIV infected patients | 15% | 8.3% |
| [11] | Rajani M & Jais M 2014 | Age-wise seroprevalence of HCV in suspected infectious hepatitis patients | - | 5.5% |
| Present Study | Seroprevalence of HBV & HCV among farmers | 0.32% | 5.0% |
The average estimated carrier rate of hepatitis B virus in India is 4%, with a total pool of approximately 36 million carriers [6]. In the present study a total number of 1219 subjects were screened with a seroprevalence rate of 0.32%. Studies from northern India found HBV sero-prevalence ranging from 0.53 to 5.1% in their blood donors [7]. A study conducted by Sood et al., showed prevelance of 1.3% [9]. Similar study conducted by R Shyamala at Bhaskar Medical College, Ranga Reddy District, India during January 2012 to December 2012, included 1980 patients and all were screened for HBsAg. Out of the total 1980 patients, 21 were found to be positive for HBsAg (1.06%) [12]. Another study was conducted by Shilpa N et al., among 1152 students; 08 cases (0.694 %) were found infected with HBsAg [13]. Overall, these findings point to a very low seropositivity of HBV vis a vis HCV although the routes of transmission are the same, thereby highlighting the unavailability of HCV vaccine as the major hurdle. Co infection with HCV and HBV was observed in 15 (5.9%) patients of chronic liver disease out of total of 251 in the study by Saravanan et al., [14]. But this high prevalence was observed because the subjects in the study were the patients of chronic liver disease & not normal subjects and moreover anti-HBC, HBV- DNA and HCV-RNA were also tested in addition to anti-HCV & HBsAg vis a vis the present study where only the normal subjects have been tested for anti-HCV and HBsAg.
Tattooing is a common practice especially in the younger age group and although not much data on tattooing amongst farmers is available, but a study on the general population in Germany revealed a prevalence of tattooing and body piercing to be 8.5% and 6.5% respectively with highest incidence between 14 to 24 years. This study also highlighted that tattooing is significantly correlated with the perception of reduced mental health and both tattooing and body piercing are correlated with significantly increased sensation seeking behavior [15].
Primary prevention of HCV should focus on availability of safe blood and blood products, safe injection practices and control on addictions. Secondary preventive efforts should stress on early medical evaluation and anti-viral treatment of HCV infected subjects with efforts that treatment facilities are easily accessible to the community. Moreover, HCV infected subjects should be counselled for minimizing the transmission to others.
Hepatitis B is a major public health problem in India and will continue to be until appropriate nationwide vaccination programmes and other control measures are applied effectively, and a proper constraint is maintained on the commercial blood banks. The discrepancy between demand and supply calls for encouragement of voluntary blood donation. Furthermore, although programs for the prevention and control of hepatitis B should represent a priority for the government and health services in India, the costs and difficulties associated with their initiation are a major problem at present.
Conclusion
The high seroprevalence of HCV to the tune of 5% among farmers in their most energetic age group highlights the handicap of vaccine and post exposure prophylaxis thereby stressing the need for safer blood supply, safe injection practices especially in villages and control on addiction. While the search for an effective and affordable therapy and vaccine continues, preventive strategies remain the foremost task of public health authorities. Also, the study calls for a more effective HBV vaccination program, a check on the commercial blood banks, and community education regarding tattooing and sexual behaviour.
[1]. Perz JF, Farrington LA, Pecoraro C, Hutin YJF, Armstrong GL, Estimated global prevalence of hepatitis C virus infection42nd Annual Meeting of the Infectious Diseases Society of America 2004, 30-Oct 3 Boston, MA, USA [Google Scholar]
[2]. Xia GL, Liu CB, Cao HL, Prevalence of hepatitis B and C virus infections in the general Chinese population: results from a nationwide cross-sectional seroepidemiologic study of hepatitis A, B, C, D, and E virus infections in China, 1992International Hepatology Communications 1996 5:62-73. [Google Scholar]
[3]. Chowdhury A, Santra A, Chaudhuri S, Hepatitis C virus infection in the general population: a community-based study in West Bengal, IndiaHepatology 2003 37:802-09. [Google Scholar]
[4]. Khattak MF, Salamat N, Bhatti FA, Qureshi TZ, Seroprevalence of hepatitis B, C and HIV in blood donors in northern PakistanJ Pak Med Assoc 2002 52:398-402. [Google Scholar]
[5]. Frank C, Mohamed MK, Strickland GT, The role of parenteral antischistosomal therapy in the spread of hepatitis C virus in EgyptLancet 2000 355:887 [Google Scholar]
[6]. Tandon BN, Acharya SK, Tandon A, Epidemiology of hepatitis B virus infection in IndiaGut 1996 38(suppl2):S56-59. [Google Scholar]
[7]. Irshad M, Singh YN, Acharya SK, HBV-status in professional blood donors in North IndiaTrop Gastroenterol 1992 13:112-14. [Google Scholar]
[8]. Chowdhury A, Santra A, Chaudhuri S, Dhali GK, Maity SG, Naik TN, Hepatitis C virus infection in the general population: A community-based study in West Bengal, IndiaHepatology 2003 37:802 [Google Scholar]
[9]. Sood A, Sarin SK, Midha V, Hissar S, Sood N, Bansal P, Bansal M, Prevalence of hepatitis C virus in a selected geographical area of Northen India: A population based surveyIndian J Gastroenterol 2012 31(5):232-36. [Google Scholar]
[10]. Thakral B, Marwaha N, Chawla YK, Saluja K, Sharma A, Sharma RR, Prevalence & significance of hepatitis C virus (HCV) seropositivity in blood donorsIndian J Med Res 2006 124:431-38. [Google Scholar]
[11]. Rajani M, Jais M, Age-wise seroprevalence of hepatitis C virus infection in clinically suspected infectious hepatitis patients attending a tertiary care hospital in DelhiInternational Journal of Medicine and Public Health 2014 4(1.78):81 [Google Scholar]
[12]. Shyamala R, Rao J, The study of prevalence of hepatitis B surface antigen in a tertiary care hospital in South IndiaDer Pharmacia Lettre 2013 5(1):11-12. [Google Scholar]
[13]. Supekar S, Patel H, Prevalence of Hepatitis B Virus Infection In Young Students of AnandNational Journal of Medical Research 2012 2(3):299 [Google Scholar]
[14]. Saravanan S, Velu V, Nandakumar S, Madhavan V, Shanmugasundaram U, Murugavel KG, Hepatitis B virus and hepatitis C virus dual infection among patients with chronic liver diseaseJ Microbiol Immunol Infect 2009 42(2):122-28. [Google Scholar]
[15]. Aglaja S, Andreas H, Elmar B, Prevalence of tattooing and body piercing in Germany and perception of health, mental disorders and sensation seeking among tattooed and body pierced individualsJ of Psychosomatic Research 2006 60(5):531-34. [Google Scholar]
[16]. Uppal Y, Garg S, Malhotra S, Singh MM, Gupta VK, Mishra B, Singh SV, Hepatitis B and C virus infection in an urban slum of Northern IndiaJ Commun Dis 2009 41(3):201-04. [Google Scholar]
[17]. Chandra N, Joshi N, Raju YSN, Kumar A, Teja VD, Hepatitis B and/or C co-infection in HIV infected patients:A study in a tertiary care centre from south IndiaIndian J Med Res 2013 138:950-54. [Google Scholar]