Imaging Diagnosis of Urethral Leiomyoma, usual Tumour at an Unusual Location
Ritu Verma1, Shibani Mehra2, U.C. Garga3, Nishchint Jain4, Krishna Bhardwaj5
1 Senior Resident, Department of Radio-diagnosis, PGIMER & Dr. RML Hospital, New Delhi, India.
2 Senior Specialist, Department of Radiology, PGIMER & Dr. RML Hospital, New Delhi, India.
3 Professor & Head, Department of Radiology, PGIMER & Dr.RML Hospital, New Delhi, India.
4 Senior Resident, Department of Radio-diagnosis, PGIMER & Dr. RML Hospital, New Delhi, India.
5 Senior Resident, Department of Radio-diagnosis, PGIMER & Dr. RML Hospital, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ritu Verma, Senior Resident, Department of Radio-diagnosis, PGIMER & Dr. RML Hospital, New Delhi-110 001, India. Phone : 9582070190, E-mail : drritumamc@gmail.com
Leiomyomas are benign tumours of smooth muscle origin and are the most common uterine masses in females of reproductive age group. Extrauterine leiomyomas are also encountered occassionally and most commonly they involve the genitourinary tract. Leiomyomas arising from urethral smooth muscle are exceptionally unusual which can pose a diagnostic dilemma. Patients usually present with urinary complaints and an intraluminal soft tissue mass bulging from urethral meatus. We are presenting the imaging findings of leiomyoma of distal urethra presenting as a perineal mass with histopathological correlation.
Female urethra, Leiomyoma, MRI, Perineum
Case Report
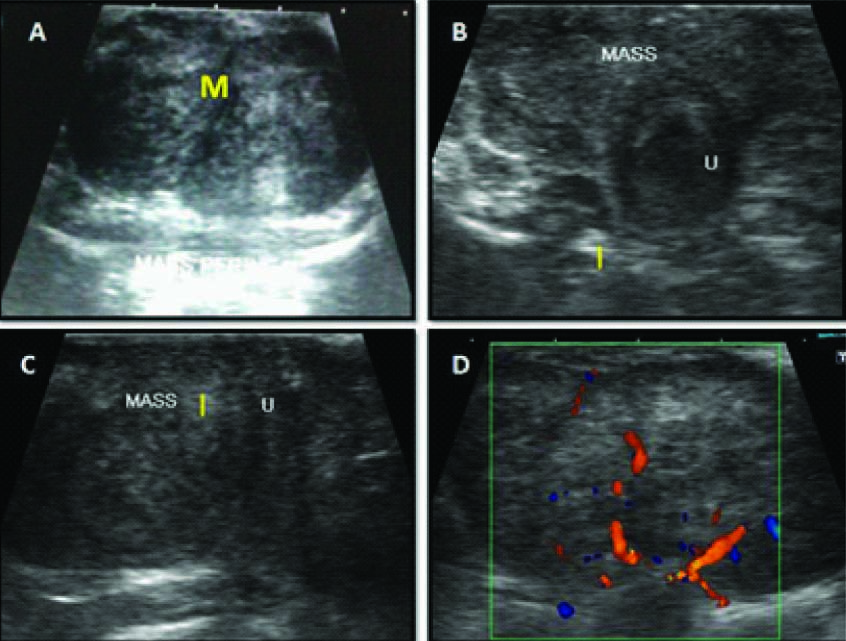
A 38-year-old female presented in July 2012 with gradually enlarging perineal mass and dyspareunia for three years. There were no urinary complaints. On examination a firm non tender submucosal perineal mass was seen beneath labia minora on right side [Table/Fig-1]. Urethral opening was stretched and was located on postero-inferior aspect of the mass. Transperineal and transvaginal USG was performed which revealed a well-defined homogenous iso to hypoechoic perineal mass with whorled appearance, measuring around 4.8 x 4.2 cm abutting the anterior utrethral wall [Table/Fig-2a–d]. Colour doppler USG revealed significant internal vascularity with high resistance arterial flow. Urinary bladder appeared normal with no significant post void residue. Cystourethroscopy was perfomed subsequently and a bulge was noted along superolateral wall of the distal urethra. The overlying mucosa was smooth and mobile. Bilateral ureteric openings and urinary bladder was normal. There was no breach in the urothelial mucosa.
Submucosal perineal mass in anterior urogenital triangle located away from vaginal orifice. The urethral meatus is stretched, located on the postero-inferior aspect,

Transperineal USG images in axial (A & B) and sagittal (C) plane showing well defined iso to hypoechoic homogenous mass, M with whorled appearance, abutting the anterior urethral wall, U with significant internal vascularity on Colour Doppler images (D)
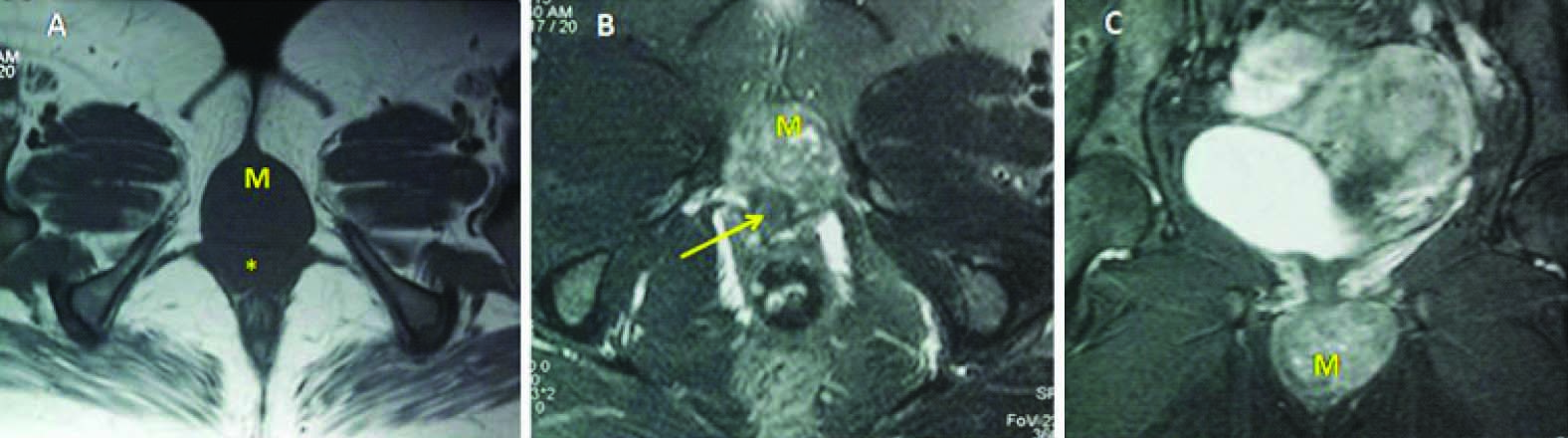
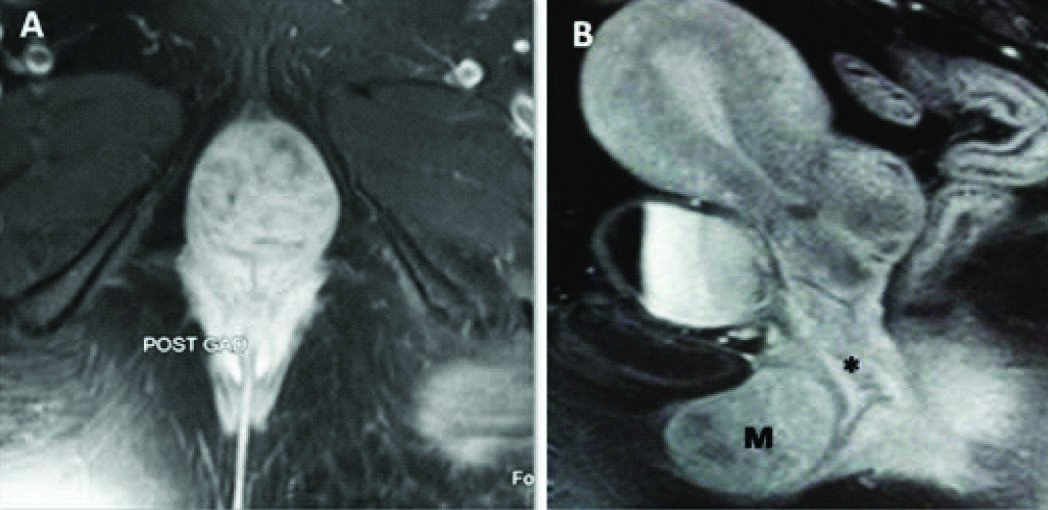
MRI pelvis was done to further characterize the lesion. A well defined solid encapsulated 4 x 5 cm perineal mass lesion was noted in anterior urogenital triangle. The mass was located below the pubic symphysis anterior to both urethra and vagina. The mass was in direct continuity with the anterior wall of urethra without any intervening fat plane [Table/Fig-3a–c]. It appeared isointense to muscle on T1W images and intermediate signal on T2W FS images. On post gadolinium images [Table/Fig-4a,b] there was immediate intense homogenous contrast enhancement. Fat plane with labia minora and adjacent perineal muscles was maintained. Uterus, bilateral ovaries and urinary bladder revealed normal signal intensity and contrast enhancement. Based on USG and MRI findings a diagnosis of urethral leiomyoma was kept and patient was taken for surgical excision of the mass.
T1W (TR:557, TE:10) axial (A) and T2W FS (TR:4280, TE: 105) axial and coronal images (B & C) showing homogenous well encapsulated perineal mass appearing isointense on T1 and intermediate signal on T2W in continuity with anterior urethral wall without intervening fat plane. M = Mass, Urethra (↗), vagina (*).,
Contrast enhanced T1W (TR: 557, TE:10) MRI images in axial and sagittal planes showing intense homogenous contrast enhancement of the mass. M = Mass, vagina (*)
Under spinal anaesthesia after raising the mucosal flaps the mass was excised and the flaps were closed by vicryl 3.0 sutures. The mass was easily separable from all structures except from anterior urethral wall from where it was separated by electrocautry. Foleys catheter was removed after 25 days and the postoperative course was uneventful.
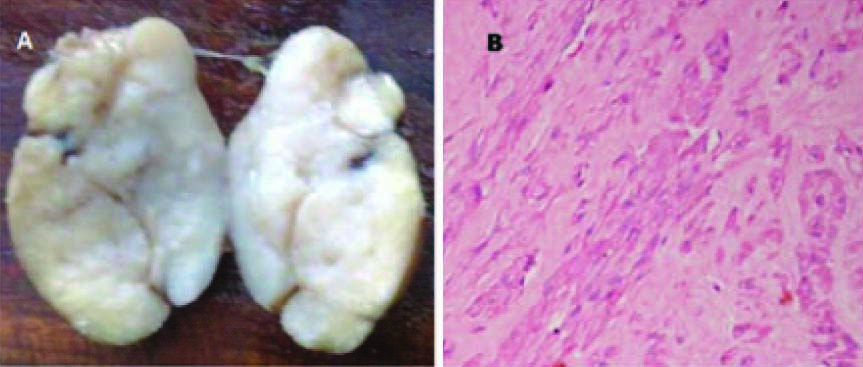
On gross examination the mass appeared well encapsulated, firm, grey white, without any areas of haemorrhage, necrosis or cystic degeneration [Table/Fig-5a]. Microscopy revealed spindle cells arranged in short fascicles with large areas of hyalinization in between suggestive of leiomyoma [Table/Fig-5b]. Individual tumour cell showed mild nuclear pleomorphism, conspicuous nucleoli and scant to moderate eosinophilic cytoplasm. There was no mitotic activity or necrosis. The tumour stained positive for both estrogen and progesterone receptors.
Cut section image of the gross specimen (A) showing well encapsulated solid homogenous mass without any haemorrhage or cystic change. Photomicrograph (B) showing spindle cell tumour arranged in short fascicles with large areas of hyalinization in between suggestive of leiomyoma
On subsequent follow up for last one year there was no recurrence and patient was asymptomatic.
Discussion
The female urethra is 4 cm long and extends from the bladder neck at the urethrovesical junction to the vestibule, where it forms the external meatus located between the labia minora.
Neoplasms involving urethra are rare. They may arise from any of its histological elements, that is, transitional epithelium, stratified squamous epithelium, glandular epithelium and smooth and striated muscles. Amongst the malignant masses Transitional Cell Carcinoma, Squamous Cell Carcinoma, Clear cell adenocarcinoma arising in a urethral diverticulum and Metastasis are known. Benign urethral masses include polyps, papillomas, hemangiomas, fibromas, leiomyomas, fibromyomas, neurinomas and adenomas [1]. Of the benign tumours, caruncles are the most common (96%) urethral masses followed by polyps and papillomas while leiomyomas are exceptionally rare. Leiomyomas are benign tumours of smooth muscle origin. They are the most common uterine masses in females of reproductive age group. However, they may arise at unusual locations and may show unusual growth patterns [2]. Extrauterine leiomyomas most commonly arise in the genitourinary system (vulva, ovaries, urethra and urinary bladder) or less commonly in gastrointestinal tract, however virtually any tissue containing smooth muscles may be involved. Urethral leiomyomas are rare benign tumours of urethra and like uterine leiomyomas they show hormone dependent growth and may also express estrogen and progesterone receptors [3]. The first case of urethral leiomyoma was reported by Buttner [4]. Till now around 40 cases have been reported in literature and only three cases have been reported in males as yet. They tend to occur in women of reproductive age (3rd to 4th decade), enlarge during pregnancy and regress in postpartum period [5].
In the perineum, leimoyomas may arise from urethra, vulva or pararurethral tissue. Urethral leiomyomas most commonly arise from anterior wall of proximal urethra while paraurethral leiomyomas arise from anterior wall of vagina and vesico-vaginal septum [6]. Common presenting symptoms include urinary tract infection (64.3%), a mass (50%), dyspareunia, urinary retention, and irritative lower urinary tract symptoms. Malignant degeneration and metastasis has not been reported as yet. Till date recurrence has been reported in only one case which was more than eight cm in size [7]. While vulvar lesions are not associated with significant postoperative complications, urethral and paraurethral lesions should be excised carefully as postoperative incontinence and urethral strictures may occur. The distinction between urethral and paraurethral masses is also important due to different surgical approach.
USG and MRI are most commonly employed imaging modalities for diagnosing pelvic and perineal masses. MRI is the investigation of choice due to multiplanar imaging, better delineation anatomy and typical signal characteristics helping tissue characterization. Leiomyomas have characteristic whorled appearance on USG and intermediate signal [8] isointense to muscle on MRI with brisk post contrast enhancement.
The differential diagnosis in this case may include urethral diverticulum or urethral caruncle however diverticulum is cystic, circumferential often horseshoe shaped and seen posterolateral to urethra; urethral caruncles are seen on posterior margin of external urethral in post-menopausal females caused by mucosal prolapse and are usually small in size; Polyps and papillomas are usually small intraluminal not intramural masses and show little enhancement on delayed scans. Neurinomas and hemangiomas usually show high signal intensity on T2 [9].
Most cases reported in literature have described urethral leiomyomas as intraluminal masses protruding through the meatus and arising from the proximal [10] urethra. However, in our case the lesion was predominantly intramural producing a perineal mass and was arising from the distal urethra which is unusual. Also, in our case the mass was arising from the anterior urethral wall while more commonly they arise from the posterior wall.
Conclusion
Urethral leiomyomas are rare benign tumours of urethra. Knowledge of perineal anatomy and thin section multiplanar MRI imaging can best tell us the organ of origin and nature of the lesion. Urethral leiomyomas behave like uterine leiomyomas clinically and on imaging. Classical whorled appearance on USG and isointense signal to muscle on MRI with immediate intense homogenous contrast enhancement are key to correct preoperative diagnosis.
[1]. Shield DE, Weiss RM, Leiomyoma of the female urethraJ Urol 1973 109(3):430-31.PubMed PMID: 4692377 [Google Scholar]
[2]. Fasih N, Prasad Shanbhogue AK, Macdonald DB, Fraser-Hill MA, Papadatos D, Kielar AZ, Leiomyomas beyond the uterus: unusual locations, rare manifestationsRadiographics 2008 28(7):1931-48.doi:10.1148/rg.287085095. Review. PubMed PMID: 19001649 [Google Scholar]
[3]. Alvarado-Cabrero I, Candanedo-González F, Sosa-Romero A, Leiomyoma of the urethra in a Mexican woman: a rare neoplasm associated with the expression of estrogen receptors by immunohistochemistryArch Med Res 2001 32(1):88-90.PubMed PMID: 11388165 [Google Scholar]
[4]. Buttner Ein Fall von Myom der Weibliehen Urethra, Z Geburshc Gynδk 1894 28:135-36. [Google Scholar]
[5]. Fry M, Wheeler JS Jr, Mata JA, Culkin DJ, St Martin E, Venable DD, Leiomyoma of the female urethraJ Urol 1988 140(3):613-14.PubMed PMID: 3411686 [Google Scholar]
[6]. Ozel B, Ballard C, Urethral and paraurethral leiomyomas in the female patientInt Urogynecol J Pelvic Floor Dysfunct 2006 17(1):93-5.Epub 2005 May 19. PubMed PMID: 15905997 [Google Scholar]
[7]. Vilar G, Martin JP, Aguado M, Argente G, Leiomyoma of the female urethra: a case report and review of the literatureActas Urol ESP 2010 34(4):396-97. [Google Scholar]
[8]. Siegelman ES, Outwater EK, Tissue characterization in the female pelvis by means of MR imagingRadiology 1999 212(1):5-18.Review. PubMed PMID:10405714 [Google Scholar]
[9]. Chaudhari VV, Patel MK, Douek M, Raman SS, MR imaging and US of female urethral and periurethral diseaseRadiographics 2010 30(7):1857-74.doi:10.1148/rg.307105054. PubMed PMID: 21057124 [Google Scholar]
[10]. Lee MC, Lee SD, Kuo HT, Huang TW, Obstructive leiomyoma of the female urethra: report of a caseJ Urol 1995 153(2):420-1.Review. PubMed PMID: 7815605 [Google Scholar]