Unusual Infra-Clavicular Venous Circle – A Case Report
Satheesha Nayak B1, Srinivasa Rao Sirasanagandla2, Ashwini Aithal P3, Anitha Guru4, Sudarshan S5
1 Professor and Head, Department of Anatomy, Melaka Manipal Medical College (Manipal Campus), Manipal University, Madhav Nagar, Manipal, Karnataka, India.
2 Lecturer, Department of Anatomy, Melaka Manipal Medical College (Manipal Campus), Manipal University, Madhav Nagar, Manipal, Karnataka, India.
3 Lecturer, Department of Anatomy, Melaka Manipal Medical College (Manipal Campus), Manipal University, Madhav Nagar, Manipal, Karnataka, India.
4 Lecturer, Department of Anatomy, Melaka Manipal Medical College (Manipal Campus), Manipal University, Madhav Nagar, Manipal, Karnataka, India.
5 Associate Professor, Department of Anatomy, Melaka Manipal Medical College (Manipal Campus), Manipal University, Madhav Nagar, Manipal, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Srinivasa Rao Sirasanagandla, Lecturer, Department of Anatomy, Melaka Manipal Medical College (Manipal Campus), Manipal University, Madhav Nagar, Manipal, Karnataka-576104, India. Phone : 9886310652, E-mail : seenaih.anat@gmail.com
Currently, numerous invasive procedures are preferred in cephalic vein (CV) and axillary vein (AV) than other veins in the neck. Anatomical variations of these veins in the axilla and delto-pectoral region may result in failure and postoperative complications of the procedures. A thorough knowledge of possible variations of AV and CV may immensely contribute to the success of any such procedures where the veins are involved. We report the variations of the CV, tributaries of AV and median cubital vein. We observed a venous circle formed by the tributaries of AV in the infra-clavicular region, deep to the pectoral muscles. Cephalic vein joined proximal end of venous circle just before ending into AV. Further, duplication of the median cubital vein was observed.
Axillary vein, Cephalic vein, Infraclavicular, Median cubital vein
Case Report
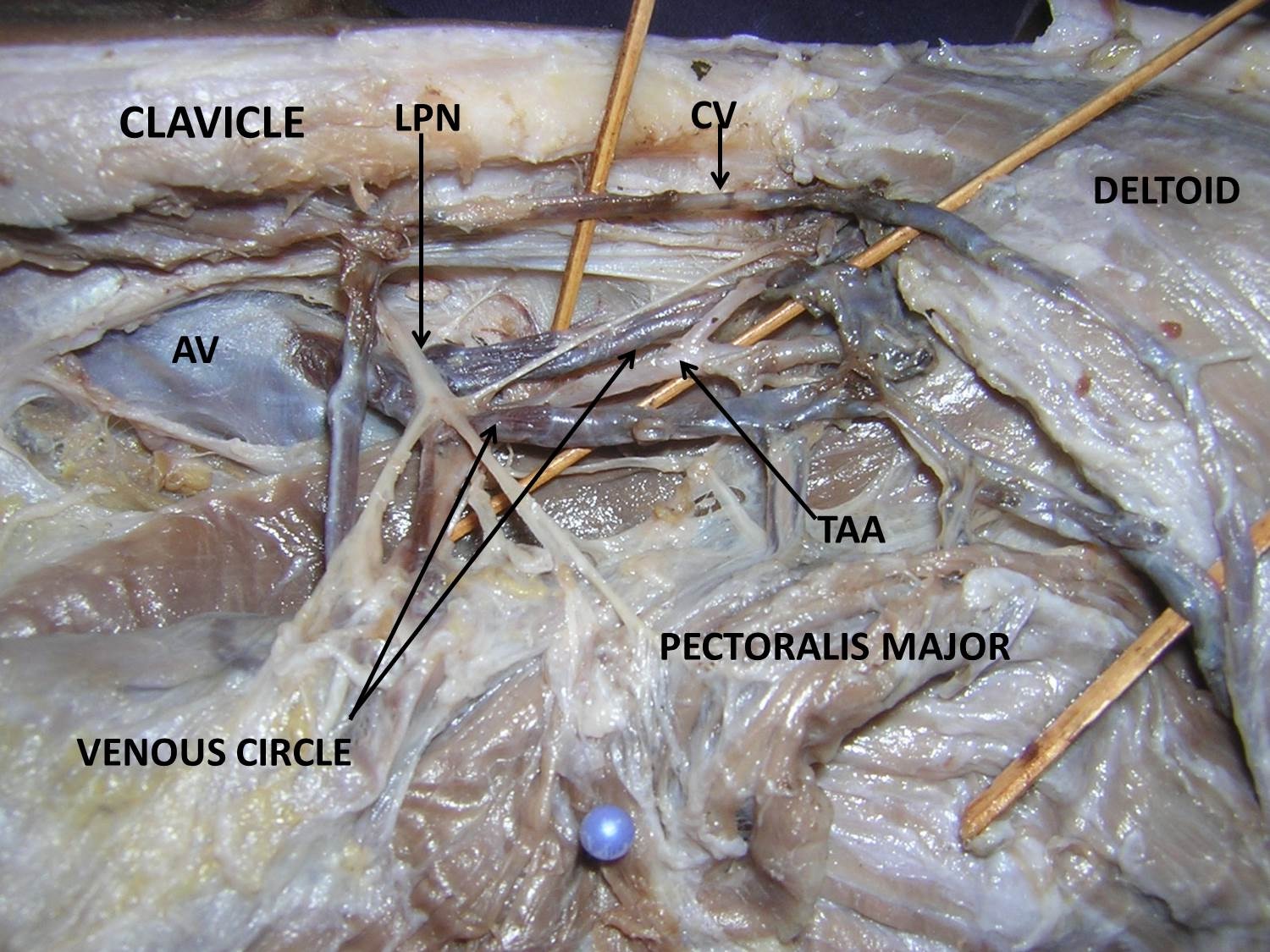
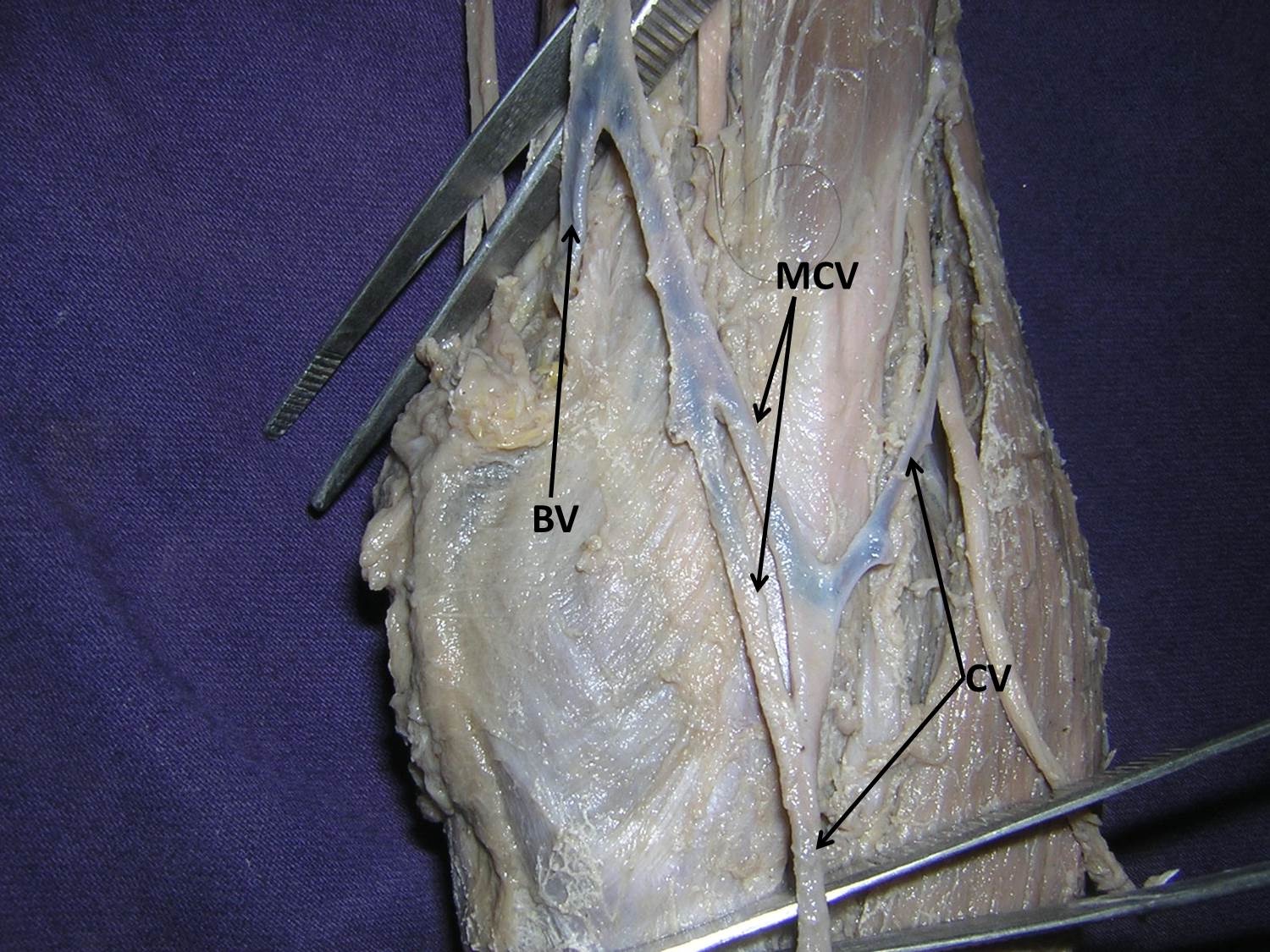
During the dissection of the left upper limb of an adult male cadaver, we found anatomical variations of CV, AV and median cubital vein. After reflection of the pectoralis major muscle, we could see a venous circle formed by the union of tributaries of AV. This venous circle was sufficiently large and received venous blood from the adjacent muscles. The proximal end of the circle received the CV and immediately terminated into the AV [Table/Fig-1]. Pectoral branch of thoraco-acromial artery passed through the venous circle. Further, there were two median cubital veins of considerable size. These two veins joined to form a single vein, which ultimately drained into the basilic vein [Table/Fig-2].
Dissection of the left subclavicular region showing the venous circle formed by the tributaries of the axillary vein (AV). The pectoralis major muscle has been reflected. Cephalic vein (CV) and thoracoacromial artery (TAA) are also seen. (LPN: lateral pectoral nerve)
Superficial dissection of cubital fossa region of left upper limb. Duplication of the median cubital vein (MCV), cephalic vein (CV) and the basilic vein (BV) are seen
Discussion
In the present case, tributaries of AV were found forming venous circle deep to the pectoral muscles, in the infra-clavicular region. In our literature search, we did not find reporting of such venous circle in the axilla. Knowledge of occurrence of such venous channel, anterior to the axillary vein is clinically important. In conventional Patey’s mastectomy procedure, axillary lymph nodes are usually accessed through the axillary base. To minimize the damage to the pectoral muscles in this procedure, recently transpectoral anterior route has been attempted to remove the axillary lymph nodes [1]. Lack of prior knowledge about the anatomic variants of veins may alarm unnecessary bleeding during transpectoral anterior entrance to axilla. AV is targeted for various invasive procedures such as central venous access in patients with severe burns [2] and defibrillator implantation in heart failure patients [3]. Further, AV identification is a crucial step in successful removal of axillary lymph nodes, in mastectomy [4]. Knowledge of anatomic variations involving the tributaries of AV plays an important role in successful approach of AV.
CV frequently shows variations in its course and termination. Unusual drainage of CV into basilic vein, internal jugular vein, subclavian vein and external jugular vein has been reported [5–8]. Due to constant position and sufficiently large size, CV is frequently used for intravenous drug administration [9]. Studies have shown that percutaneous venous punctures are preferred in CV than subclavian vein [10]. CV is used for the central venous access, and its usage has been shown to give better results than subclavian vein [11]. Appropriate size and thickness of wall as well as ease of handling properties have enabled CV suitable for carotid patching than long saphenous vein [12]. As clinical importance of CV is gaining increasing significance, reporting of its possible anatomical variants may be important to perform the above said invasive procedures with minimum complications. Introduction of the cannula into the variant CV may result in unnecessary complications. In the present case, the CV terminated into the proximal end of venous circle formed by the tributaries of AV. Direction of termination of CV into the proximal end of venous circle may lead to complications in the cannulation procedures.
In majority of cases (84 %), median cubital vein arises from the CV. But less frequently (16 %), median cubital vein arises from the basilic vein and terminates into CV [13]. In the present case, median cubital vein was duplicated. Since CV is frequently used for intravenous injections, blood collection and transfusion and also for cardiac catheters introduction [14], knowledge of its possible variations is quite important.
Conclusion
Anatomic variants of CV, tributaries of AV and median cubital vein reported in the present case are clinically important to avoid iatrogenic injuries and postoperative complications in surgical procedures of axilla as well of invasive procedures involving these veins.
[1]. Dasgupta S, Sanyal S, Sengupta SP, Transpectoral anterior approach to the axilla for lymph node dissection in association with mastectomy preserving both pectoral muscles and their neurovascular bundlesTumori 1999 85(6):498-502. [Google Scholar]
[2]. Andel H, Rab M, Felfernig M, Andel D, Koller R, Kamolz LP, The axillary vein central venous catheter in severely burned patientsBurns 1999 25:753-56. [Google Scholar]
[3]. Ramza BM, Rosenthal L, Hui R, Nsah E, Savader S, Lawrence JH, Safety and effectiveness of placement of pacemaker and defibrillator leads in the axillary vein guided by contrast venographyAm J Cardiol 1997 80:892-96. [Google Scholar]
[4]. Ung O, Tan M, Chua B, Barraclough B, Complete axillary dissection: A technique that still has relevance in contemporary management of breast cancerANZ J Surg 2006 76:518-21. [Google Scholar]
[5]. Ishizuka H, On variations in the mode of outlet of the cephalic veinYokohama Med Bull 1964 15:79-89. [Google Scholar]
[6]. Bergman RA, Afifi Ak, Miyauchi R. Upper Limb. Illustrated Encyclopedia of Human Anatomic Variation: Opus II: Cardiovascular System: Veins. http://:www.anatomyatlases.Org/ana-tomicVariantiant/ Anatomy HP. shtml. (accessed April 2009) [Google Scholar]
[7]. Saaid A, Drysdale I, Unusual termination of the cephalic veinClin Anat 2008 21:786-87. [Google Scholar]
[8]. Lau EW, Liew R, Harris S, An unusual case of the cephalic vein with a supraclavicular coursePacing Clin Electrophysiol 2007 30:719-20. [Google Scholar]
[9]. Vialle R, Pietin-Vialle C, Cronier P, Brillu C, Villapadierna F, Mercier P, Anatomic relations between the cephalic vein and the sensory branches of the radial nerve: How can nerve lesions during vein puncture be prevented?Anesth Analg 2001 93:1058-61. [Google Scholar]
[10]. Mathes SJ, Nahai F, Reconstructive surgery, principles, anatomy and technique 1997 Vol. 1PhiladelphiaSection 8F Radial Forearm, Churchill Livingstone:775-802. [Google Scholar]
[11]. Povoski SP, A prospective analysis of the cephalic vein cutdown approach for chronic indwelling central venous access in 100 consecutive cancer patientsAnn Surg Oncol 2000 7:496-502. [Google Scholar]
[12]. Khan RSA, Simms M, Cephalic vein for carotid patchingEJVES Extra 2005 9:35-36. [Google Scholar]
[13]. Bergman R, Thompson SA, Afifi AK, Compendium of Human Anatomic Variation 1988 Baltimore, MDUrban and Schwarzenberg, Inc:90-91. [Google Scholar]
[14]. Kyle J, Pye’s Surgical Handicraft 1977 20th ednBristolJohn Wright and Sons Ltd [Google Scholar]