Regional anaesthesia (spinal anaesthesia) is widely used as a safe anaesthetic technique for both elective and emergency operations. Shivering is known to be a frequent complication, reported in 40 to 70% of patients undergoing surgery under regional anaesthesia [1,2]. Shivering can be very unpleasant and physiologically stressful for the patients after enjoying the comforts of modern anaesthetics [3].
Various methods are available for the control of shivering during anaesthesia. Non-pharmacological methods using equipments to maintain normothermia are effective but may be expensive and are not practical in all the settings. Pharmacological methods using various drugs like Pethidine, Clonidine, Doxapram, Ketanserine, Tramadol, Nefopam etc. have been tried which are simple, cost effective and easily available.
Here, we have compared Tramadol, a synthetic opioid with Pethidine, the gold standard drug for the treatment of shivering, in the quest for more safe and efficacious drug. In our study this we compared the efficacy, potency, haemodynamics effects and complications or side effects of Tramadol with that of Pethidine for the control of shivering.
Materials and Methods
After obtaining approval of the ethics committee, a prospective double blinded randomised study was conducted at the PES Institute of Medical Sciences and Research, Kuppam. A total of 40 patients belonging to both sexes aged between 20 to 50 y of ASA grades 1 and 2 scheduled to undergo various surgical procedures under neuraxial blockade were selected. Patients with compromised cardiovascular function, endocrine abnormalities like thyroid disease and Diabetes Mellitus, patients on long term phenothiazines and MAO inhibitors and patients having fever were excluded from the study.
All patients who developed post spinal anaesthesia intraoperative shivering grade 3 and grade 4 were randomly allocated to two groups: Group P (n=20) received Pethidine 0.5mg/kg IV and group T (n=20) received tramadol 1.0 mg/kg IV.
Grading of shivering was done as per Wrench[4], which is as follows:
Grade 0: No shivering
Grade 1: One or more of the following: Piloerection, Peripheral vasoconstriction, peripheral cyanosis with, but without visible muscle activity
Grade 2: Visible muscle activity confined to one muscle group
Grade 3: Visible muscle activity in more than one muscle group
Grade 4: Gross muscle activity involving the whole body
All operation theatres in which the operations were performed maintained constant humidity (70%) and an ambient temperature of around 21°C to 23°C. Oxygen was administered to all the patients of both groups at a rate of 5 L/min with face mask and patients were covered with drapes but not actively warmed. No means of active re-warming were used. Intravenous fluids and anaesthetic drugs were administered at room temperature.
All the patients were pre-loaded with Ringer Lactate 10 ml/kg before giving neuraxial blockade. Injections atropine and glycopyrrolate were not used as premedicant drugs. Baseline pulse rate, Blood Pressure (BP), oxygen saturation (SpO2) and body temperature (axillary) were recorded. Subarachnoid block was given with inj. Bupivacaine 0.5% (10-15 mg) at L3-4 or L4-5 interspace using 25 gauge Quincke’s needle and blockage up to T9-10 dermatome was achieved.
Patients who developed either grade 3 or grade 4 of shivering were included in the study. The attending anaesthesiologist recorded the severity of the shivering, time to disappearance of shivering (in minutes) and response rate (shivering ceased after treatment in 15 min). If the shivering did not subside by 15 min, the treatment was considered to be not effective. Recurrence of shivering was also noticed until the patient left the operation theatre. Patients who did not respond or in whom recurrence of shivering occurred were treated with additional dose of pethidine (0.25 mg/kg IV) or tramadol (0.5 mg/kg IV) in the respective groups.
Side effects like nausea, vomiting, bradycardia (<50/min) and hypotension (>20% of baseline) were recorded. Bradycardia, hypotension and vomiting were treated with atropine, mephenteramine and metoclopramide, respectively, in titrated doses when required.
Statistical Analysis
Statistical analysis was done using suitable statistical software, Student t-test and Chi-square test were applied for the interpretation of results. A p-value <0.05 was considered statistically significant.
Results
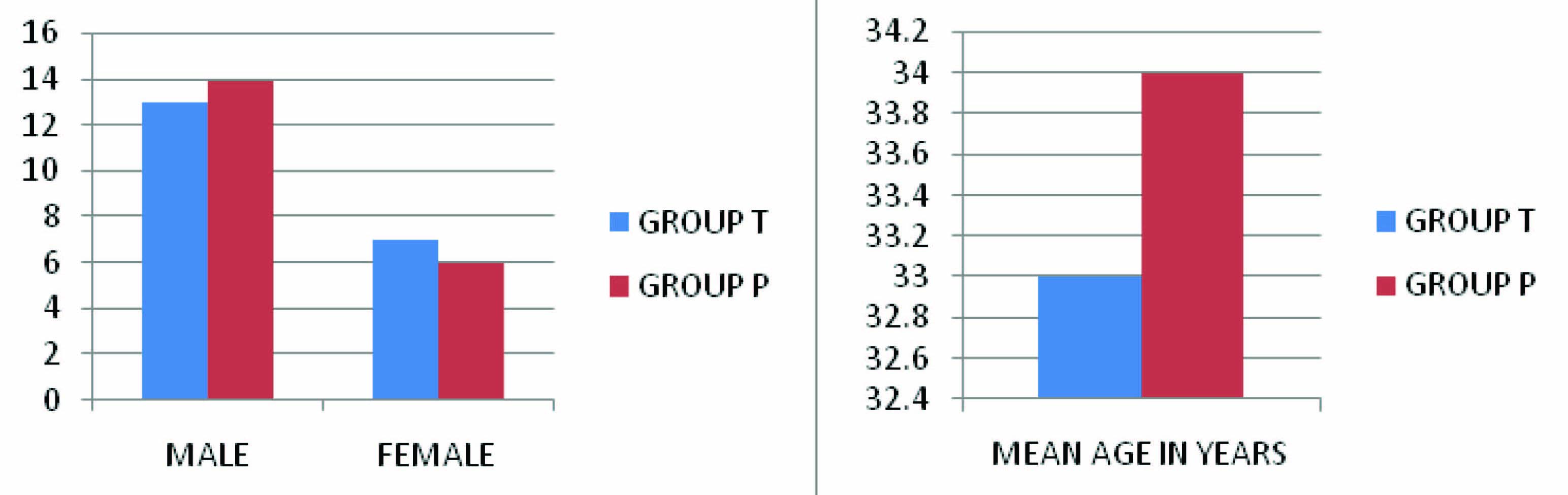
Forty patients were studied, 20 in each Group and the demographic data are summarized in [Table/Fig-1,2,3]. There was no significant difference found in the axillary temperature as well as shivering grades at the start of study between the two groups.
| Tramadol (n=20) | Pethidine (n=20) | t | p | |
|---|
| Age (Yrs) | 33±9.65 | 34.55±8.98 | 2.024 | 0.6 | NS |
| Sex (M:F) | 13:7 | 14:6 | - | 1 | NS |
| Weight (Kg) | 52.35±6.12 | 51.65±5.12 | 2.026 | 0.7 | NS |
| ASA PS (I:II) | 14:6 | 13:7 | - | 1 | NS |
| Tramadol | Pethidine | t | p | |
|---|
| Temp (°C) | 36.6±0.129 | 36.56±0.153 | 2.024 | 0.206 | NS |
| Shivering Grade | 2.75±0.444 | 2.5±0.513 | - | 0.1908 | NS |
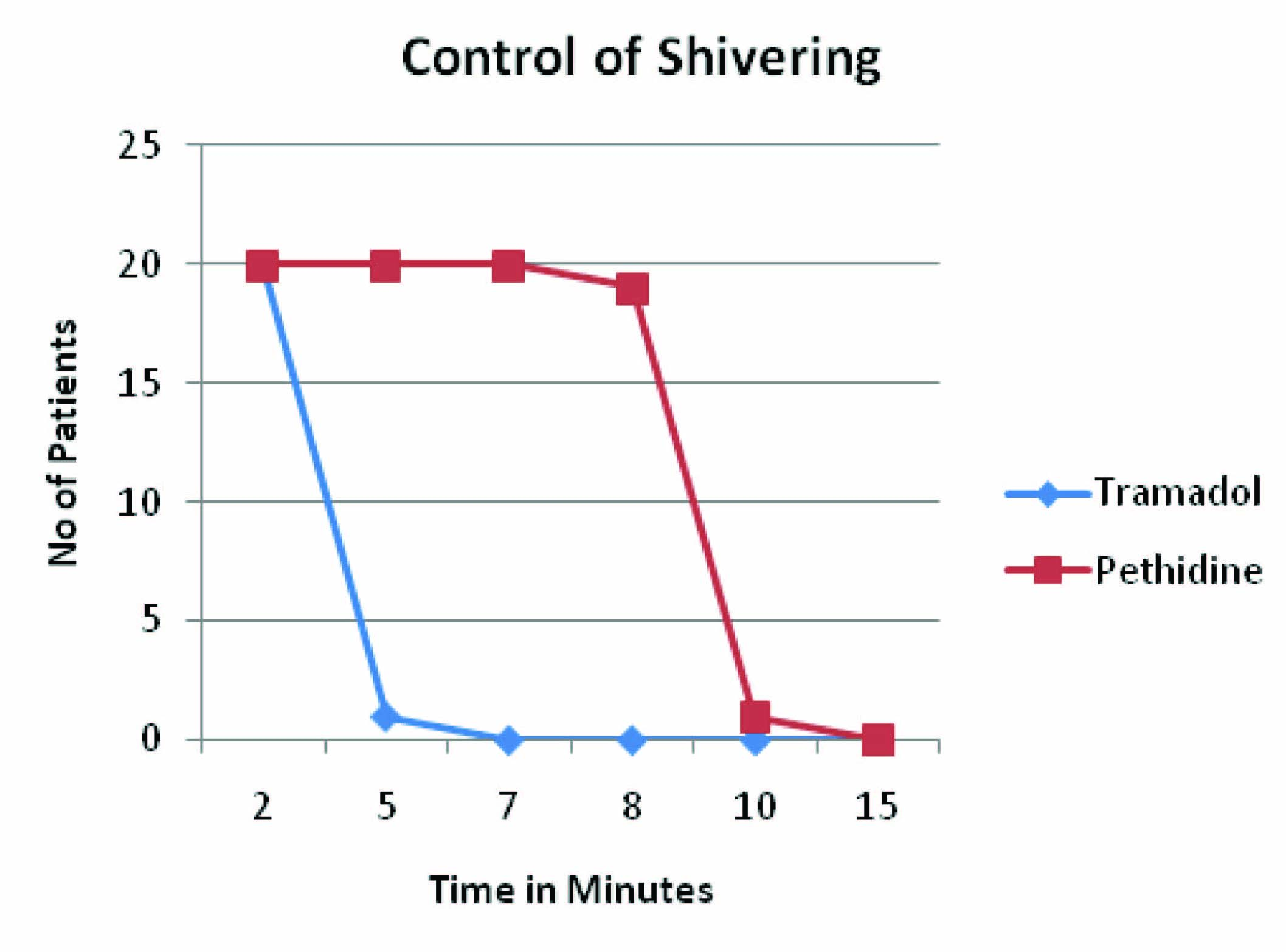
Shivering disappeared in all the patients (20) of group T by two minutes but in group P disappearance of shivering was achieved at end of five minutes. The time interval between administration of drug after onset of shivering and disappearance of shivering was significantly shorter in the Tramadol group [Table/Fig-4].
Onset of Disappearance of shivering
| Time (Minutes) | Tramadol (n=20) | Pethidine (n=20) | p | |
|---|
| 1 | 0 (0%) | 0(0%) | 1 | |
| 2 | 20 (100 %) | 0(0%) | <0.0001 | Significant |
| 3 | 20 (100 %) | 0(0%) | <0.0001 | Significant |
| 5 | 20 (100 %) | 20 (100%) | 1 | |
Both the drugs were found to be effective in reducing shivering. Nineteen patients in the Group T had control of shivering at end of five minutes but there were no patients who had control of shivering Group P (p < 0.0001) which is statistically significant [Table/Fig-5].
Control of shivering (p < 0.0001)
There was no statistically significant difference with respect to heart rate, mean blood pressure and axillary temperature between the two groups [Table/Fig-6].
| | Tramadol (n=20) | Pethidine (n=20) | t | p | |
|---|
| Basal | Mean BP | 87.45±7.149 | 87.15±6.277 | 2.026 | 0.888 | NS |
| Mean PR | 81.3±15.32 | 76.6±7.989 | 2.045 | 0.233 | NS |
| During Shivering | Mean BP | 96.65±17.44 | 92.1±6.24 | 2.064 | 0.283 | NS |
| Mean PR | 86.55±18.09 | 82.15±8.235 | 2.052 | 0.331 | NS |
| Post Drug admin-istration | 2 Min | Mean BP | 92.8±9.78 | 89.6±6.295 | 2.037 | 0.746 | NS |
| Mean PR | 83.95±8.42 | 81.7±8.06 | 2.055 | 0.621 | NS |
| 5 Min | Mean BP | 91.25±9.239 | 89.6±6.46 | 2.032 | 0.517 | NS |
| Mean PR | 84.65±17.16 | 80.4±7.83 | 2.052 | 0.322 | NS |
The incidence of recurrence of shivering was 50% in pethidine group while only in 10% in tramadol group. Complications like nausea and vomiting occurred in 40% in pethidine group while 5% in tramadol group [Table/Fig-7]. The difference is statistically significant.
Recurrence and complications
| Tramadol (n=20) | Pethidine (n=20) | p | |
|---|
| Recurrence | 2 (10%) | 10 (50%) | 0.176 | Significant |
| Nausea and Vomiting | 1 (05%) | 8 (40%) | 0.48 | Significant |
Discussion
Regional anaesthesia including central neural blockade and peripheral nerve blockade is a safe and popular technique for various surgeries. Around 40-60% of the patients under regional anaesthesia develop shivering, though it is found commonly after general anaesthesia. The probable mechanism under regional anaesthesia could either be a result of decrease in core body temperature or misinformation from receptors [5].
Shivering is a potentially serious complication, resulting in increased metabolic rate; increased oxygen consumption (up to 100-600%) along with raised carbon dioxide (CO2) production; ventilation and cardiac output; adverse postoperative outcomes, such as wound infection; increased surgical bleeding; and morbid cardiac events. It causes arterial hypoxemia, lactic acidosis, increased intraocular pressure (IOP), increased intracranial pressure (ICP); and interferes with pulse rate, blood pressure (BP) and electrocardiographic (ECG) monitoring [6–8].
Shivering may happen as a response to hypothermia. This is one reason why patients’ body temperature should be kept within a normal range during surgery. However, shivering may also occur in normothermic patients. Moreover, adequate body warming is not always possible. In selected surgical patients, anesthesiologists may therefore wish to prevent shivering by using pharmacological strategies.
Among the pharmacological methods of controlling shivering, pethidine, gold standard for control of shivering, has been shown to be effective with a minimum effective dose of 0.35mg/kg [9]. Tramadol, a synthetic opioid agonist, prevents shivering by inhibiting the reuptake of norepinephrine and serotonin and activating the descending inhibitory spinal pathways. It also modulates the activity of nucleus median raphe acting centrally on the m opioid receptors predominately with minimum effects on k and d receptors. The antishivering effect of tramadol is mediated via serotonergic of noradrenertic receptor or both [10–12]. Tramadol in a dose of 1mg/kg iv has been shown to be effective in the treatment of postoperative shivering. Its pharmacodynamic advantage in causing less respiratory depression and sedation make it theoretically safer than pethidine. In our study we compared the anti shivering properties of Pethidine with Tramadol which is a synthetic opioid agonist.
With prophylaxis, many patients will receive a drug without actually needing it. These patients are unnecessarily exposed to adverse drug reactions [13]. We included only those patients who had shivering of grade 3 and above.
We designed our study to standardise the possible compounding factors while reflecting the common practice in our institution. The temperature in the operating room was maintained constant at 21°C to 23°C. IV fluids and drugs were given at room temperature. Axillary temperature was recorded at regular intervals intraoperatively.
In our study we observed that shivering disappeared by 1 minute in case of Tramadol and 5 minutes in case of Pethidine and in comparison to earlier study by Write et al., [14], shivering reduced significantly at one minute after Tramadol but the dose was 2 mg/kg.
The complete disappearance of shivering took 10 mi in Tramadol group and 20 min in Pethidine group in the study by Write et al., [14]. However, in our study the complete disappearance of shivering occurred by the end of seven minutes in case of Tramadol and 15 min in Pethidine. Earlier studies have showed better results with Tramadol group [10,15].
The incidence of recurrence of shivering was 50% in pethidine group while only in 10% in tramadol group in our study. The difference was statistically significant (p<0.05). The findings were in consolence with other studies by Write et al., [14] and Wrench et al., [16] which noted 8% with Tramadol group13 and 13-50% in Pethidine group. Thus various studies including ours there was higher rate of recurrence with Pethidine in comparison to Tramadol. The second dose of the drug controlled the shivering completely but the possibility of respiratory depression with Pethidine should be borne in mind. The probable reason for recurrence of shivering could be result of low plasma concentration of the active drug, when hypothermia is still persisting and individual variations in the core temperatures. Till date it is not clear whether higher shivering grades requires higher doses of the drug [9].
In our study both the drugs gave good and better haemodynamic stability throughout the course of the study in all the patients.
40% of cases from Pethidine group had nausea and vomiting which was easily treated with H2 receptor blocker and antiemetic drug. Earlier studies [4] have found that use of 1 mg/kg of Tramadol was associated with higher incidence of nausea and vomiting, and also sedation, which was not observed in our study. Some others [7] have suggested that slow injection of Tramadol over two minutes, reduces and prevents nausea and vomiting. In our study we injected 1% Tramadol and Pethidine I.V slowly in all the cases.
Conclusion
Our study results showed that the two groups were similar in regard to the hemodynamic responses. But, tramadol reduced the occurrence of postanaesthetic shivering more significantly than pethidine. In accordance with the previous studies, this study showed that tramadol is more effective for early control of shivering and its effect on recurrence of shivering is greater than pethidine. Also, Tramadol has less side effects like nausea and vomiting, respiratory depression compared to Pethidine. Tramadol cheaper and easily available (i.e. drug license is not required) as compared to Pethidine.
Hence our study concluded that anti-shivering effect of tramadol is early and more effective compared to pethidine. This study was in accordance with the previous studies indicating that tramadol can control the post anesthetic shivering effectively.