Congenital Porencephaly in a New Born Child
Suthar Pokhraj P.1, Patel Jigar J.2, Mehta Chetan3, Patel Narottam A.4
1 Resident Doctor, Department of Radiology, S.S.G. Hospital, Medical College, Vadodara, Gujarat, India.
2 Student, S.B.K.S. Medical Institute & Research Center, Suamandeep Vidhyapeeth University, At & Po Pipariya, Ta. Waghodia, Vadodara, Gujarat, India.
3 Associate Professor, Department of Radiology, S.S.G. Hospital, Medical College, Vadodara, Gujarat, India.
4 Professor, Department of Radiology, S.S.G. Hospital, Medical College, Vadodara, Gujarat, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Pokhraj Prakashchandra Suthar, 5-Durga Nagar Society, Karodiya , Baroda, Gujarat-391 310, India. Phone : +91-9662500537, +91-9825543039, E-mail : pokhraj_suthar@yahoo.co.in
A 2-day-old male child presented with history of enlarged head and seizures since birth, born by caesarean section. Head circumference was 56 cm (dilated) with widely open anterior and posterior fontanelle. Routine investigations were within normal limits. CT head revealed a large non-enhancing fluid attenuating cystic lesion in posterior parietal and occipital region with communicating to dilated bilateral lateral ventricles and subarachnoid space.
Central nervous system, Congenital, CT scan, Paediatric
Case Report
A 2-day-old male child presented with history of enlarged head and seizures since birth. He was born at 33 wk gestation with caesarean section for hydrocephalus. His mother did not take any antenatal care. No history of similar type of anomaly or tuberculosis in family, maternal teratogenic drug or radiation exposure. On Physical examination, fetal movements were reduced, head circumference was 56 cm (dilated), chest circumference 33 cm (normal), length 52 cm (normal). Anterior and posterior fontanelles were widely open with dilated visible veins.
Routine investigations like haemoglobin, total WBC, ESR, C-Reactive protein, blood sugar, serum creatinine, serum billirubin, Cerebrospinal fluid examination were within normal limit.
On ultrasonography of head, a large anechoic intracranial cystic lesion noted in parieto-occipital region which was communicated with lateral ventricle and subarachnoid space, bilateral lateral ventricles appeared dilated with hydrocephalus. Bilateral thalamus appeared normal.
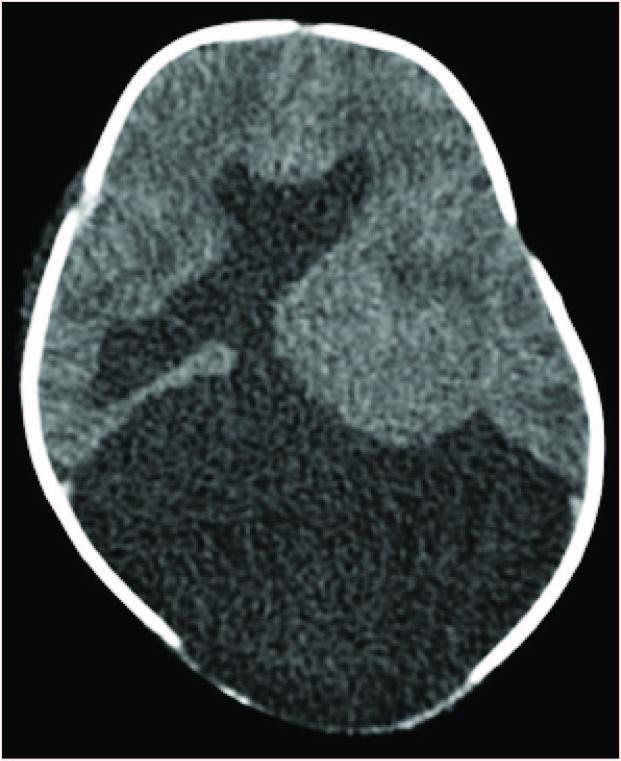
CT head showed a large well defined, hypo dense intracranial cystic lesion with attenuation value similar to CSF in bilateral posterior parietal and occipital regions. The lesion communicated with bilateral lateral ventricles and subarachnoid space. Bilateral lateral ventricles appeared dilated with thinning of over lying brain parenchyma. The lesion displaced the brain stem anteriorly and compressed cerebellum from superiorly. Widely open anterior and posterior fontanelle with small amount of brain parenchymal tissue seems to herniated from anterior fontanelle. Bilateral thalami appeared normal. On post contrast image cystic lesion was non enhancing without any solid component within. Provisional diagnosis of congenital porencephalic cyst was made. Then patient was referred to the higher center for further management [Table/Fig-1,2,3,4,5,6].
Axial Plain CT head shows large well defined, hypodense intracranial cystic lesion with attenuation value similar to CSF in bilateral posterior parietal and occipital regions. The lesion communicated with lateral ventricle and subarachnoid space. Widely open posterior fontanelle
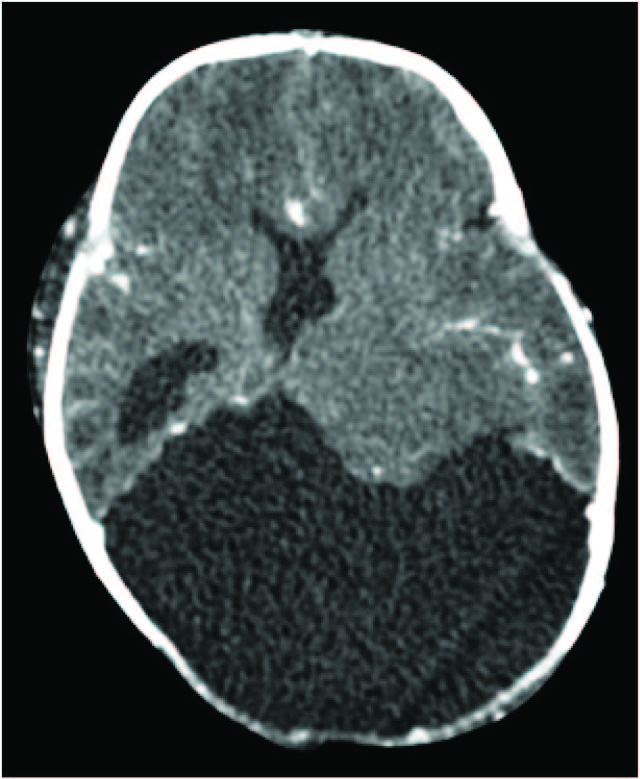
Axial Post Contrast CT head shows a large well defined non enhancing hypodense intracranial cystic lesion with attenuation value similar to CSF without any solid component within, in bilateral posterior parietal and occipital regions. Widely open posterior fontanelle
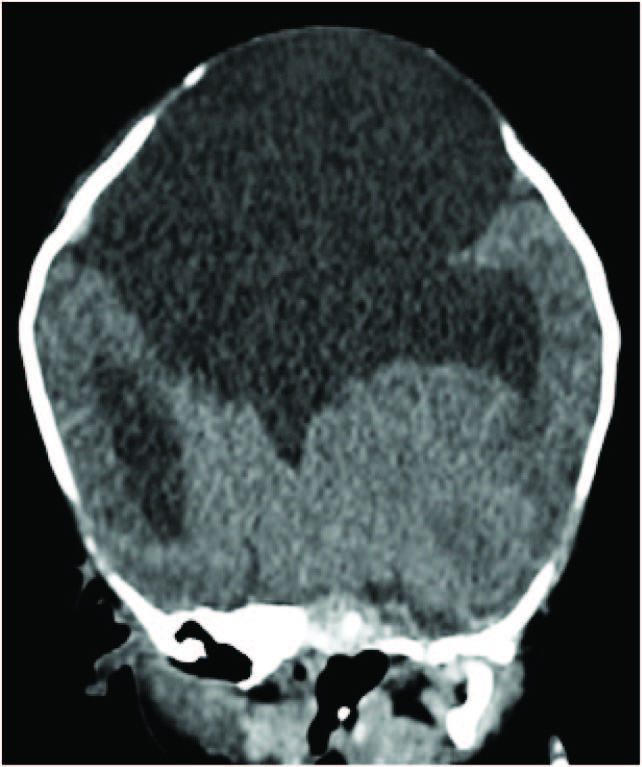
Coronal plain CT head shows a large well defined , hypodense intracranial cystic in bilateral posterior parietal and occipital regions with communicating to bilateral lateral ventricles and subarachnoid space
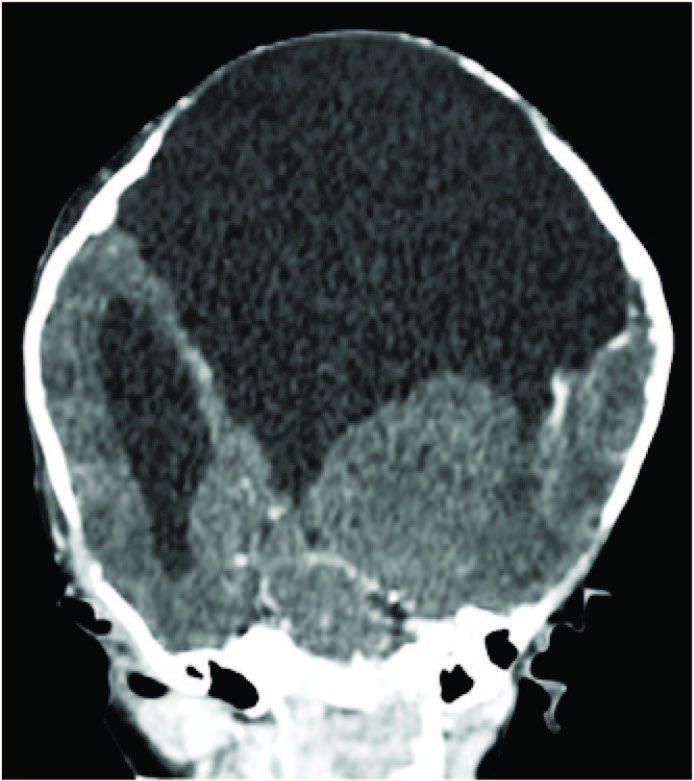
Coronal post contrast ct head shows a large well defined non enhancing, hypo dense intracranial cystic lesion with attenuation value similar to CSF in bilateral posterior parietal and occipital regions. The lesion communicated with bilateral lateral ventricles and subarachnoid space. Bilateral lateral ventricles appeared dilated with thinning of over lying brain parenchyma. Bilateral thalami appeared normal
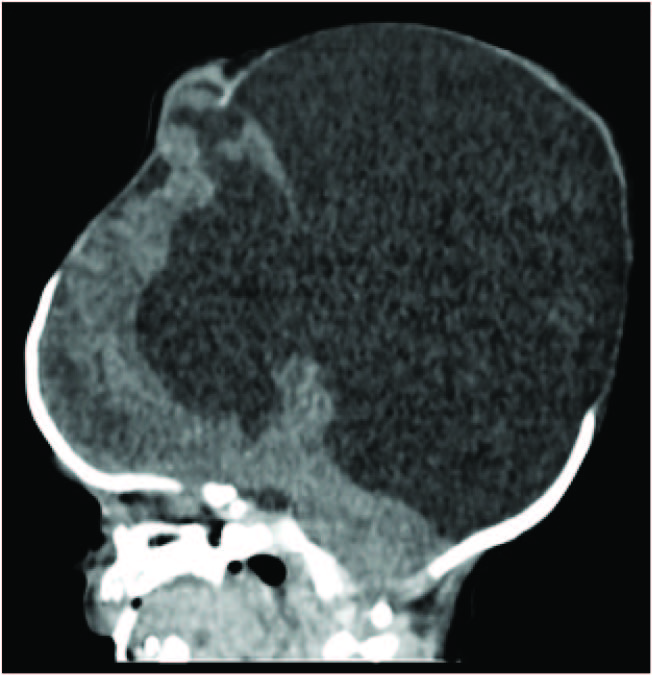
Sagittal Plain CT head shows a large cystic lesion in parietal and occipital regions with communication in lateral ventricle and subarachnoid space. Brain stem is displaced anteriorly and cerebellum is compressed from superiorly. Widely open anterior and posterior fontanelle with small amount of brain parenchyma tissue seems to herniate from anterior fontanelle
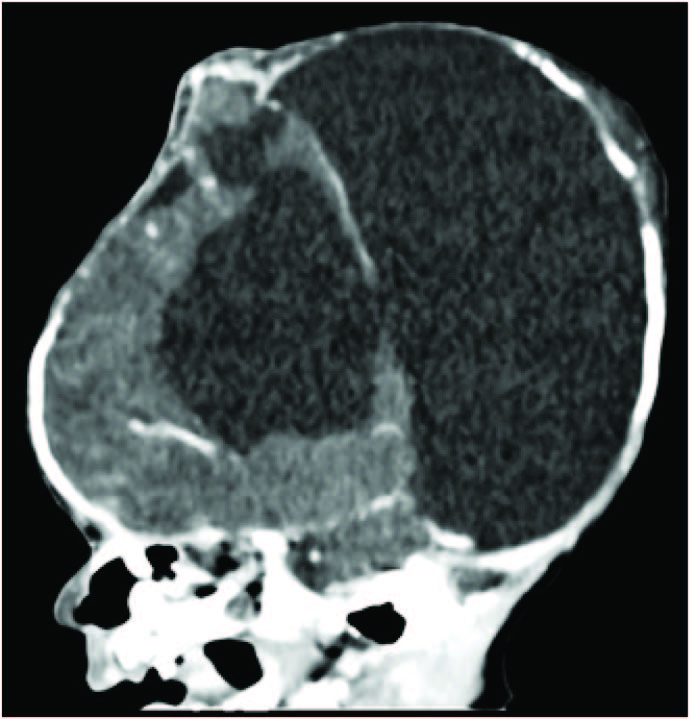
Sagittal post contrast CT head shows a large non enhancing hypo dense intracranial cystic lesion in posterior parietal and occipital region with communication in lateral ventricle and subarachnoid space. Widely open anterior and posterior fontanelle with small amount of brain parenchymal tissue seems to herniated from anterior fontanelle
Discussion
Porencephaly is an extremely rare congenital disorder of the central nervous system. It is a cavity filled with cerebrospinal fluid, in the brain’s parenchyma. It is caused by ischemia; haemorrhage after birth or less commonly as a consequence of abnormal development [1].
Porencephalic cysts can be located in any lobe. Involvement of bilateral hemisphere is very rare presentation. We report a case of bilateral porencephaly. Porencephaly encompasses a number of conditions, and can then be divided into developmental, congenital, internal and external types. If communicating with the ventricle then it is internal and communicating with the subarachnoid space then external type. It is lined by white matter. Gliosis will develop if the insult is as early as 20 wk of gestations [2].
Antenatal diagnosis by Ultrasonography is possible from the third trimester in case of congenital origin. Porencephalic cysts appear as a well defined intracranial cyst with attenuation similar to the CSF without solid component or post contrast enhancement. No mass effect on the adjacent parenchyma, although sometime the cysts are enlarged and result in local mass effect. Increased theta and delta bands in the areas surrounding the lesion sites seen on EEG [3].
Porencephalic cyst should be differentiated from the neuroglial cyst, archnoid cyst, interhemispheric cyst and holoprosencephaly. Neuroglial cyst is not communicating with the ventricles or sub-archnoid space. Arachnoid cyst is extra axial in location and underlying grey-white matter is normal. Holoprosencephaly is due to normal neuronal separation, where fused thalami and monoventricles seen.
The prognosis is very poor, most children dying within a few weeks or months.
[1]. Ho SS, Kuzniesky RI, Gilliam F, Faught E, Bebin M, Morawetz R, Congenital porencephaly:MR features and relationship to hippocampal sclerosisAJNR Am J Neuroradiol 1998 19(1):135-41. [Google Scholar]
[2]. Roessmann U, Gambetti P, Pathological reaction of astrocytes in perinatal brain injury. Immuno histochemical studyActa Neuropathol 1986 70(3-4):302-07. [Google Scholar]
[3]. Cerguidlini A, Seri S, Sturniolo MG, Galletti F, Computerized electroencephalographic assessment of congenital brain infarctionChilds Nerv Syst 1994 10:252-58. [Google Scholar]