Fibromatosis Colli - A Rare Cytological Diagnosis In Infantile Neck Swellings
Sabina Khan1, Sujata Jetley2, Zeeba Jairajpuri3, Musharraf Husain4
1 Assistant Professor, Department of Pathology, HIMSR, Jamia Hamdard University, New Delhi, India.
2 Professor, Department of Pathology, HIMSR, Jamia Hamdard University, New Delhi. India.
3 Associate Professor, Department of Pathology HIMSR, Jamia Hamdard University, New Delhi, India.
4 Associate Professor, Department of Surgery, HIMSR, Jamia Hamdard University, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sujata Jetley, Professor, Department of Pathology, HIMSR, Jamia Hamdard University, New Delhi. India. Phone : 9540248289, E-mail : drjetley2013@gmail.com
Fibromatosis colli or sternocleidomastoid tumour is a rare cause of benign neck mass in infants. It is a self limiting fibroblastic lesion usually presenting with torticollis and a history of birth trauma.It is one of the few causes in which Fine Needle Aspiration Cytology (FNAC) is indicated in a neonate to confirm the diagnosis and to differentiate it from other congenital, inflammatory and neoplastic causes. FNAC provides a rapid, cost-effective, reliable, non invasive method of diagnosis resulting in conservative management of these lesions. We present two interesting cases of neck swelling in infants where FNAC performed as the first diagnostic procedure was instrumental in establishing the diagnosis of fibromatosis colli thus avoiding unnecessary surgical intervention.
Fibromatosis colli, Fine needle aspiration cytology, Infant
Case Report
We report two cases of 40-day-old and 3-week-old male infants in whom FNAC helped in establishing the diagnosis of fibromatosis colli. In both the infants presenting with neck swelling FNAC was performed using a 23G needle attached to a10 ml syringe. The aspirate was air dried and stained with May-Grunwald-Giemsa stain or wet fixed in 95% ethanol and stained with Hematoxylin & Eosin (H&E) as well as Papanicolaou stain.
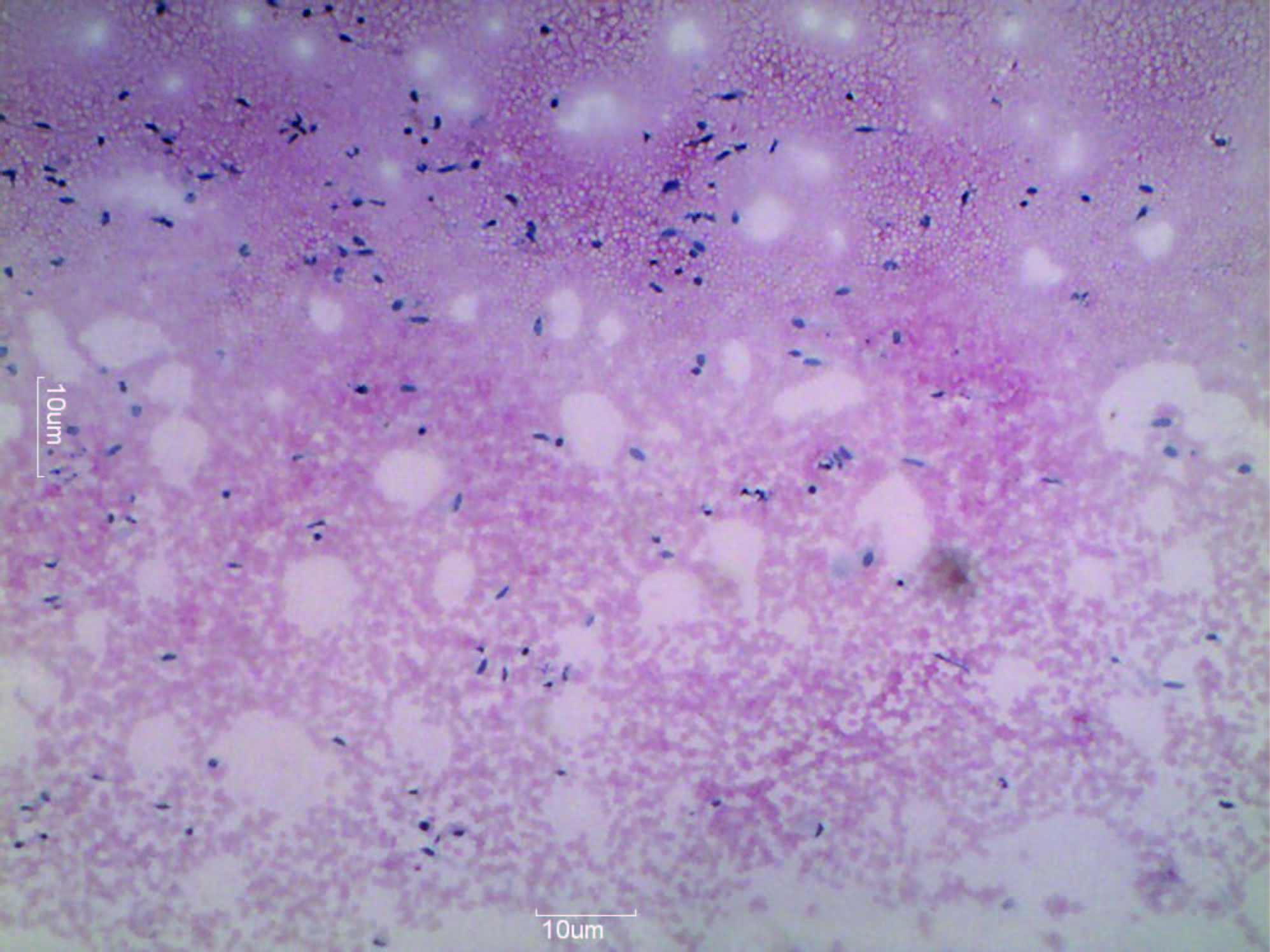
Case 1- A 40-day-old male child presented with firm swelling measuring 2x2 cm on the left side of anterior neck, noticed by the mother ten days back. A history of progressively increasing size was given. There was history of difficult labour with usage of forceps for delivery. On examination restricted neck movements were seen on the affected side. No evidence of other congenital abnormalities was noted. The child was advised FNAC. Characteristic cytomorphological features of fibromatosis colli consisting of proliferating fibroblasts, scattered bare nuclei and muscle giant cells were seen [Table/Fig-1&2]. Collagen was also present. Following this report, reassurance to the parents and conservative management in the form of physiotherapy was started .The swelling showed a slight decrease in size after three weeks, with the neck movements returning to near normal. The mass decreased in size over a period of few months.
Low power view showing numerous spindle shaped fibroblastic cells (Pap stain, 5x)
Few scattered spindle cells with a multinucleated muscle giant cell (MGG stain,40 x)

Case 2- A 3-week-old male infant presented with firm to hard, immobile, 2x1 cm fusiform swelling in right neck just anterior to the sternocleidomastoid muscle. However, there was no torticollis or history of prolonged labour or birth trauma. Clinically lymphadenopathy was the initial concern of the physician. After examination a provisional diagnosis of sternomastoid tumour or cervical tuberculosis was suggested. Patient was advised neck ultrasound which was done at another centre and was suggestive of cervical lymphadenopathy. FNAC was then advised to confirm the diagnosis of tuberculosis. Cytological findings were of moderately cellular smears composed of bland looking spindled fibroblastic cells along with muscle giant cells [Table/Fig-3]. No epithelioid granuloma or evidence of tuberculosis was seen. Based on cytological findings diagnosis of Fibromatosis colli was given. Conservative management was advised which included gentle passive stretching of the affected muscle. Parents were educated regarding proper stretching techniques. The mass gradually decreased in size with conservative management.
Showing multinucleated giant muscle cells. (MGG stain, 40x)

Discussion
Fibromatosis Colli is a rare benign tumour usually presenting in infancy. It is also known as sternomastoid tumour as there is diffuse enlargement of the sternocleidomastoid muscle especially in the lower portion [1]. Its aetiology is uncertain although birth trauma is suggested as a possible cause [2]. Usually it presents with congenital torticollis [3]. It is a rare cause of benign neck mass in infants and needs to be differentiated from other congenital, inflammatory and neoplastic causes occuring in a similar site and age group. FNAC offers a rapid, cheap and non invasive method of diagnosing this condition as it is mostly treated conservatively and rarely requires surgical intervention [4].
Fibromatosis colli mostly appears at 2-4 wk of age. Around 0.4% of all newborns have fibromatosis colli [5]. Majority of affected infants are diagnosed before six months of age. The etiopathogenesis of the lesion is not clear. Various theories have been proposed which include fetal malposition, birth trauma, ischemic necrosis following vascular compression during birth, infection and presence of endogenous factor [6]. The most favoured theory is birth trauma/injury associated with difficult or assisted deliveries including forceps delivery. In present study also there was history of difficult delivery in one case. However, the other patient did not give any such history. According to Kurtycz et al., it is more frequently seen in males as seen in our case too [7]. Fibromatosis colli may be associated with other congenital defects specially muscular disorders like club foot, congenital dislocation of hip etc. However, no such congenital abnormality was seen in the present cases.
Clinically, fibromatosis colli has a characteristic history and clinical presentation. Its differential diagnosis includes congenital lesions such as branchial cyst, thyroglossal cyst, inflammatory lesions like tuberculous lymphadenitis and neoplastic conditions which could be benign (haemangioma, cystic hygroma) or malignant (neuroblastoma, rhabdomyosarcoma & lymphoma).
FNAC is considered the first line investigation in the diagnosis of infantile fibromatosis colli and helps in excluding other causes. It is a rapid, cheap and reliable diagnostic procedure which helps in avoiding more invasive and costly procedures. Radiological imaging modalities such as ultrasonography and computed tomography maybe helpful in the diagnosis [8]. However, the cost and availability of these procedures limits its use.Very few published reports are available on the cytologic features of fibromatosis colli. A comparison of cytological findings of fibromatosis colli published in various studies is given in [Table/Fig-4]. A study of eight cases of fibromatosis colli was undertaken by Sharma et al., and its cytomorphological features assessed [9]. The characteristic features described are bland appearing fibroblasts and degenerative, atrophic skeletal muscle in a clean background. Similar study was done by Kurtycz et al., on ten cases of infantile fibromatosis colli [7]. Pereira et al., in a study presented eight cases of fibromatosis colli accurately diagnosed by FNA cytology [10].
Comparison of Cytological findings in various studies
| S no | Study | Cytological findings |
|---|
| 1 | Sharma S et al., 2003 | Bland-appearing fibroblasts, degenerative atrophic skeletal muscle,muscle giant cells; numerous bland, bare nuclei; and parallel clusters of fibroblasts |
| 2 | Rajlakshmi et al., 2009 | Sheets of spindle cells,atrophic muscle fibres, regenerating muscle giant cells. |
| 3 | Chakrabarti et al., 2010 | Plump and normal fibroblasts,atrophic muscle fibres, multinucleated regenerating muscle cells. |
| 4 | Baisakh et al., 2012 | Clusters of spindle shaped fibroblast with wispy cytoplasm, multinucleated muscle giant cells |
| 5. | Present study 2014 | Proliferating fibroblasts, scattered bare nuclei and muscle giant cells |
The condition is generally self limited. Most of the cases respond to conservative management. When diagnosed early, it is managed in a non-surgical manner which involves passive stretching and physiotherapy. Surgical intervention maybe required only in refractory cases or in a child greater than one year of age [11]. Prognosis is worse in children diagnosed and treated when older than one year.
Conclusion
To conclude, FNAC provides a confirmatory non invasive diagnosis of fibromatosis colli. Its importance lies in the fact that if diagnosed early around 90% of these case regress with conservative management thereby avoiding unnecessary surgery in an infant.
[1]. Baisakh MA, Mishra M, Narayanan R, Mohanty R, Cytodiagnosis of sternocleidomastoid tumour of infancyJ Cytol 2012 29:149-51. [Google Scholar]
[2]. Goldblum JR, Weiss SW, Fibrous tumours of infancy and childhood. In: Goldblum JR, Weiss SW. (Eds)Enzeinger and Weiss's Soft tissue tumours 2001 4th edSt. LouisMosby:273-75. [Google Scholar]
[3]. Apple SK, Nieberg RK, Hirschowitz SL, Fine needle aspiration diagnosis of fibromatosis colli. A report of three casesActa Cytol 1997 41:633-35. [Google Scholar]
[4]. Rajalakshmi V, Selvambigai G, Jaiganesh Cytomorphology of fibromatosis colliJ Cytol 2009 26:41-42. [Google Scholar]
[5]. Porter SB, Blund BW, Pseudotumour of infancy and congenital muscular torticollisAm Family Phys 1995 52:1731-36. [Google Scholar]
[6]. Kumar B, Pradhan A, Diagnosis of sternomastoid tumour of infancy by fine needle aspiration cytologyDiagn Cytopathol 2011 39:13-17. [Google Scholar]
[7]. Kurtycz DF, Logrono R, Hoerl HD, Heatley DG, Diagnosis of fibromatosis colli by fine needle aspirationDiagn Cytopathol 2000 23:338-42. [Google Scholar]
[8]. Chakrabarti I, Bandopadhyay A, Goswami BK, Fine Needle Aspiration Cytology of Fibromatosis ColliTurkish Journal of Pathology 2010 26:243-44. [Google Scholar]
[9]. Sharma S, Mishra K, Khanna G, Fibromatosis Colli in Infants. A cytologic study of eight casesActa Cytol 2003 47:359-62. [Google Scholar]
[10]. Pereira S, Tani E, Skoog L, Diagnosis of fibromatosis colli by fine needle aspiration (FNA) cytologyCytopathology 1999 10:25-29. [Google Scholar]
[11]. Raab SS, Silverman JF, McLeod DL, Banning TL, Geisinger KR, Fine needle aspiration biopsy of fibromatosiesActa Cytol 1993 37(3):328-28. [Google Scholar]