Nose is the most prominent part of face with great aesthetic significance and functional importance. Non-neoplastic and neoplastic lesions of nasal cavity, paranasal sinuses and nasopharynx are very commonly encountered in routine clinical practice [1]. They are a common finding in all the age groups.Common presenting symptoms of sinonasal lesions are nasal blockade, nasal discharge, epistaxis, facial swelling, orbital and ear symptoms [2]. Although, clinical complaint of a mass in nose seems to be a simple problem but it gives arise to a large number of differential diagnosis in the mind of treating physician and diagnosing pathologists. Sinonasal area is exposed to various infective agents, chemicals, antigens, mechanical and many other influences. These deleterious exposures lead to formation of tumour like and neoplastic conditions [3]. They can range from simple nasal polyps to infective polypoidal granulomatous lesions to malignant lesions. Nasal polyps are the most common cause of nasal obstruction with 04% of prevalence rate [4]. Their exact pathogenesis is unknown but they have association with allergy, asthma, infections and aspirin sensitivity [4].
Benign lesions of sinonasal region are common and lack of appreciation of these lesions can lead to radical surgeries. They have long clinical history with frequent local recurrence and thus relatively significant morbidity.Malignant lesions in nasal cavity, paranasal sinuses and nasopharynx accounts for not more than 3% of head and neck malignancies and less than 1% of all the malignant tumours. Geographically, they have tendency for Africans, Japanese and Arabians and are rarely seen in Americans and Western Europeans [5]. Due to varieties of histopathological types and grades of malignancies, it is very important to study their clinical and pathological aspects. Coupled with radiological techniques, histopathology has become indispensable in the timely diagnosis and treatment of these lesions [6,7].
The aim of this prospective study was to categorize these lesions into non neoplastic and neoplastic and to study their clinical and histopathological patterns and to compare their incidences.
Materials and Methods
This is a prospective study of 147 cases, conducted in the Department of Pathology of a tertiary care Hospital in Rajasthan, India, for the period of January 2013 to January, 2014. Demographic data regarding age, sex, chief complaints, clinical examination and radiological investigations was retrieved from histopathology and OPD records.
The inclusion criteria for selection of cases was medically untreatable cases of masses in nasal cavity, paranasal sinuses and nasopharynx, requiring surgical treatment and are fit for surgery. All the received biopsies were fixed in 10% buffered formalin. After routine gross examination and processing, Hematoxylin & Eosin staining for histopathological examination was done. Immunohistochemistry was used wherever required.
Results
In the present study, the age distribution of patients ranged from less than 1 to 76 y (mean age – 29.1 y). Patients in second and third decades are commonly affected with male to female ratio of 1.98:1. The most common presenting symptoms were nasal obstruction in 128 patients (87.07%) followed by nasal discharge in 102 patients (69.39%). Other less common complaints were headache due to sinusitis, sneezing, nasal bleeding, change in voice, decreased sense of smell and facial swelling.
Among total 147 cases, there were 91 cases of nasal and paranasal sinus masses and 56 cases of nasopharyngeal masses.
Nasal and paranasal sinus masses- Histopathological examination revealed that out of total 91 nasal and paranasal sinus masses, there were 67 (73.6%) non-neoplastic and 24 (26.4%) neoplastic lesions.
Among the 67 non-neoplastic lesions, inflammatory polyp was the commonest one with 60 cases (89.5%) followed by fungal infection in 5 cases (7.5%), rhinosporodiosis in 1 case (1.5%) and one case of glioma (1.5%) [Table/Fig-1].
Histopathological diagnosis of non-neoplastic lesions of nose and paranasal sinuses
| Non-neoplastic lesions | Incidence (Number of cases) | Percentage (%) |
|---|
| Inflammatory Polyp | 60 | 89.5 |
| Fungal infection | 5 | 7.5 |
| Rhinosporidiosis | 1 | 1.5 |
| Nasal glioma | 1 | 1.5 |
| Total | 67 | 100 |
Inflammatory polyp was the most frequently encountered in sinonasal region with a peak in second and third decades of life. These polyps were bilateral in the majority of the patients, presented with the symptoms of nasal obstruction, sinusitis, headache and nasal discharge. Microscopically, these polyps comprised of loose mucoid stroma and mucous glands lined by respiratory epithelium. Inflammatory infiltrate of lymphocytes, plasma cells, neutrophils and eosinophils was noticed in this loose stroma. Allergic polyps show more eosinophilic infiltrate as compared to other inflammatory cells.
Fungal infections were seen in third decade, presented with foul smelling discharge and on microscopy exhibited inflammation of neutrophils and histiocytes in the granulation tissue. The culture was positive on Sabouraud’s dextrose agar medium, confirming its fungal origin. Aspergillosis was the commonest fungal infection.
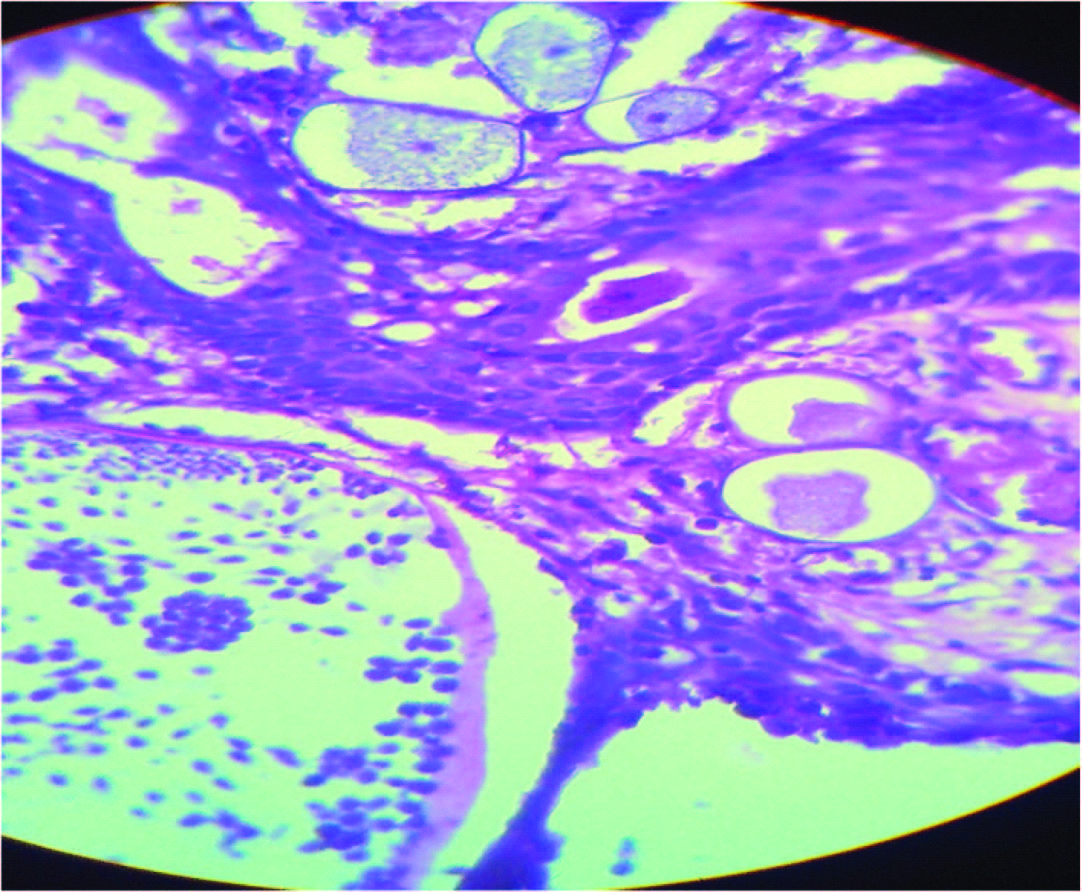
Rhinosporodiosis was seen in fifth decade and in microscopic examination, showed many diagnostic globular sporangia containing numerous spores [Table/Fig-2].
Rhinosporodiosis, multiple sporangia containing numerous spores (H & E stainX400)
A case of nasal glioma was seen in a nine months old female child presenting with a firm, non-compressible polypoidal mass in nasal cavity. Microscopically, this mass was composed of astrocytic neuroglial tissue, interlacing with fibrous and vascular connective tissue, which is lined by respiratory mucosa.
Out of 24 neoplastic lesions, there were 11 (45.83%) cases of benign tumours and 13 cases (54.17%) of malignant tumours. Among the benign tumour, inverted papilloma was the most common lesion in five cases (45.46%). Others were two cases of angiofibroma (18.18%), two of capillary hemangioma (18.18%) and two cases of schwannoma (18.18%) [Table/Fig-3].
Histopathological diagnosis of benign neoplastic lesions of nose and paranasal sinuses
| Benign lesions | Incidence (Cases) | Percentage (%) |
|---|
| Inverted papilloma | 5 | 45.46 |
| Angiofibroma | 2 | 18.18 |
| Capillary hemangioma | 2 | 18.18 |
| Schwannoma | 2 | 18.18 |
| Total | 11 | 100 |
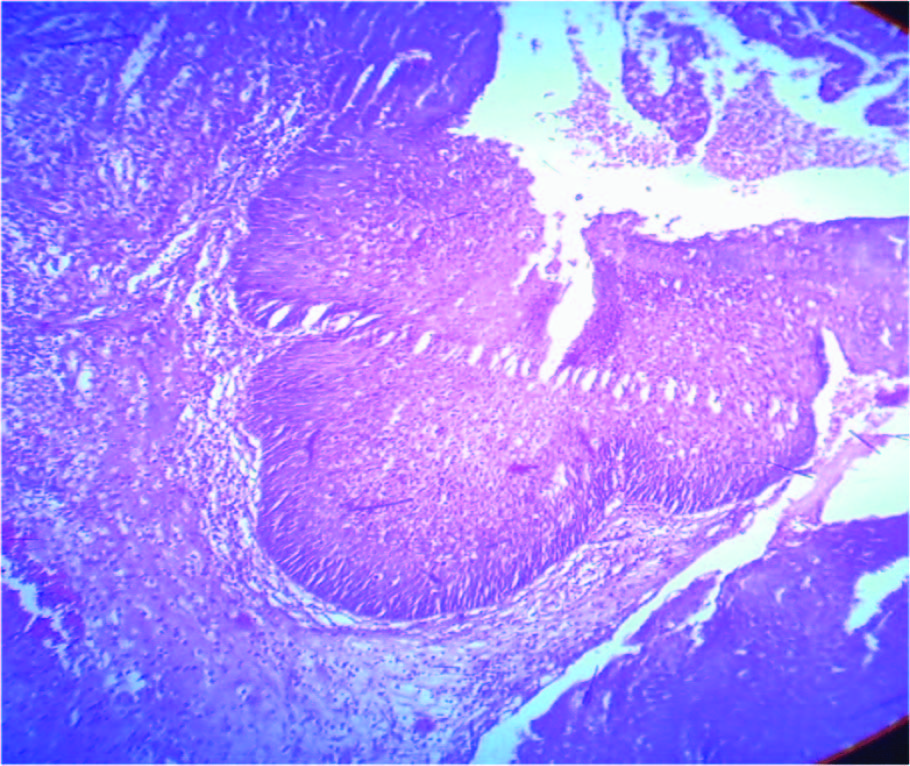
Inverted papillomas presented in second and third decades with nasal obstruction, mass and epistaxis. Microscopically, they were composed of invaginations of squamous epithelium into the underlying stroma [Table/Fig-4]. Angiofibromas were seen in 2nd decade with the microscopy of intricate mixture of blood vessels and fibrous stroma. Other benign lesions, capillary hemangioma and schwannoma presented in third to fourth decades with characteristic microscopic picture.
Inverted papilloma with typical inverted pattern of growth (H&E stainX100)
Among 13 malignant cases, squamous cell carcinoma constituted majority of six cases (46.15%) followed by two cases (15.4%) of primitive neuroectodermal tumour and one case each of basal cell carcinoma (7.69%), hemangiopericytoma (7.69%),neuroblastoma (7.69%), round cell tumour (7.69%) and plasmacytoma (7.69%) [Table/Fig-5].
Histopathological diagnosis of malignant neoplastic lesions of nose and paranasal sinuses
| Malignant lesions | Incidence (Cases) | Percentage (%) |
|---|
| Squamous cell carcinoma | 6 | 46.15 |
| Primitive neuroectodermal tumour | 2 | 15.4 |
| Basal cell carcinoma | 1 | 7.69 |
| Hemangiopericytoma | 1 | 7.69 |
| Neuroblastoma | 1 | 7.69 |
| Round cell tumour | 1 | 7.69 |
| Plasmacytoma | 1 | 7.69 |
| Total | 13 | 100 |
Squamous cell carcinoma was the most common malignant lesion, observed in 6th and 7th decades. Histologically, tumour cells were arranged in nests, masses or groups with the evidence of squamous differentiation in form of intracellular keratin, intercellular bridges and extracellular keratin pearls.
Next common were two cases of primitive neuroectodermal tumour. Immunohistochemistry was done in one case which was focally positive for CD99, positive for vimentin and NSE and negative for AE1/AE3, EMA, LCA, desmin and chromogranin, which confirmed the diagnosis of PNET/Ewing’s sarcoma [Table/Fig-6]. Next was one case of hemangiopericytoma which microscopically appeared highly cellular with round to oval tumour cells arranged around blood vessels but they show mild atypia, necrosis and mitotic activity. Then was one case each of basal cell carcinoma and neuroblastoma both seen in male patients with typical histology.
PNET-Ewing’s sarcoma demonstrating immunoreactivity by CD-99 (H&E stain 400X)

HPE was suggestive of round cell tumour in one case but immunohistochemistry (positive for LCA and negative for CK, vimentin, HMB-45, CD99) confirmed it to be a Non-Hodgkin’s Lymphoma. IHC also confirmed the histopathological diagnosis of plasmacytoma by positive kappa chain and negative LCA and lambda light chain.
Nasopharyngeal masses – The age of patients ranged from 1-11 y. Out of total 56 nasopharyngeal masses, there were 53 (94.6%) non-neoplastic and 3 (5.4%) neoplstic lesions [Table/Fig-7]. Among the 53 non-neoplastic lesions, majority comprised of 52 (98.11%) cases of adenotonsillar hypertrophy and only one case (1.89%) of inflammatory polyp. Out of 3 neoplastic lesions, there were one case each of adenocarcinoma, non-hodgkin’s lymphoma and leiomyosarcoma.
Histopathological diagnosis of Nasopharyngeal masses
| Nature of lesion | Histopathological diagnosis | Number of cases |
|---|
| Non neoplastic lesions | Adenotonsillar hypertrophy | 52 |
| Inflammatory polyp | 1 |
| Neoplastic lesions | Adenocarcinoma | 1 |
| Non-hodgkin’s lymphoma | 1 |
| Leiomyosarcoma | 1 |
| Total | | 56 |
Microscopically, adenocarcinoma revealed a well differentiated seromucinous composition with tubulopapillary architecture. Non-Hodgkin’s lymphoma showed diffuse discohesive pattern of medium to large sized neoplastic cells with large round to oval nuclei and prominent nucleoli. Necrosis and atypical mitotic activity were also noted. Leiomyosarcoma showed typical histomorphology.
Discussion
Masses in nasal cavity, paranasal sinuses and nasopharynx form a heterogeneous group of lesions with a broad spectrum of histopathological features. A variety of these non-neoplastic and neoplastic lesions are quite impossible to differentiate clinically and they are mostly clinically diagnosed as nasal polyp [8]. They are frequently neglected by the clinicians as infective or allergic aetiology. Benign sinonasal disorders account for a major proportion of visits to hospital. The lack of differentiation of benign and malignant disorders at initial presentation leads to significant delay in the initial diagnosis and therapy.
In the present study, these masses had predilection for males demonstrating a male to female ratio of 1.98:1 similar to a study by Zafar et al., [1]. A Nigerian study revealed female preponderance with opposite M: F ratio of 1:1.2 [9]. The common presentation of sinonasal masses were rhinorrhea, headache, nasal obstruction comparing favorably with other studies [8–10].
Regarding age, current study revealed 2nd and 3rd decades of life were the most vulnerable period as observed by Bakari et al., [9] and Zafar et al., [1]. Malignant lesions have been generally reported in 6th-7th decades in concordance with Patel et al., [11].
Non-neoplastic lesions made 81.6% of the total cases of nasal cavity, paranasal sinuses and nasopharynx in our study. Similarly a high proportion of non-neoplastic lesions are also reported in the study by Zafar et al., [1] revealing 89% of non-neoplastic lesions in their study.
Nasal polyps are the commonest lesion of nasal cavity. Its exact pathogenesis is not known but they have strong association with allergy, asthma, aspirin sensitivity and infection. Among, masses of nasal cavity and paranasal sinuses, the incidence of nasal polyp was 65.9% in concordance with Tondon et al., [6] (64%) and Dasgupta et al., [8] (62.5%). In our study, five cases of fungal infection (5.49%) were seen in 3rd decade, comparable to Modh et al., [12]. During one year of study period, we found only one case of rhinosporodiosis (1.09%) similar to Pradhananga et al., [10] (0.69%). This is a chronic granulomatous lesion, caused by rhinosporodiosis seeberi. Nasal glioma is a congenital malformation of choristoma of mature glial tissue discontinuous with intracranial component and presents with respiratory abnormalities. It is a rare lesion, accounting for only one case, below one year of age, similar to as observed in a study from Nepal [13]. Rahbor et al., [14] observed in their review study of nine cases of nasal glioma that the mean age of presentation was nine months.
Nasal papilloma is said to be a commonly occurring benign neoplastic lesion. We have observed five cases of inverted papilloma, forming 45.46% of all benign neoplastic masses, slightly higher from findings of Humayun et al., [15] (33.33%). We have reported two cases of angiofibroma in adolescent males, presenting with profuse recurrent epistaxis as the chief complaint, comparable to the finding of three cases by Parajuli S et al., [13]. They are typical lesions reported in young people with histological findings of blood filled spaces separated by fibrous tissue. Capillary hemangiomas constituted 18.18% of benign neoplasms as observed 19.4% by Modh et al., [12]. These lesions presented as bleeding nasal polyps. This neoplasm has been regarded as a hamartoma or malformation rather than a true neoplasm.
Schwannomas in the nasal cavity are rare. We encountered two cases both in females aged 15-27 y as observed by Modh et al.,[12]. Histology revealed uniform spindle cells arranged in loose stroma (Antoni B) and palisading arrangement of nuclei (Verocay body).
Malignant lesions of sinonasal tract are rare [16]. Malignant polypoidal lesions masquerade as simple nasal polyps or chronic inflammatory masses, causing delay in the diagnosis.Squamous cell carcinoma is the commonest histological type [17]. In our study, squamous cell carcinoma constituted 46.15% comparable to Modh et al., [12] and Panchal et al., [18]. It was more common in 6th and 7th decades of life as documented by Ghosh and Bhattacharya [19]. We encountered only one case of extramedullary plasmacytoma. They are uncommon tumours accounting for 1% of all head and neck tumours. Hemangiopericytoma is a rare angiogenic tumour constituting 7.69% of all malignant lesions which is slightly higher than that observed by Modh et al., (5%) [12]. In the present study, one case of non-Hodgkin’s lymphoma was reported accounting for 7.69% of malignant tumours, confirmed by IHC. Olfactory neuroblastoma is a rare neuroectodermal tumour arising from olfactory sensory epithelium in upper nose. There was a single case of olfactory neuroblastoma in concordance with ParajuliS et al., [13] accounting for 7.69% of malignant tumours.
Nasopharyngeal masses are not an uncommon entity. Such masses either arise from nasopharynx or from neuroectoderm or nose and paranasal sinuses and present as mass in nasopharynx. Such patients present with nasal obstruction, mouth breathing, epistaxis and earache. In the present study, majority of nasopharyngeal masses were of adenotonsillar hypertrophy in contradiction to Biswas et al., [20] reporting antrochoanal polyp as the commonest nasopharyngeal masses although they have reported that in the patients of age group of 0-10 y, 86% cases were of adenotonsillar hypertrophy in concordance to present study with majority of cases in age group of less than 10 y.
In the present study, various lesions were distributed into non-neoplastic and neoplastic lesions and compared with previous studies. A high incidence of malignant lesions was observed in our study. Among non-neoplastic lesions, inflammatory polyp was the most common lesion. Among benign neoplastic lesions, inverted papilloma was the commonest one and squamous cell carcinoma was most common malignant lesion. Surgical excision is the main modality of treatment in most of non-neoplastic and benign neoplastic masses and wide surgical excision, radiotherapy or chemotherapy in malignant masses. Regular follow up is necessary for early detection of recurrence or metastases.
Conclusion
Masses of nasal cavity, paranasal sinuses and nasopharynx are a common problem in today’s environment as diagnostic and therapeutic dilemma. Due to the overlapping presentation of lesions of this region with more commonly encountered inflammatory and infectious diseases, role of histopathological examination needs to be understood and is mandatory for proper and early treatment of the patient. The purpose of present study is to present various differential diagnoses of sinonasal masses with their histopathological correlation.