Images in Medicine: Giant Cell Tumour of the Talus in a 7-Year-old Boy
Ravishankar Pillenahalli Maheshwarappa1, Amit Gupta2, Juhi Bansal3, Mangi Lal Meena4, Narendra Kardam5
1 Assistant Professor, Department of Radiodiagnosis, Adichunchanagiri Institute of Medical Sciences, Bellur, Karnataka, India.
2 Fellow in Neuroradiology, Department of Neuroradiology, University Hospitals Case Medical Center, Cleveland, Ohio.
3 Senior Resident, Department of Radio-diagnosis, Sawai Mann Singh Medical College, Jaipur, India.
4 Professor and Head, Department of Radiodiagnosis, Ravindra Nath Tagore Medical College, Udaipur, India.
5 Professor, Department of Radiodiagnosis, Ravindra Nath Tagore Medical College, Udaipur, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ravishankar Pillenahalli Maheshwarappa, Room No. 24, Kalpataru Bhavan, Adichunchanagiri Institute of Medical Sciences, Bellur, Nagamangala taluk, Mandya-571-401, Karnataka, India. Phone : +917665166933, E-mail : ravi_spm@yahoo.co.in
Gaint cell tumour, talus, young age
Introduction
Giant cell tumours (GCT) are locally aggressive lesions that primarily affect the epiphyses of long bones. They typically present in the third to fourth decades of life and are rare under 20 years of age. Involvement of the foot is uncommon, frequently affecting the calcaneus and metatarsals, rarely the talus. We report a case of GCT of the talus in a 7 year old boy which was diagnosed by imaging and confirmed by histopathological analysis.
Case Report
A 7-year-old boy came with progressively increasing pain and swelling in the right ankle joint of several months duration. A radiograph of the ankle joint showed an expansile lytic lesion of the right talus. The contrast CT scan showed an expansile lesion with enhancing soft tissue at the periphery. There was significant thinning of the cortex. No intra articular extension was seen [Table/Fig-1,2a,b]. However no other lesions were found elsewhere in the skeleton. The diagnosis of gaint cell tumour was given which was later confirmed by histopathological analysis [Table/Fig-3]. Partial resection of the talus with bone grafting was done. The patient was followed up for two years. No recurrence was found.
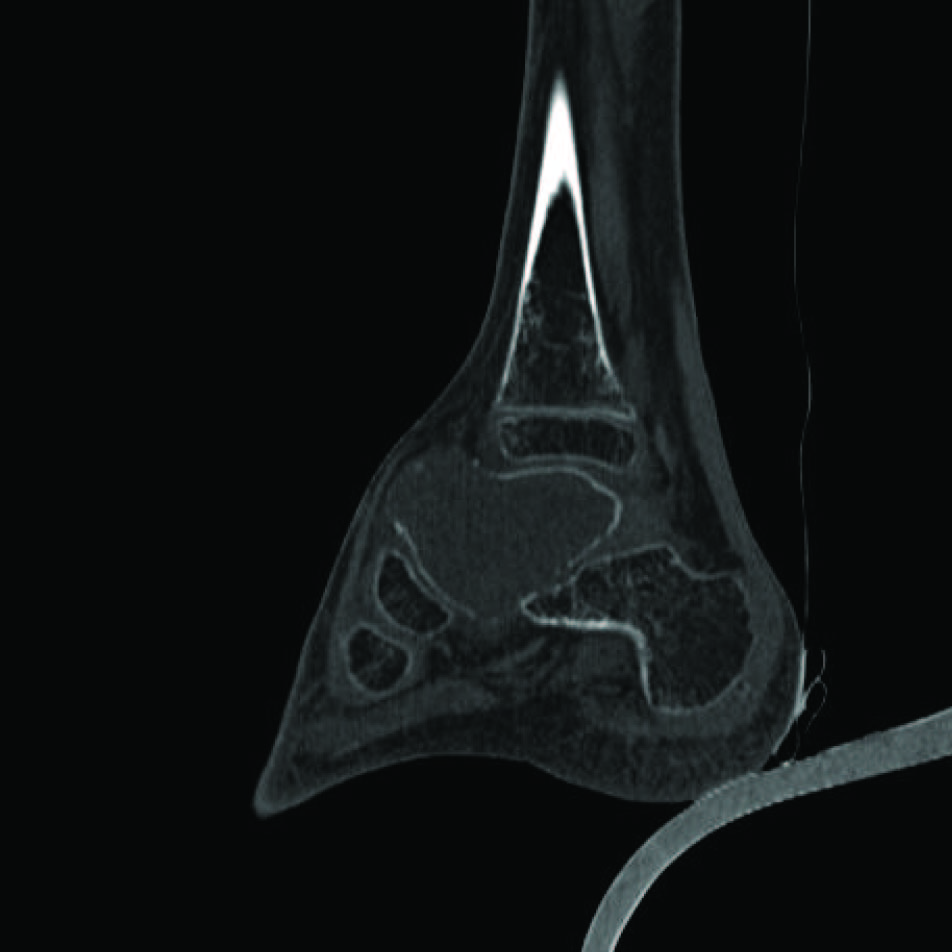
Sagittal non contrast CT of the ankle joint (bone window) showing a osteolytic lesion involving the talus showing cortical thinning. Lesion is seen minimally extending beyond the confines of the corte
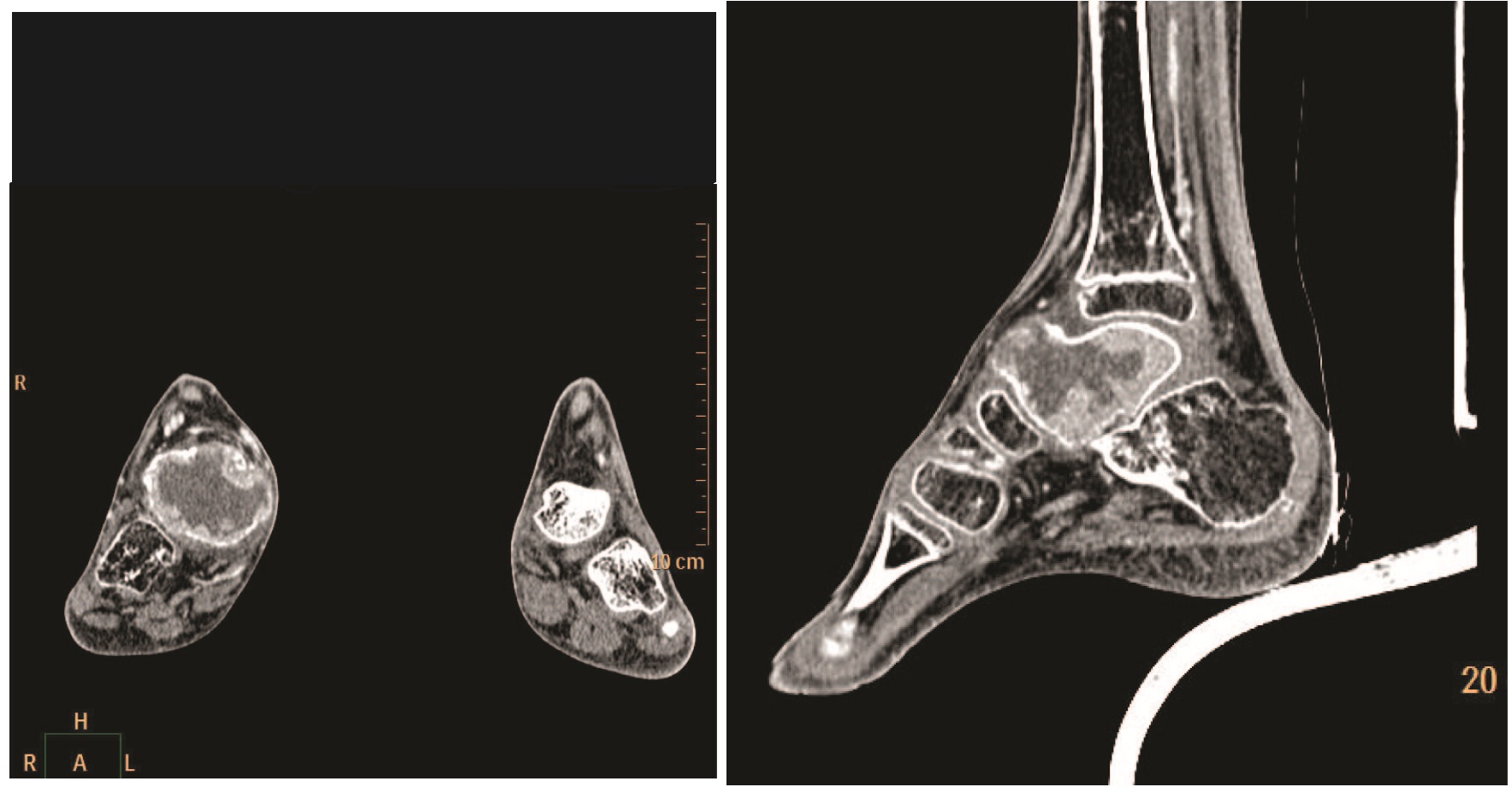
Coronal and Sagittal contrast enhanced CT scan showing a soft tissue mass with peripheral enhancement and minimal extension beyond the confines of the cortex anteriorl
Histopathology showing multiple giant cells on a background of homogenous mononuclear stromal cells

Discussion
Giant cell tumour, also known as osteoclastoma, accounts for approximately 5% of bone tumours and 20% of benign bone tumours [1]. The incidence of GCT is highest in the second to fourth decades of life with a peak in the third and only about 1% occurring in the first decade of life [2]. 50% of GCTs arise around the knee, most often in the distal femur and proximal tibia, followed by the distal radius and then the sacrum. Typically, GCTs are metaphyseo-epiphyseal in location but tend to be metaphyseal in skeletally immature patients. The phalanx, metacarpal, maxilla, and metatarsal are rarely affected and tend to be more aggressive than those in other bones [3].
GCT of the talus usually presents as ankle pain and swelling or sinus tarsi syndrome of several months duration with or without history of trivial trauma. Conventional radiographs demonstrate a lytic lesion centered in the epiphysis but may involve the metaphysis and extend to the adjacent articular cortex. The tumour usually bulges beyond the confines of the cortex. No periosteal reactions are appreciated unless a fracture is present [4]. Histological analysis of biopsy tissue is necessary for diagnosis, as radiological images are not conclusive [5].
The treatment of GCT is directed towards local control without sacrificing joint function. This can be achieved by intralesional curettage with autograft reconstruction by packing the cavity of the excised tumour with morsellised iliac cortico-cancellous bone. Since the recurrence rate is as high as 60%, attempts to extend the curettage or intralesional excision by chemical or physical means such as phenol or cytotoxic agents like chlorpactin have been tried with varying results [6,7].
[1]. Szendroi M, Giant-cell tumour of boneJ Bone Joint Surg Br 2004 86:5-12. [Google Scholar]
[2]. Turcotte RE, Giant cell tumour of boneOrthop Clin North Am 2006 37:35-51. [Google Scholar]
[3]. Biscaglia R, Bacchini P, Bertoni F, Giant cell tumour of the bones of the hand and footCancer 2000 88:2022-32. [Google Scholar]
[4]. Dridi M, Annabi H, Ben Ghozlen R, Abdelkefi M, Trabelsi M, Giant cell tumour of a phalanx in the foot: A case reportActa Orthopædica Belgica 2008 74(2):273-75. [Google Scholar]
[5]. Jarkiewicz-Kochman E, Golebiowski M, Swiatkowski J, Pacholec E, Rajewski R, Tumours of the metatarsusOrtop Traumatol Rehabil 2007 9:319-30. [Google Scholar]
[6]. Carrasco CH, Murray JA, Giant cell tumoursOrthop Clin North Am 1989 20:395-405. [Google Scholar]
[7]. Scully SP, Mott MP, Temple HT, O’keete RJ, O’ Donnell RJ, Mankin HJ, Late recurrence of giant cell tumour of bone. A report of four casesJ Bone Joint Surg Am 1994 76:1231-33. [Google Scholar]