Historically diseases of the oral cavity have been viewed separately from those of the rest of the body. In recent years however efforts have been made to recognize oral health as an integral part of overall health. Moreover, the oral cavity has a multitude of functions in relation to daily life such as food intake, speech, social contact and appearance. Poor oral health has thus the potential of hampering the quality of life. Decreased food intake because of oral pain or poor dental status can cause low growth in children and may worsen the nutritional status. Pain might also have a negative impact on the ability to engage in social relations and children might not get the full benefit of their education if suffering from pain and discomfort. While poor dental status among children has a negative effect on speech development, it may also have a socially stigmatizing effect in adolescents affecting social acceptance [1]. However there is no definite picture, yet regarding the disease status among children in rural and backward areas of country.
Gingivitis is inflammation of the soft tissue without apical migration of the junctional epithelium. Redness, oedema and bleeding on probing characterize this condition. When treated gingivitis is reversible with no permanent damage. Untreated cases may lead to a more complex and destructive entity known as chronic perioodontitis [2]. Periodontitis are the main cause of tooth loss. Bhayya et al., [3] reported prevalence of gingivitis 81% among school children. Dhar et al., [4] reported 84.37% prevalence of gingivitis among school going children of rural areas in Udaipur district.
The epidemiological study was planned as very few studies have been conducted in Bhopal district. Aim of this study was undertaken to find the prevalence of gingivitis among the school-going children of urban and rural areas of Bhopal district, India.
Materials and Methods
The present descriptive, cross-sectional study was conducted among 12 & 15 y old middle and high school government rural and urban school children of Bhopal district. It was conducted for a period of two months from 15th June to 15th Aug. 2013. A pilot survey comprising 110 school children was done to assess the feasibility of the study, and to assess the prevalence of oral diseases to calculate the sample size. One school was selected randomly and the students who were present on that day were examined. Pilot study assessment was utilized for proper planning and execution of the main study and also to check the survey form to be used for collection of data.
A sample size of 1100 (538 Males & 562 Females) were examined. For the selection of schools, a three- stage sampling procedure was adopted. During first stage, stratification of urban and rural areas of Bhopal district was done. Then, in second stage total numbers of school in Bhopal district were listed out. During the third stage, students were selected from each class by simple random technique using the student’s attendance register till the desired sample from each class was met. The investigator was trained in the Department of Public health Dentistry, People’s college of Dental sciences & Research Centre. Ethical clearance was obtained from institutional ethical committee of People’s college of dental sciences and Research Centre. Written permission was obtained from the district Educational Officer. Written approvals were also obtained from school authorities before scheduling the survey. Informed consent was obtained from the participating school children before carrying out the survey procedures. Information on demographic details and oral hygiene practices was collected from the participants with the help of pretested questionnaire. The questionnaire consisted of two parts. Part one comprised of demographic details and questions covering the oral hygiene practices of children with regard to frequency, type and material used for cleaning, part two comprised of clinical examination using gingival index.
Single trained examiner, examined all the school children, who was trained to record the WHO (modified) oral health assessment form to avoid inter-examiner variations. Loe and Silness index was used for recording gingival status [5]. The scoring criteria of Loe-Silness gingival index is 0 for Absence of inflammation/ normal gingival, 1 for Mild inflammation, slight change in color,slight edema, no bleeding on probing for Moderate inflammation, moderate redness, edema, bleeding on probing, hypertrophy for severe inflammation: marked redness and hypertrophy, ulceration, tendency to spontaneous bleeding [5].
SPSS version 20 (SPSS Pty Ltd, Chicago, IL, USA) was used for the statistical analysis. The chi-square test used for categorical data. p<0.05 was considered statistically significant.
Results
Among 1100 children examined 217 (40.2%) males and 323 (59.8%) females were from urban schools; 321 (57.3%) males and 239 (42.7%) females were from rural schools respectively [Table/Fig-1].
Distribution of study subjects according to gender and location
| Gender | Location |
|---|
| Urban | Rural | Total |
|---|
| Subjects (%) | Subjects (%) | Subjects (%) |
|---|
| Male | 217 (40.2%) | 321 (57.3%) | 538 (48.9%) |
| Female | 323 (59.8%) | 239 (42.7%) | 562 (51.1%) |
| Total | 540 (100%) | 560 (100%) | 1100 (100%) |
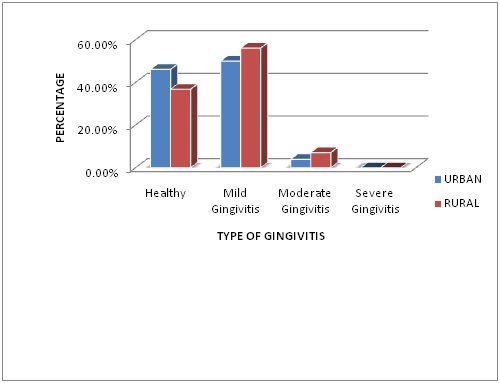
Out of 1100 children examined 455 (41.36%) had normal gingiva, prevalence of gingivitis was 59% found. 584 (53.09 % ) children had mild gingivitis,61(5.54%) had moderate gingivitis. When urban and rural school children were compared for gingivitis it was found that In Urban schools 249(46.11%) children had normal gingival,270(50.0%)had mild gingivitis, 21(3.88%) had moderate gingivitis. In Rural schools 206 (36.78%) children had normal gingival,314 (56.07%) had mild gingivitis,40(7.14%) had moderate gingivitis [Table/Fig-2].
distribution of study subjects according to type of gingivitis and location
332 (62%) male and 311(55.3%) female had gingivitis. Prevalence of gingivitis in urban schools was 54%, and in rural school children it was 63.2%. Healthy scores decreased with the age and were more among males.
Mild and moderate gingivitis were found higher in 15 y age group 295(50.5%) and 32 (52.5%) respectively, when compared with 12 y of age group [Table/Fig-3]. Twice daily brushing was significantly associated with healthy gingival (p = 0.001) in the both age groups [Table/Fig-4].
Relation between age group and gingivitis
| Age Group | Healthy | Mild Gingivitis | Moderate Gingivitis | CHI-Sq. | p-value |
|---|
| 12 year | 232 (51.0%) | 289 (49.5%) | 550 (47.5%) | 0.387 | 0.824 |
| 15 year | 223 (49.0%) | 295 (50.5%) | 32 (52.5%) |
| Total | 455 | 584 | 61 |
Relation between frequency of brushing and gingivitis
| Type of Gingivitis | Once Daily | Twice Daily | Occasionally | CHI-Sq. | p-value |
|---|
| Healthy | 337(74.1%) | 115(25.3%) | 3(0.7%) | 38.31 | p=0.001 (p<0.05) |
| Mild Gingivitis | 473(81.0%) | 110(18.8%) | 1(0.2%) |
| Moderate Gingivitis | 47(77.0%) | 235(16.4%) | (86.6%) |
| Total | 857 | 235 | 8 |
Discussion
Oral health is essential for general health and well-being throughout life and is a marker for overall health status. The present study was targeted at school going children because of the ease of accessibility.
At both the age groups, around 96% of population used tooth brush and toothpaste or toothpowder for cleaning their teeth. This clearly indicates their awareness about oral hygiene. 3.8 % children clean their teeth with their finger and 0.35% children use neem sticks, which is the traditional method of cleaning the teeth in India, the custom of cleaning teeth with finger and neem sticks is still followed in certain parts of rural India. Nevertheless the percentile usage of their traditional methods is decreasing [6]. From this finding it is evident that a better usage of oral hygiene aids was found in schoolchildren of Bhopal district.
Most of them (78%) used to brush once a day which is in line with the findings of shailee et al., [7] but high as compared with findings of Harikiran and Pallavi [8] and Peng et al., [9], where as only 21.3% of student brushed twice daily which is low. The fact that all the children examined belong to government school and most of them come from illiterate-low socio-economic families is responsible for this finding. The frequency of brushing twice was more common in urban schools as compared with rural schools which were also reported by Kumar et al., [10], in the present study, as the frequency of brushing increased prevalence of gingivitis decreased. The reason being obvious, that there is significant co-relation between plaque retention and gingival inflammation [11].
In the present study the prevalence of gingivitis among schoolchildren was 59%,It is less when compared to results reported by Dhar et al., [4], who did the study on school going children of rural areas of India have reported 84.3% overall prevalence which is high. Whereas 100% prevalence was seen in the reports of Mathur et al., [12], which is very high when compared to our findings. This study was conducted in early 90’s & this might be the reason behind the high prevalence of gingivitis while recent literature is suggestive of possible trend of lower prevalence rates [13]. This might be attributed to the better oral hygiene awareness among the children. When the gender wise prevalence of gingivitis was considered, boys were affected more than girls, this may be due to improper oral hygiene practices in boys .similar findings were seen in a study conducted by Das et al., [14]. Sutcliff survey shows high prevalence among females [15].
As the present study showed that about 96% used tooth brush, but the gingivitis present in most of the school children reflects irregular brushing methods which can be due to inadequate brushing time, ineffective brushing technique, or both factors, or it may also be possible that some of the children did not brush as they claim.
The frequency of regular dental check up and dental service utilization followed was very poor. This could be due to knowledge, attitude and Socio-economic status of the parents indicating the need for school oral health education program and to build a comprehensive preventive care.
In epidemiological survey it is difficult to differentiate puberty gingivitis. this could be the one of the limitation of this study.
As to improve the oral health of children in Bhopal district, the following recommendations are given:
Oral health promotion through well-structured oral health education program can create positive change in awareness for special groups like school children
Reinforcement of knowledge is necessary which can be done by incorporating chapters on oral health and oral hygiene in school textbooks. Also, the teachers training programs can ensure continuity of reinforcement
Implementation of school dental health programs focusing on preventive programs like fluoride mouth rinse and tooth brushing programs
Preventive services should be given high priority and needs to be started at an early age to target the primary dentition and future caries in permanent dentition
Regular interval screening programs to assess the oral health and treatment needs of school children and provision of treatment as per the need [7].
Conclusion
Early gingivitis if unattended may slowly lead to periodontitis which can have more detrimental effects such as early tooth loss. More often than not the painless nature of gingivitis masks its true potential and become the reason of not visiting the dentist. Furthermore, parents and school children require awareness and proper education regarding gingivitis and its future effects and its prevention via proper oral hygiene means. Suitable oral health program using audio visual aid should be conducted regularly for the children to educate them which might prove to be a significant factor in reducing the prevalence of gingivitis in future.