Most of the tibial plateau fractures are associated with significant soft tissue injuries. Injury to the surrounding soft tissue envelope increases the risks for complications and must be considered when managing tibial plateau fractures [1–6]. Ilizarov fixation has a special advantage over other modalities of treatment in managing such fractures. Most data indicate that external fixation is equally as effective as or more so than plate fixation or any other form of internal fixation [7–9]. Aim of our study was to evaluate various of tibial condyle fractures treated by Ilizarov fixation.
Materials and Methods
This study was undertaken in patients who were operated between July 2006 to Jun 2013 at MS Ramaiah Teaching Hospital, which is a tertiary hospital in Bangalore. Study included 43 patients with Schatzker type II and above tibial plateau fractures treated by ilizarov fixation. All 43 patients were treated in M S Ramaiah teaching hospital by Ilizarov and limb reconstruction unit. Informed consent was taken from all the patients.
Inclusion Criteria
Age: >20 y
Sex: Both sexes
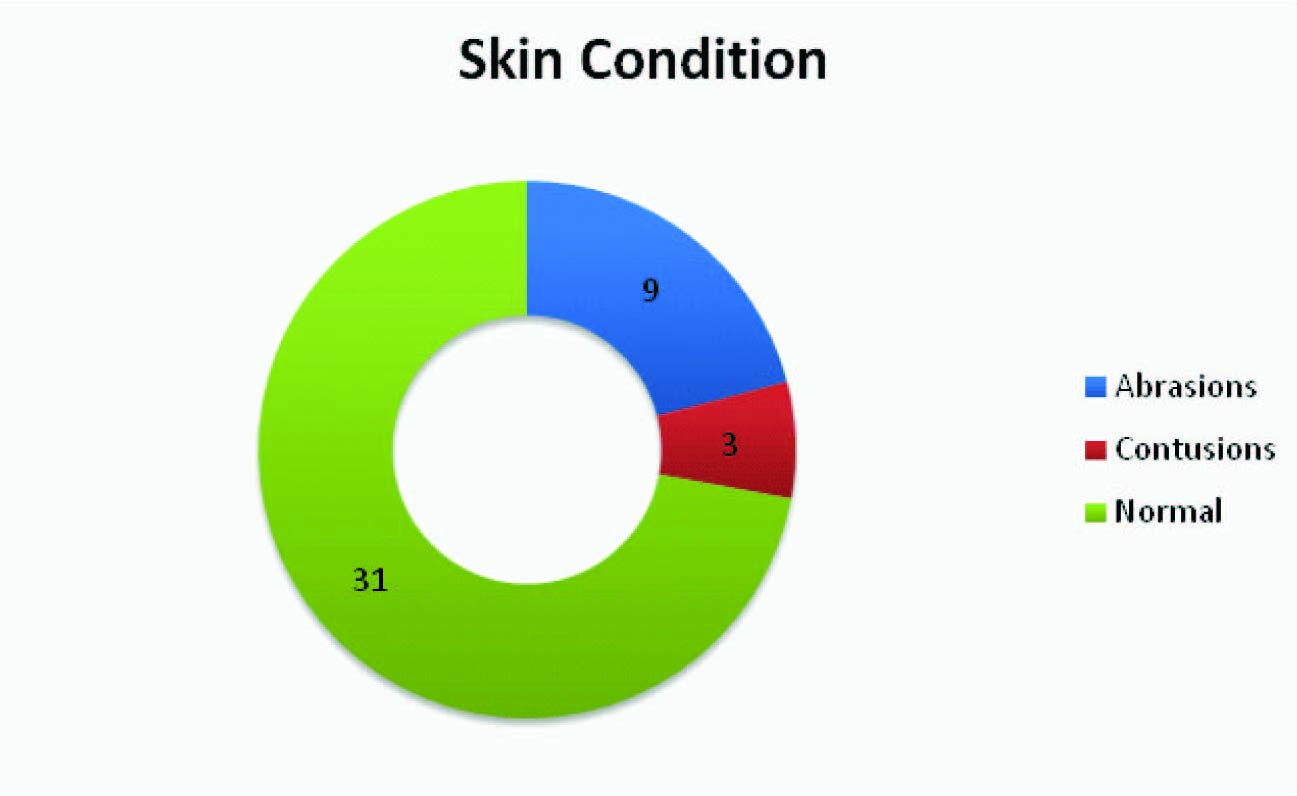
Closed tibia plateau fracture with skin abrasion and contution
Severly comminuted fractures of the tibial plateau treated by ilizarov external fixator.
Exclusion Criteria
Associated ipsilateral femur fractures
Pathological fractures of tibia
Patients lost for follow up.
Standard trauma evaluation, a meticulous musculoskeletal and neurologic examination was carried out in all patients. Detailed radiographic assessment and preoperative templating was done for each case. CT scan with 3D reconstruction was done for most of severe type injuries for better understanding of fracture geometry. The time period between the trauma and the surgery varied from 8 h to 12 d with an average of 7 day. Majority of cases were operated under regional anaesthesia. The frame was prepared based on the preoperative templating. All the patients were put on fracture table except few where elevation of the depressed fragment and bone grafting was necessary. On fracture table indirect reduction was achieved by ligamentotaxis and was confirmed on fluoroscopy. By maintaining reduction Ilizarov wires passed from proximal to distal. Patients were followed up at 6 wk, 3 mnth,6 mnth and 1 y. With each visit clinical, radiological and functional evaluation of these patients were done.
Results
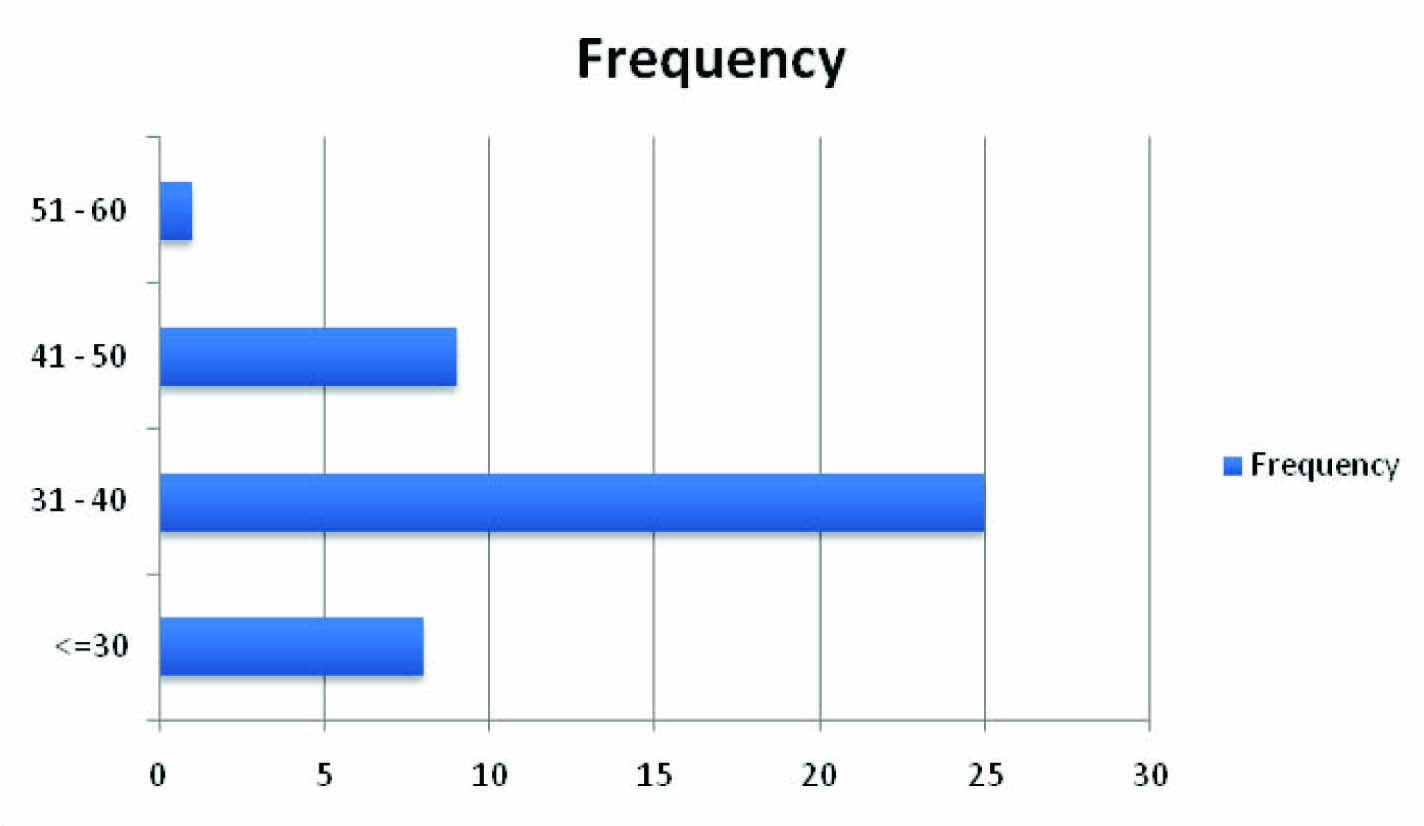
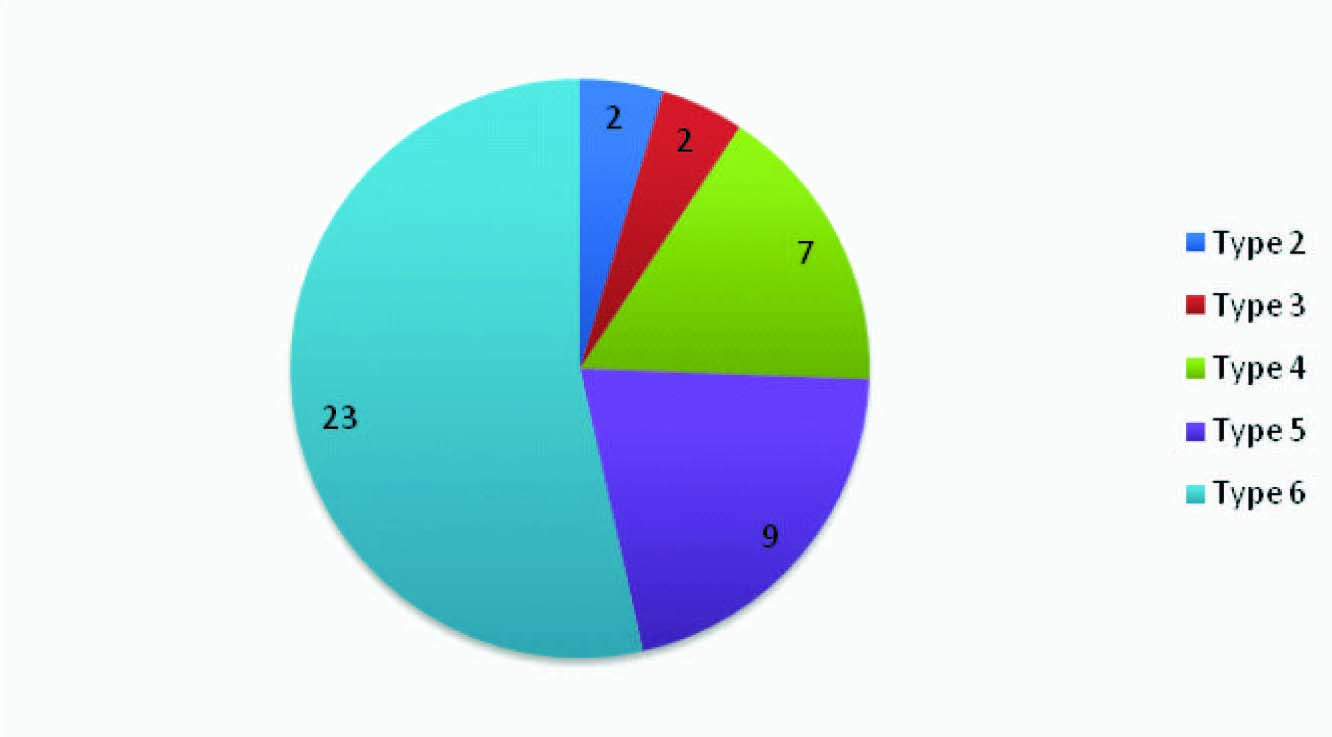
A total 43 cases of tibial plateau fractures, which full filled our inclusion criteria were part of our study. The observations and the results of the study are shown in tables and graphs as follows [Table/Fig-1,2,3,4,5,6,7,8].
| SEX | Frequency | % |
|---|
| F | 4 | 9.3% |
| M | 39 | 90.7% |
| Total | 43 | 100% |
Skin conditon overlying the fracture
| Sl No | Complication | Number of cases |
|---|
| 1 | Varus Malunion | 2/43 |
| 2 | Osteomyelitis | 2/43 |
| 3 | Extensor lag | 5/43 |
| 4 | Foot drop | 1/43 |
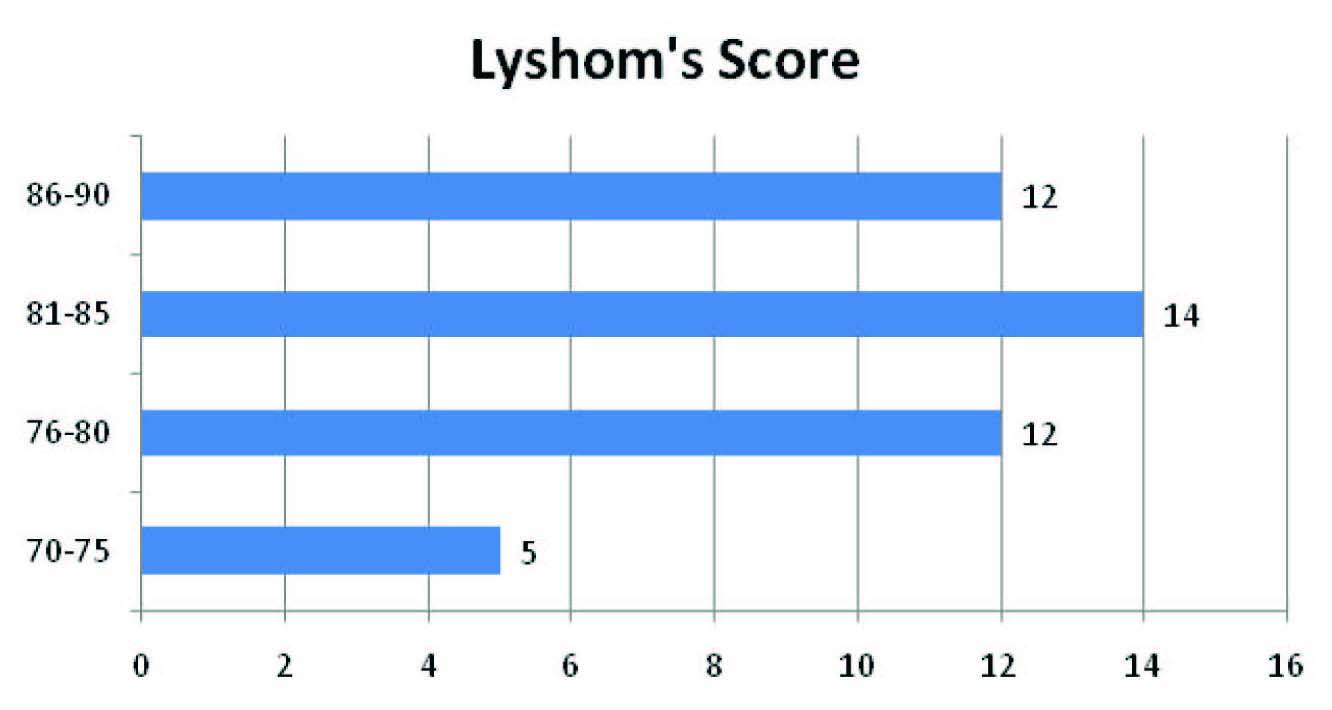
Lyshom’s score at the end of one year
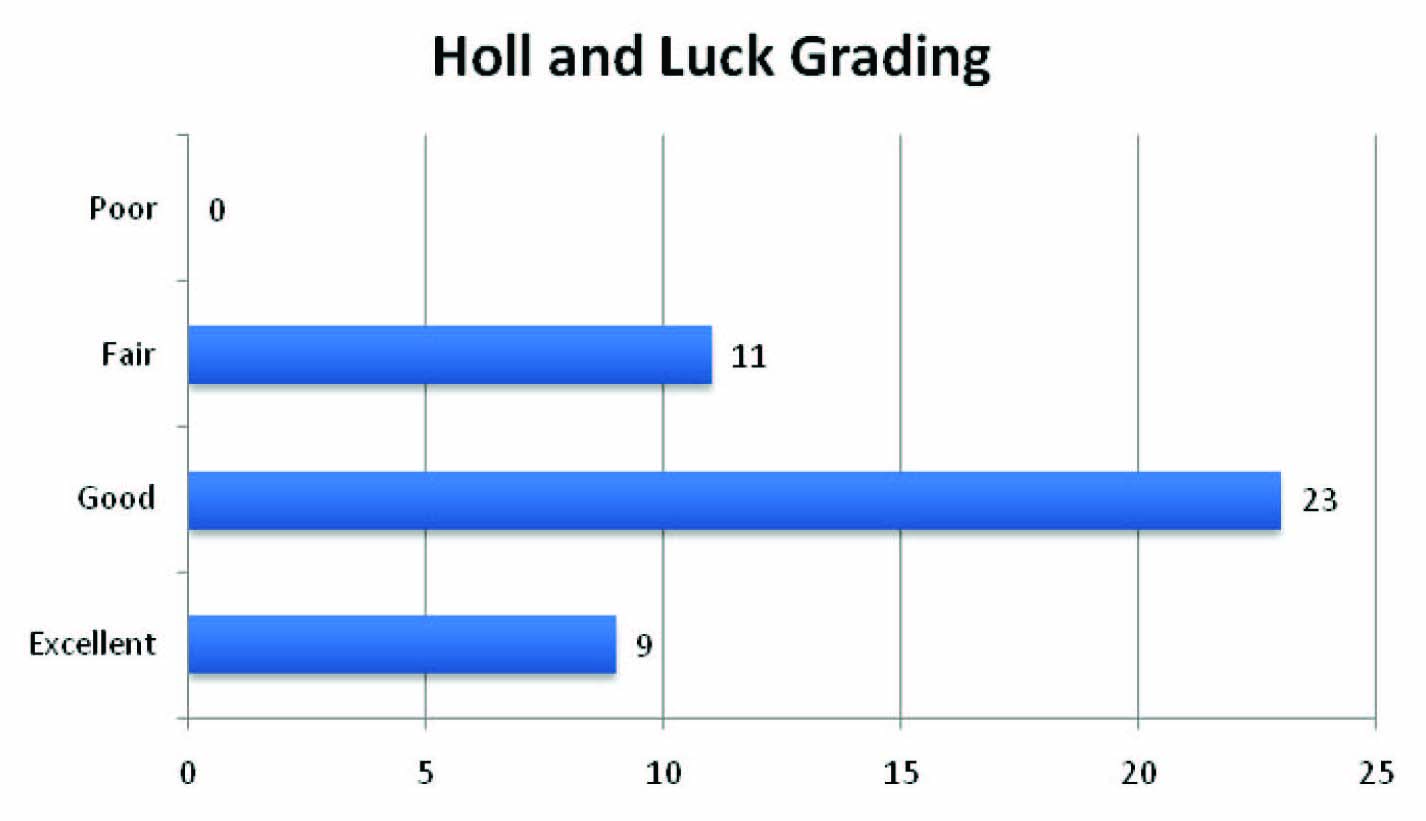
Holl and Luck Score at the end of one year
Radiological union in week
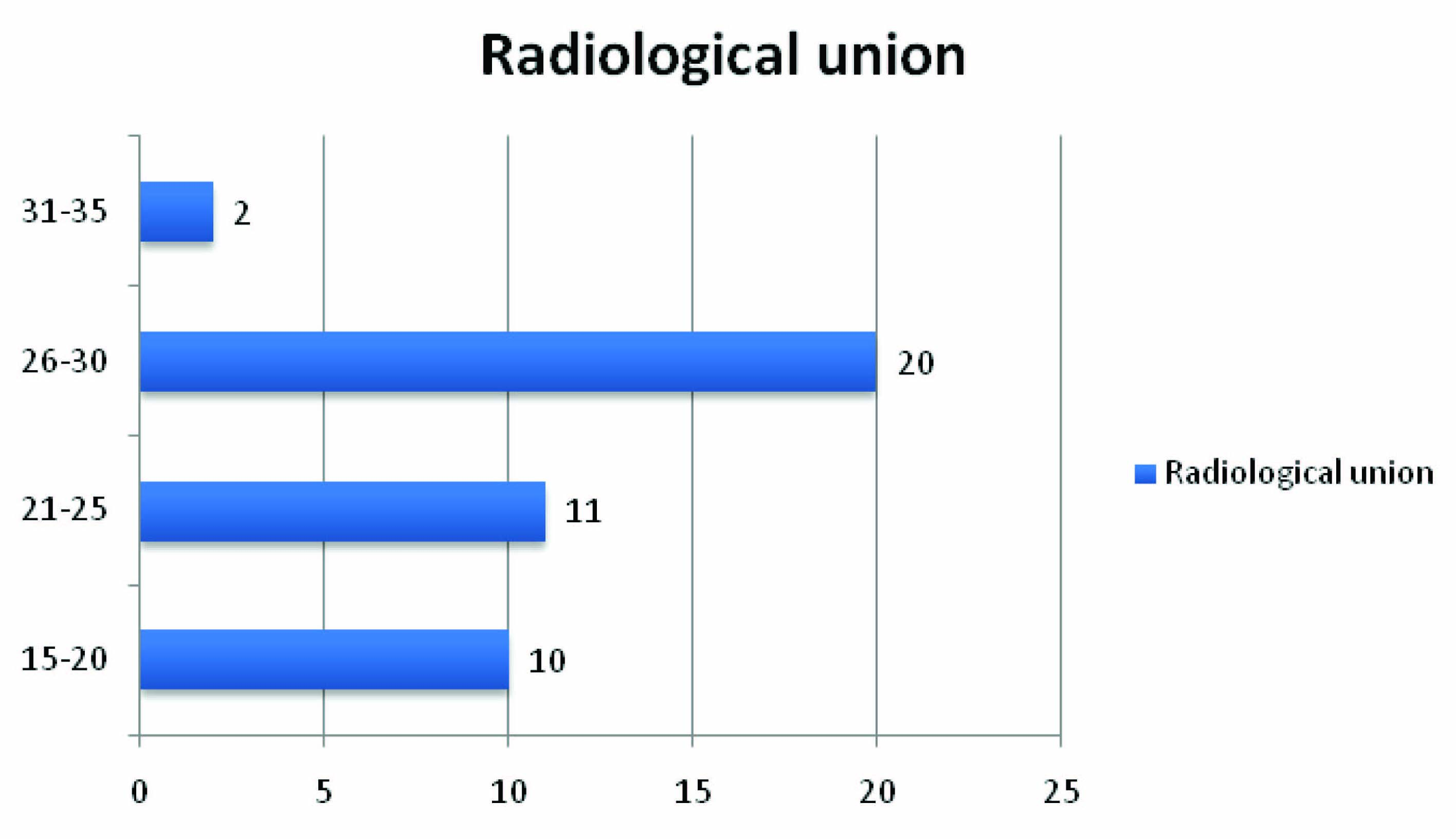
Our study included 43 cases of tibial plateau of various types except type I. All the fractures were treated in a same team of surgeons. In our study of 43 cases all the cases underwent union. Mean time for radiological union was 24.51 wk (range 15 to 32 wk) [Table/Fig-8]. Mean fixator period was 26.6 wk (16-34 wk). The Ilizarov fixator was removed approximately two wk after radiological union. The functional results were measured by Lyshom’s and Hohl and Luck score. The mean Lyshom’s score was at the end of one year was 82.16. At end of one year by Hohl and Luck grading 11 patients had fair, 23 had good and 9 had excellent results. None of our patients had poor scores [Table/Fig-6,7].
Pin site infection was the most common complications seen in our study. Thirty five patients had pin site infection but only in two cases it required change of pins. The other complications were varus malunion, extensor lag, osteomyelitis and foot drop [Table/Fig-5].
Discussion
Periarticular fractures are challenging to treat and tibial plateau fractures are no exception. The principles and techniques have dramatically evolved over few decades. Tibial fractures range from low energy injuries in osteoporosis to high energy trauma with severe soft tissue injury [1–5]. The goal of treatment these fractures are to achieve union and prevent complications. Various modalities of treatment have been described for treatment of these fractures which include traction, splitting, internal fixation and external fixation. Traction and casting provides poor union rate and high complications like knee stiffness. Open reduction and internal fixation in high velocity injuries carries risk of infection and wound complications [6–9].
Soft tissue injury is the most common association with these fractures. The soft tissue injury is worse with bicondylar fractures, fracture-dislocations and metaphysio-diaphyseal dissociation. Internal fixation with plating in such injuries carries significant complications like infection, wound and hardware problems. The use of external fixation in treatment of such fractures has dramatically improved results. Closed reduction using ligamentotaxis or limited open reduction followed by Ilizarov fixator application avoids additional soft tissue injury and devitalisation of bone. Recent studies indicate that Ilizarov fixation has similar or better results and fewer complications compared with plating. Ilizarov fixation can be done early compared to internal fixation.Chances of achieving accurate reduction and ligamentotaxis more when surgery is performed early.
Review of literature shows many studies of Ilizarov fixation in the treatment of tibial plateau fractures with variable results [10–15]. Study of Ilizarov fixation in the treatment of various authors and their conclusion is summarized in [Table/Fig-9].
Various studies of Ilizarov fixation in treatment of Tibial plateau fractures
| Authors | Year | No of patients | Conclusion |
|---|
| Marsh J L et al., [10] | 1995 | 21 | External fixation has good results and low complications |
| George K Dendrinos et al., [11] | 1996 | 24 | Ilizarov circular fixation is an ideal method of treatment for these fractures when extensive dissection |
| Whatson J Tracy et al., [12] | 1998 | 14 | Ilizarov fixation shows excellent results without severe soft tissue complications |
| Barbary H. El et al.,[13] | 2005 | 29 | Ilizarow has clinical success and low morbidity |
| Ranatunga IR et al., [14] | 2010 | 18 | Ilizarov is a good and viable option in the management of tibial plateau fractures |
| Mohammad OA et al., [15] | 2013 | 30 | Good results and low morbidity |
| Ours Study | 2014 | 43 | Ilizarov fixation is the definitive treatment of tibial plateau fractures , with good union rates and less complications |
The advantage of Ilizarov over internal fixation is that it allows closed reduction, minimal soft tissue damage and early mobilization of the joint. In presence of severe soft tissue swelling, blisters or open fractures Ilizarov fixation is not a contraindication [10,15]. Ilizarov fixator removal is a minor procedure unlike plate removal can be done under sedation on an outpatient basis.
Conclusion
High energy tibial plateau fractures can be definitively treated with Ilizarov external fixation. Treatment with this method gives good union rates and less risk of infection. Closed reduction, minimal soft tissue damage and early mobilization are the key to low complications.