Introduction
MRI is the established gold standard for imaging of acute spinal trauma. It can accurately depict intrinsic changes in the spinal cord i.e. cord haemorrhage and cord oedema as well as extrinsic compression of cord by herniated disc, epidural hematoma or bony fragments.Prognostic value of various qualitative factors like cord oedema, haemorrhage, disc herniations, ligamentous injury and extradural hematomas has been described previously [1-6]. In acute setting, MRI is important for defining the extent of soft tissue and bony injury and associated ligamentous and disc injuries and for defining the extent of epidural hematomas and extent of cord compression. These factors are important for planning of surgical/non-surgical treatment and for prognostic quantification [3]. Various quantitative parameters have also been described to look for quantifiable variables of spinal injury which can be measured objectively like lesion length, maximum canal compromise (MCC) and maximum spinal cord compression (MSCC) [4,6,7]. There is scanty literature on prognostic value of these quantitative variables as predictors of neurological recovery on follow up [4]. Particularly, there is very little literature regarding the same in developing countries like India. Therefore the present study was aimed to study qualitative and quantitative variables in patients with acute spinal trauma and study the factors predictive of outcome on follow up.
Materials and Methods
The present study was conducted on 50 indoor patients presenting with suspected acute cervical or dorsal spinal trauma from January 2009 to April 2010 which were available for follow up. Study was approved by the university. Patients who have any contraindication to MRI were excluded. Unconscious patients and those with concomitant head injury were also excluded in which neurological deficit can not be accurately assessed. All patients were assessed for neurological deficit using ASIA grading system [5,6] as follows:
A. No motor or sensory function is preserved in sacral segments S4-S5
B. Sensory, but not motor function is preserved below the neurologic level and includes sacral segments S4-S5
C. Motor function is preserved below the neurologic level, and more than half of key muscles below the neurologic level have muscle grade < 3
D. Motor function is preserved below the neurologic level, and atleast half of key muscles below the neurologic level have muscle grade ≥ 3
E. Motor and sensory functions are normal.
ASIA grade A defined complete spinal cord injury (SCI). ASIA grades B, C and D defined incomplete SCI. ASIA grade E represented spinal trauma without spinal cord injury.
Preparation of the patient
Articles such as jewellery, keys, credit cards, watches, coins, and other metallic objects were placed in the locker provided. Before starting the MR study, the procedure was explained to the patient in his/her vernacular language to allay the fear and the anxiety and written informed consent was taken. Length of the study in magnet was communicated to the patient which may vary from 30min to 45 min. During the entire period of procedure patient was in contact with technologist/ doctor by a two way intercom system.
MRI protocol
All examinations were performed on a 18 channel 1.5 Tesla MRI scanner (Magnetom Avanto, Siemens Medical Systems, Erlangen, Germany). Localizer was taken in axial and sagittal planes after making proper positioning of the patient. The MRI protocol consisted of sagittalT1W, sagittal T2W, Sagittal STIR, axial T1W, axial T2W sequences. Additional T2*GRE (TE 25, TR 810) with flip angle of 28 degrees were obtained wherever required.
MRI evaluation [Table/Fig-1a,1b,Table/Fig-2,3a,3b]
Based on the MRI findings, patients were divided into six patterns as described by Ramon et al., [3]
Pattern zero: Normal findings on MRI
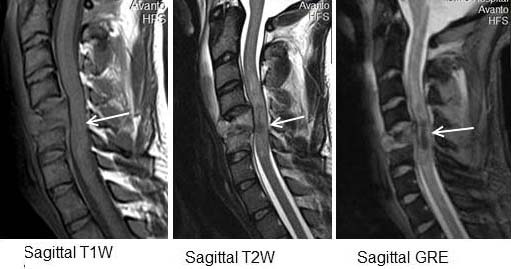
Pattern I: Haemorrhage (hypointense on T2W with thin rim of hyperintensity) [Table/Fig-1a].
Pattern II: Oedema (hyperintense on T2W images) [Table/Fig-2].
Pattern III: Contusion (mixed central signal on T2W with peripheral hyperintensity) [Table/Fig-3a].
Pattern IV: Compression (severe obliteration of the spinal cord, with significant alteration of its morphology preventingdetection of signal alterations such as bleeding) [Table/Fig-4].
Pattern V: Transection pattern: sagittal discontinuity of spinal cord [Table/Fig-5].
Nine qualitative variables (vertebral fracture/subluxation, facetal subluxation/dislocation, cord oedema, haemorrhage/contusion, cord compression,epidural haemorrhage, traumatic disc herniation, ligamentous injuryand pre/paravertebral collection) were assessed for correlation with severity of spinal injury using ASIA score.
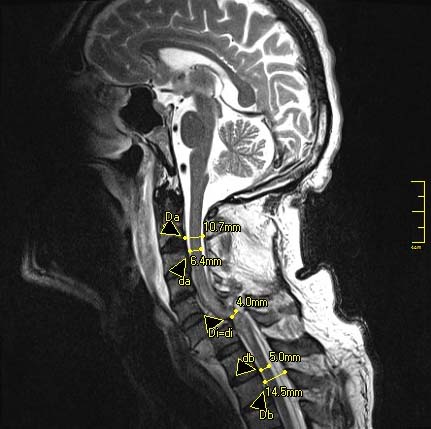
Three quantitative parameters were measured: Maximum (bony) canal compromise (MCC), maximum spinal cord compression (MSCC) and lesion length.MCC was measured on mid sagittal T2W images by measuring canal diameter at the level of injury and by taking average of diameters at normal levels above and below it. Similarly MSCC were measured on mid sagittal T2W images by measuring cord diameter at the level of injury and by taking average diameters at normal level above and below the level of injury as described previously in literature [5-7]. Lesion length was measured on sagittal T2W images as maximum cranio-caudal dimension of signal abnormality [Table/Fig-1band3b] .
Patients’ ASIA score was assessed again at 2 weeks/at the time of discharge (whichever was earlier) and at 3-6 months follow up period.
MRI findings and patterns were correlated with patients’ neurological status at the time of examination and at final follow up to look for predictors of neurological deficit.
Results
There were a total of 50 subjects in the age group of 11–90 years with a mean age of 43 years. Majority of subjects belonged to the young age group with maximum of 13(26%) subjects in the age group of 21-30 years with predominance of male subjects (86%)with male: female ratio of 6.1:1.The most common cause of spinal trauma among the subjects was road traffic accidents accounting for 62% of the cases. Next most common cause was fall from height (34%) while 4% of injuries were due to work related activities.Cervical spine was the most common site of injury, accounting for 70% of all the subjects.
Using ASIA score, the most common pattern was incomplete spinal cord injury (seen in 50% of the subjects). Second most common pattern was complete spinal cord injury (seen in 34% of the subjects), while the least common pattern was spinal trauma without spinal cord injury (seen in 16% of the subjects).
The most commonly observed MRI pattern was pattern II (oedema) seen in 26% of the subjects. Pattern III (contusion) was observed in 24% of subjects and Pattern I (haemorrhage) was observed in 16% of the subjects. Pattern IV (6%) and pattern V (4%) were least commonly observed [Table/Fig-6].
Normal baseline MRI (pattern 0) was seen in 12 subjects and was associated with no neurological deficit in 8 subjects (ASIA grade E) and incomplete SCI in 4 subjects (ASIA grade D) followed by complete recovery in all patients on follow-up examination. Pattern I (haemorrhage) was associated with complete spinal cord injury (ASIA grade A) in all 8 patients. Six of them expired on follow-up and rest did not show any recovery of follow-up. Pattern II (oedema) was associated with complete SCI in one patient and incomplete SCI in 12 subjects. On follow, there was complete recovery in 7 subjects and other 6 subjects showed good functional recovery (ASIA grade C and D).Pattern III (contusion) was associated with complete SCI in three subjects and incomplete SCI in 9 subjects. One subject expired on follow-up. Others shows incomplete recovery with only one subject progressing to complete recovery (ASIA grade E). Compression and transection patterns were associated with complete neurological deficit at presentation and increased mortality at subsequent follow-up[Table/Fig-6,7,8].
When comparing qualitative variables among patients with complete and incomplete SCI, haemorrhage/ contusion (p-value <0.0001), pre/paravertebral collection (p-value =0.001), facetal subluxation/dislocation (p-value = 0.007), vertebral fracture/subluxation (p value =0.026), epidural haemorrhage (p-value=0.019) and ligamentous injury (p-value=0.026) were more commonly seen among patients with complete SCI. No significant correlation was observed between the two groups with presence or absence of cord oedema, cord compression and traumatic disc herniation [Table/Fig-9]. Using one way ANOVA, all qualitative variables were tested for significance of difference in all subjects with severity of injury by dividingsubjects into three groups: those with complete SCI, those with incomplete SCI and thosewith spinal trauma without SCI. Significant correlation was observed with all qualitative variables except with vertebral fracture/subluxation
We calculated three quantitative variables in our study: Lesion length, mean canal compromise (MCC), mean spinal cord compression (MSCC). All the three quantitative parameters (lesion length, MCC and MSCC) were significantly increased in patients with complete SCI as compared to those with incomplete SCI [Table/Fig-10]. Using Fisher exact test, we compared the significance of difference of these variables among subjects with complete SCI and in those with incomplete SCI. Mean lesion length was significantly more in patients with complete SCI as compared to those with incomplete SCI (67.8mm vs 34mm, p-value <0.0001). Mean value of MCC and MSCC was significantly more in patients with complete SCI as compared to those with incomplete SCI (p-value <0.0001). Using multiple regression, we analysed three quantitative parameters (lesion length, MCC and MSCC) and nine qualitative parameters (vertebral fracture/subluxation, facetal subluxation/dislocation, cord oedema, haemorrhage/contusion, cord compression, epidural haemorrhage, traumatic disc herniation, ligamentous injury and pre/paravertebral collection) to determine the potential predictors of baseline ASIA score (at the time of MR study) and at the time of final follow up. The best predictors for baseline ASIA score were MCC, cord oedema and cord haemorrhage. For the final ASIA score, the best predictors were baseline ASIA score and cord haemorrhage. Lesion length was also a predictor factor, however it did not reach statistical significance (p-value = 0.07) [Table/Fig-11].
Discussion
Spinal trauma is a major health problem in both the developed and the developing countries. It causes an enormous economic burden because a large number of affected patients are relatively young. In the present study, majority of the affected patients belonged to the age group of 20-30 years (26%) while the mean age was 43 years. The majority of the affected patients were males (86%, with male to female ratio of 6.1:1) which is similar to findings in other studies. [3,4,8] The relative predominance of young male patients is due to increased mobility, work related injuries and road traffic accidents
The most common cause of spinal trauma in present study was road traffic accidents (62%) followed by fall from height (34%) while 4% of injuries were due to work related activities. Other studies [3,8,9] have also reported a similar trend. India is a developing country with increasing vehicular traffic and poorly maintained roads, especially in rural areas. Most people are not fully aware of traffic rules, roads are not well maintained and traffic regulation is often poor. These factors account for large number of motor vehicle accidents. In elderly, even minor falls can result in significant spinal trauma due to underlying osteoporotic and degenerative spine disease.
The most common site of injury in the spine was cervical spine, accounting for 70% of the cases. Increased mobility in cervical region combined with reduced vertebral and musculo-ligamentous support makes it more prone to injury.
Among qualitative parameters,when comparing patients with complete and incomplete SCI, haemorrhage/ contusion pre/paravertebral collection, and facetal subluxation/dislocation, vertebral fracture/subluxation, epidural haemorrhage and ligamentous injury were significantly more common in patients with complete SCI. No significant correlation was observed between the two groups with presence or absence of cord oedema, cord compression and traumatic disc herniation. Overall, presence of cord haemorrhage/contusion was the most significant qualitative factor for indicating the severity of spinal cord injury using ASIA scoring system. Miyanji et al., [4] also observed significant correlation between severity of SCI and presence or absence of cord haemorrhage, cord oedema, cord swelling and soft tissue injury. They observed no significant correlation with presence or absence of canal stenosis or disc herniation. Overall the presence of cord haemorrhage is most important qualitative marker for indicating the severity of cord injury.
We calculated three quantitative variables in our study: Lesion length, mean canal compromise (MCC), mean spinal cord compression (MSCC). Using Fisher exact test, we compared the significance of difference of these variables among subjects with complete SCI and in those with incomplete SCI. Mean lesion length was significantly more in patients with complete SCI as compared to those with incomplete SCI (67.8mm vs 23mm, p-value <0.0001). Mean value of MCC and MSCC was significantly more in patients with complete SCI as compared to those with incomplete SCI (p-value <0.0001). These findings are similar to Miyanji et al., [4].
Normal pattern (type 0) ruled out complete spinal injury. Also in those with deficit, it predicted good prognosis for neurological recovery on subsequent follow up.Type I pattern (haemorrhage)in present study was associated with complete SCI with no recovery on follow up. These findings are similar to those of Ramón et al.,[3]and Kulkarni et al., [10] that type I pattern indicates irreversible cord injury and no recovery on subsequent follow-up. Gross haemorrhage visible at MR imaging is indicative of complete damage at cellular level and confers pooly outcome. Type II pattern (oedema) was associated with incomplete SCI. These findings are similar to other studies [3,10]. Cord oedema indicates incomplete type of spinal cord injury as the damage at cellular level is reversible to some extent. Many of these patients initially show evidence of neurological deficit, however on subsequent follow up, there is good chance of neurological recovery and usually favourable outcome.Type III pattern (contusion) indicates spinal cord injury intermediate between pattern I and II. These patients showed intermediate severity of spinal injury and more often associated with incomplete neurological recovery on subsequent follow-up.Type IV pattern (Compression pattern) was associated with complete spinal cord injury at the time of presentation. Two of them expired on subsequent follow-up. The only surviving subject made incomplete recovery (ASIA grade C) on final follow-up.Type V pattern (Transection pattern) was associated with complete SCI These results are expected because this pattern involves physical transection of the cord, therefore it represents complete injury and any hope for recovery is remote.
When analysing all quantitative and quantitative parameters to determine the potential predictors of baseline ASIA score (at the time of MR study) and at the time of final follow up, the best predictors for baseline ASIA score were MCC, cord oedema and cord haemorrhage. For the final ASIA score, the best predictors were baseline ASIA score and cord haemorrhage. Lesion length was also a predictor factor, however it did not reach statistical significance (p-value = 0.07) [Table/Fig-11] Miyanji et al., [4] in their study, observed that baseline ASIA score was best predicted by MCC, MSCC and cord oedema. In another study, Selden et al., [11] compared MR findings with neurological status using Frankel grading system [12]. They observed that baseline neurological status correlated with cord oedema and haemorrhage. Thus results of the present study are similar to the past studies. In the study by Miyanji et al., [4] the best predictors for final ASIA score were baseline ASIA score, cord haemorrhage and cord swelling. In the study of Selden et al., [11] baseline Frankel score, cord oedema, haemorrhage and lesion length were predictive factors of final neurological outcome. So the results of present study are similar to the previous observations.
Qualitative factors like MCC and MSCC although may correlate with baseline neurological status, they are not useful for predicting the long term prognosis as observed in past studies and again confirmed in present study. This is likely due to the fact that MCC and MSCC reflect acute neurological deficit that arises due to cord compression. It does not reflect permanent damage and there is potential for recovery. This is further supported by the fact that even patients with most severe compression pattern of injury showed incomplete recovery on follow-up in our study. Similar observations were made by Ramón et al., [3]. Similarly cord oedema was predictor for baseline score but not for the final outcome because oedema also reflects that injury may be reversible and indicates potential for recovery.
Final ASIA score is related to the baseline ASIA score. It has been observed in earlier studies and again confirmed in present study. When using multiple regression analysis for comparing all qualitative and quantitative parameters, only other significant predictor in our study was cord haemorrhage. Cord haemorrhage has been recognised as an important predictor for both baseline neurological status as well as subsequent potential for recovery. Haemorrhage indicates complete SCI and reflects poor outcome. This has been confirmed in the past studies as well as the present study. Apart from the baseline ASIA score; this was the only predictor for long term prognosis in our study.
Sagittal T1W, T2W and GRE images showing type I pattern (haemorrhage) showing blooming on GRE. Also seen is burst fracture of C5 vertebra with posterior retropuslion of the cortex with bony contusions in C6 vertebra. Small anterior epidural collection is seen at these levels. Anterior and posterior longitudinal ligaments are disrupted at this level. There is large pre/paravertebral T2W hyperintense collection from C1 to C6 levels,
Showing calculation of lesion length by measuring cranio-caudal dimension of T2W signal abnormality (measuring 61.9mm in this case)

Sagittal T2W and STIR images showing type II pattern (oedema). Also seen is burst fracture of D12 vertebra with posterior retropulsion of its cortex and marrow oedema in D11 vertebra.Small pre/paravertebral collection is also seen at this level. Anterior longitudinal ligament is disrupted. Posterior longitudinal ligament is stretched but intact

Sagittal T1W, T2W and GRE images showing type III pattern (contusion) showing cord oedema with tiny foci of blooming on GRE.There is marked anterior dislocation of C6 over C7 vertebra with bilateral facetal dislocation (not shown) with focal disruption of anterior and posterior longitudinal ligaments and ligamentumflavum. Anterior epidural and pre/paravertebral collection is also seen.,

Showing calculation of MCC and MSCC. MCC= [1- Di/{1/2(Da+Db)}] x 100 = 68.25 and MSCC[1- di/{1/2(da+db)}] x 100=29.8, [
Sagittal T1 and T2W showing type IV pattern (compression) with marked anterior dislocation at C6-7 level with focal ligamentous disruption with altered signal in the spinal cord above and below this level. Small anterior epidural and pre/paravertebral collection is also seen.,

Sagittal T1 and T2W showing type V pattern (transection) with complete anterior dislocation of C4 over C5 vertebra. Again seen is focal ligamentous disruption with altered signal in the spinal cord above and below this level. Small anterior epidural and pre/paravertebral collection is also seen

Showing distribution of the subjects according to MRI pattern and ASIA grading at initial presentation
| MRI pattern | Total no (%age) | ASIA grade A | ASIA grade B | ASIA grade C | ASIA grade D | ASIA grade E |
| 0 | 12 (24%) | 0 | 0 | 0 | 4 | 8 |
| I | 8 (16%) | 8 | 0 | 0 | 0 | 0 |
| II | 13 (26%) | 1 | 2 | 7 | 3 | 0 |
| III | 12 (24%) | 3 | 6 | 2 | 1 | 0 |
| IV | 3 (6%) | 3 | 0 | 0 | 0 | 0 |
| V | 2 (4%) | 2 | 0 | 0 | 0 | 0 |
Showing distribution of the subjects according to MRI pattern and ASIA grading at 2 weeks/discharge
| MRI pattern | ASIA grade A | ASIA grade B | ASIA grade C | ASIA grade D | ASIA grade E |
| 0 | 0 | 0 | 0 | 0 | 12 |
| I | 4 | 0 | 0 | 0 | 0 |
| II | 0 | 1 | 7 | 5 | 0 |
| III | 1 | 7 | 2 | 1 | 0 |
| IV | 3 | 0 | 0 | 0 | 0 |
| V | 1 | 0 | 0 | 0 | 0 |
Showing distribution of the subjects according to MRI pattern and ASIA grading at follow up (3-6 months)
| MRI pattern | ASIA grade A | ASIA grade B | ASIA grade C | ASIA grade D | ASIA grade E |
| 0 | 0 | 0 | 0 | 0 | 12 |
| I | 2 | 0 | 0 | 0 | 0 |
| II | 0 | 0 | 1 | 5 | 7 |
| III | 0 | 2 | 6 | 2 | 1 |
| IV | 0 | 0 | 1 | 0 | 0 |
| V | 1 | 0 | 0 | 0 | 0 |
Showing comparative distribution of qualitative variables in patients with complete and incomplete SCI
| Complete SCI | Incomplete SCI | p-value |
| Total no. of patients | 17 | 25 | |
| Vertebral fracture/subluxation | 15 | 13 | 0.026 (S) |
| Facetal subluxation/dislocation | 8 | 2 | 0.0076 (HS) |
| Cord oedema | 17 | 21 | 0.1343 (NS) |
| Haemorrhage/Hemorrhagic contusion | 16 | 9 | <0.0001 (HS) |
| Cord compression | 14 | 20 | 1 (NS) |
| Epidural haemorrhage | 7 | 2 | 0.019 (S) |
| Traumatic Disc herniation | 4 | 3 | 0.39 (NS) |
| Ligamentous injury | 12 | 8 | 0.026 (S) |
| Pre/paravertebral collection | 14 | 8 | 0.0018 (HS) |
Showing Mean±SD of MCC, MSCC and lesion length in patients with complete SCI, incomplete SCI and in those with spinal trauma without SCI
| ASIA Grading |
| Complete SCI | Incomplete SCI | Spiral trauma without SSI |
| Total no. Of patients | 17 | 25 | 8 |
| MCC | 61.70±20.71 | 29.52±17.06 | 5.0±10.69 |
| MSCC | 51±27.5 | 19.52±14.41 | 0 |
| Lesion length (in cm) | 6.78±2.23 | 3.41±2.09 | 0 |
Showing multiple linear regression analysis results for testing of qualitative and quantiative variables as predictors of baseline ASIA score and ASIA score at final follow up
| R2 value, p value | Dependent variable | Independent variable | p-value |
| Model 1 | 0.85, <0.001 | Baseline ASIA score | MCC | 0.04 |
| Cord oedema | <0.001 |
| Cord haemorrhage | <0.001 |
| Model 2 | 0.897, <0.001 | Final ASIA score | Baseline ASIA score | 0.03 |
| Cord haemorrhage | <0.001 |
| Lesion length | 0.07 |
Conclusion
So to conclude, presence of cord oedema, cord haemorrhage and MCC best correlate with neurological deficit at presentation. While poor baseline ASIA score and cord haemorrhage confers a poor long term outcome. On the other hand, absence of cord haemorrhage usually indicates some potential for neurological recovery.
[1]. AE Flanders, DM Schaefer, HT Doan, MM Mishkin, CF Gonzalez, BE Northrup, Acute cervical spine trauma: correlation of MR imaging findings with degree of neurologic deficitRadiology 1990 177(1):25-33. [Google Scholar]
[2]. K Shimada, T Tokioka, Sequential MR studies of cervical cord injury: correlation withneurological damage and clinical outcomeSpinal Cord 1999 37(6):410-15. [Google Scholar]
[3]. Ramon S, Dominguez R, Raamirez L, Paraira M, Olona M, Castello T, Garcia Fernandez L, Clinical and magnetic resonance imaging correlation in acute spinal cord injurySpinal Cord 1997 35:664-73. [Google Scholar]
[4]. F Miyanji, JC Furlan, B Aarabi, PM Arnold, MG Fehlings, Acute cervical traumatic spinal cord injury: MR imaging findings correlated with neurologic outcome prospective study with 100 consecutive patientsRadiology 2007 243(3):820-27. [Google Scholar]
[5]. FM Maynard JR, MB Bracken , G Creasey, International Standards for Neurological and Functional Classification of Spinal Cord Injury. American Spinal Injury AssociationSpinal Cord 1997 35(5):266-74. [Google Scholar]
[6]. MG Fehlings, SC Rao, CH Tator, G Skaf, P Arnold, E Benzel, The optimal radiologic method for assessing spinal canal compromise and cord compression in patients with cervical spinal cord injury. Part II: Results of a multicenter studySpine (Phila Pa 1976) 1999 24(6):605-13. [Google Scholar]
[7]. KC Song, JW You, HH Kim, HM Sohn, Neurologic and Functional Outcomes after Traumatic Central Cord SyndromeJ Korean Orthop Assoc 2014 49:50-57. [Google Scholar]
[8]. LH Sekhon, MG Fehlings, Epidemiology, demographics, and pathophysiology of acute spinal cord injurySpine (Phila Pa 1976) 2001 15(24 Suppl):S2-12. [Google Scholar]
[9]. MD D’Alise, EC Benzel, BL Hart, Magnetic resonance imaging evaluation of the cervical spine in the comatose or obtunded trauma patientJ Neurosurg 1999 91(1 Suppl):54-59. [Google Scholar]
[10]. MV Kulkarni, CB McArdle, D Kopanicky, Acute spinal cord injury: MR imaging at 1.5 TRadiology 1987 164(3):837-43. [Google Scholar]
[11]. NR Selden, DJ Quint, N Patel, HS d’Arcy, SM Papadopoulos, Emergency magnetic resonance imaging of cervical spinal cord injuries: clinical correlation and prognosisNeurosurgery 1999 44(4):785-93. [Google Scholar]
[12]. HL Frankel, DO Hancock, G Hyslop, The value of postural reduction in the initial management of closed injuries of the spine with paraplegia and tetraplegiaParaplegia 1969 7(3):179-92. [Google Scholar]