Humans emit a variety of volatile and non- volatile molecules from their oral cavities which impart it a characteristic odor [1]. If unpleasant, disagreeable or disturbing, it is called as halitosis/ bad breath/ oral malodor [2–4]. It is believed to affect one quarter of the population around the world [5–7]. Studies have reported an incidence as high as 50% with varying degree of intensity [8,9]. The causes include gingivitis, periodontitis, tongue coatings favouring the bacterial growth and systemic diseases like diabetes mellitus, respiratory diseases and medications [1,2,10]. It is now widely accepted that the primary cause of oral malodor is the release of volatile sulphur compounds (VSCs) like hydrogen sulphide, dimethyl sulphide and methyl mercaptan [1,2].
Oil pulling is a traditional Indian folk remedy used to prevent and cure various diseases [12–14]. It is claimed to cure about 30 systemic diseases such as headache, migraine, diabetes and asthma. Studies have also demonstrated that it prevents dental decay, oral malodor, bleeding gums, dryness of throat, cracked lips and strengthens teeth, gums and jaws [15–22]. It is cost-effective compared to other treatment modalities [18]. As limited literature is available on the effects of oil pulling on oral malodor, this study aims to compare the efficacy of oil pulling and chlorhexidine in reducing oral malodor and microbes.
Materials and Methods
A double blind randomized controlled trial was conducted for 21 d in August 2012 to compare the efficacy of oil pulling (sesame oil) and chlorhexidine in reducing halitosis and microorganisms responsible for it [23]. Methodology was based on the Acceptance Program Guidelines given by American Dental Association, Council of Scientific Affairs 2003 [23].
Study population and sample size
Sixty subjects were recruited from the three hostels of Maharani Group of colleges: science, commerce and arts and home science colleges [Table/Fig-1]. Ethical clearance was obtained from Institution Review Board of Vokkaligara Sangha Dental College and Hospital and management of Maharani Group of Colleges and Smt. V.H.D. College of Home science. Informed consent was obtained from study subjects. Each hostel was assigned to one of the three groups namely; chlorhexidine (CHX, 0.2%, Hexidine, ICPA Health Products Ltd, India), oil (sesame oil, VVV Sons India) and placebo group using simple random sampling with the help of lottery method. Each group consisted of 20 girls. The inclusion criteria consisted of: subjects 18 y and above, with atleast 24 permanent teeth with gingival probing depth <3mm, gingival and plaque index scores of => 1 in 10% of the sites and intrinsic malodor of oral origin two or more hours after eating, drinking or brushing of teeth or any other oral activity. Exclusion criteria consisted of: subjects with systemic causes of malodor like diabetes, gastritis; oral diseases such as advanced periodontitis, frank dental caries, mucosal lesions, smokers, with orthodontic appliances; on medications like anti hypertensives, oral hypoglycaemics; history of use of antibiotics in past 3 to 4 wk and whose who got oral prophylaxis done less than a week ago [23]. Each participant was instructed to use 15ml of the intervention agent daily. The intervention agents were supplied in uniform bottles with instructions for quantity, duration and frequency of use. A small video demonstrating the use of the agents was also shown to study participants. The respective hostel wardens selected group allocation and monitored use of agent’s everyday.
Showing allocation of study participants according to CONSORT 2010
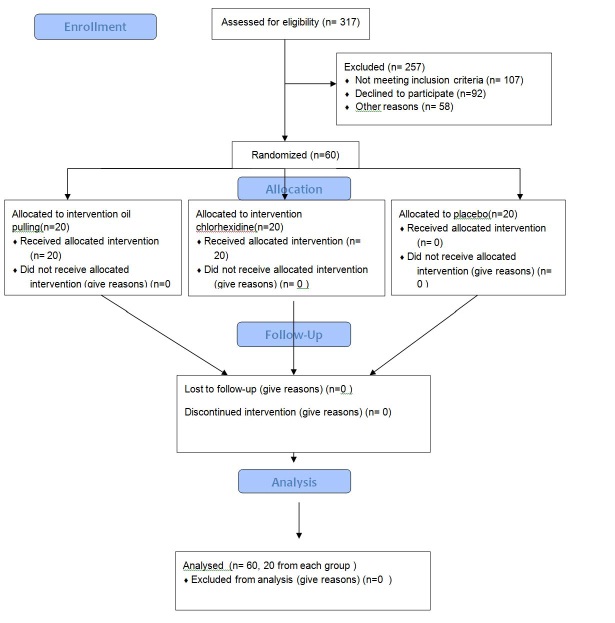
The sample size was estimated using the data from the study done by Ashokan et al., and taking prevalence of halitosis as 30- 40% [18].The final sample size for each group was 20 taking into account effect size.
Study tool
It consisted of a proforma divided into two parts. Part one consisted of structured interview which recorded demographic data, oral hygiene practices and past medical and dental history of the participants. The second part consisted of clinical assessment by using gingival and plaque index (Silness P and Loe H 1964), organoleptic intensity scale (Rosenberg) for oral malodor and microbial anerobic count using Robertson’s cooked meat media [23,24]. Two examiners were trained and calibrated to record plaque and gingival index and oral malodor respectively [23]. The examiners were blinded to group allocation. The intra examiner reliability was 0.90 and 0.86 respectively. Both were instructed not to eat and drink any odour producing substance like onions, garlic, alcohol, cigarettes 24 h before examination. They were also instructed not to use odour producing substances like perfumes, shampoos, body lotions and creams and aftershave 24 hours before examination. All the variables were recorded at baseline and after 21 d.
Statistical Analysis
Mean plaque (PI) and gingival (GI) scores and objective (ORG1) and subjective organoleptic scores (ORG2) per subject were calculated. Colony forming units per ml (CFU/ml) were calculated for anaerobic bacterial count (ABC) and transformed to logarithmic base (base 10). The group score was calculated by taking mean of individual subject scores. The data was analyzed using Kruskal Wallis test, Wilcoxan Sign Rank test, ANOVA and student t-test to determine if there was any statistical difference between and within the groups. Post hoc test was also done. The value of p< 0.05 was accepted as statistically significant. The analysis was performed using SPSS (17.0) software.
Results
The present randomized controlled study was conducted to compare the efficacy of oil pulling and chlorhexidine in reducing oral malodor and microbes causing it. All the study participants (N= 60) completed the study and all were females. The mean age of chlorhexidine group was 19.05 y (SD 1.47, range: 17- 23), oil group 18.60 y (SD 1.31, range: 17- 23) and placebo group 18.7 y (SD 1.03, range 17- 23) respectively. Oral hygiene practices across the three groups were similar. Tooth brush and tooth paste were the only oral hygiene aids used. None of the participants had visited dentist in the previous three months.
Mean Gingival and plaque index scores (GI and PI)
The mean gingival index scores reduced in all the three groups after 21 d of intervention. However, there was no statistically significant difference in the mean gingival index scores among the groups pre and post intervention (p< 0.05) [Table/Fig-2,3]. Wilcoxan sign rank test showed statistically significant reduction in the gingival index scores within each group (p<0.05) [Table/Fig-4,5,6] after 21 d. Similar results were seen for mean plaque index scores within and among the three groups.
Comparison of the mean baseline values of gingival index (GI), plaque index (PI), organoleptic scores and anaerobic bacterial colony count (ABC)among groups
| Parameter | Group | Mean scores (SD) | p- value |
|---|
| Gingival index scores (GI) | CHX | 1.77 (0.576) | 0.944* |
| Oil | 1.71 (0.512) |
| Placebo | 1.69 (0.506) |
| Plaque inde scores (PI) | CHX | 2.45 (0.44) | 0.982* |
| Oil | 2.41 (0.42) |
| Placebo | 2.39 (0.39) |
| Objective organoleptic scores (ORG1) | CHX | 3.6 (0.68) | 0.952* |
| Oil | 3.67 (0.66) |
| Placebo | 3.8 (0.670 |
| Anaerobic bacterial colony count (ABC) | CHX | 8.02 (0.82) | 0.844** |
| Oil | 7.99 (0.8) |
| Placebo | 7.8 (0.67) |
* P< 0.05, Kruskal Wallis test, ** P<0.05, ANOVA
Comparison of the mean post values of gingival index (GI), plaque index (PI), organoleptic scores and anaerobic bacterial colony count (ABC) among groups.
| Parameter | Group | Mean scores (SD) | p- value |
|---|
| Gingival index scores | CHX | 1.53 (0.541) | 0.606* |
| Oil | 1.49 (0.484) |
| Placebo | 1.53 (0.471) |
| Plaque index scores (PI) | CHX | 2.19 (0.44) | 0.384* |
| Oil | 2.41 (0.49) |
| Placebo | 2.27 (0.32) |
| Objective organoleptic scores (ORG1) | CHX | 2.2 (0.91) | 0.000* |
| Oil | 2.15 (0.81) |
| Placebo | 4.05 (0.94) |
| Subjective organoleptic scores (ORG2) | CHX | 1.95 (0.68) | 0.000* |
| Oil | 1.6 (0.6) |
| Placebo | 3.35 (0.66) |
| Anaerobic bacterial colony count (ABC) | CHX | 6.93 (0.3) | 0.000** |
| Oil | 7.06 (0.33) |
| Placebo | 7.8 (0.67) |
* P< 0.05, Kruskal Wallis test, ** P<0.05, ANOVA
Comparison of mean pre and post values of gingival index, plaque index, organoleptic scores and anaerobic colony count within CHX group
| Parameter | Time interval | Mean values (SD) | p- value |
|---|
| Gingival index (GI) | 0 day | 1.77 (0.58) | 0.000* |
| 22 day | 1.53 (0.54) |
| Plaque index (PI) | 0 day | 2.45 (0.44) | 0.000* |
| 22 day | 2.19 (0.19) |
| Objective organoleptic test (ORG1) | 0 day | 4.1 (0.91) | 0.000* |
| 22 day | 2.2 (0.83) |
| Subjective organoleptic test (ORG2) | 0 day | 3.6 (0.68) | 0.000* |
| 22 day | 1.95 (0.68) |
| Anaerobic colony count (ABC) | 0 day | 8.02 (0.82) | 0.000* |
| 22 day | 6.93 (0.3) |
* P<0.05,Wilcoxan sign rank test, ** P<0.05, Student t test
Comparison of mean pre and post values of gingival index, plaque index, organoleptic scores and anaerobic colony count within Oil group
| Parameter | Time interval | Mean values (SD) | p- value |
|---|
| Gingival index (GI)> | 0 day | 1.71 (0.51) | 0.000* |
| 22 day | 1.49 (0.48) |
| Plaque index (PI) | 0 day | 2.42 (0.42) | 0.000* |
| 22 day | 2.08 (0.49) |
| Objective organoleptic test(ORG1) | 0 day | 4.1 (0.85) | 0.000* |
| 22 day | 2.15 (0.81) |
| Subjective organoleptic test (ORG2) | 0 day | 3.67 (0.66) | 0.000* |
| 22 day | 1.6 (0.6) |
| Anaerobic colony count (ABC) | 0 day | 7.99 (0.8) | 0.000** |
| 22 day | 7.06 (0.33) |
* P<0.05,Wilcoxan sign rank test, ** P<0.05, Student t test
Comparison of mean pre and post values of gingival index, plaque index, organoleptic scores and anaerobic colony count within Placebo group
| Parameter | Time interval | Mean values (SD) | p- value |
|---|
| Gingival index (GI) | 0 day | 1.69 (0.46) | 0.001* |
| 22 day | 1.56 (0.40) |
| Plaque index (PI) | 0 day | 2.39 (0.30) | 0.000* |
| 22 day | 2.27 (0.32) |
| Objective organoleptic test (ORG1) | 0 day | 4.15 (0.86) | 0.157* |
| 22 day | 4.05 (0.94) |
| Subjective organoleptic test (ORG2) | 0 day | 3.8 (0.67) | 0.014* |
| 22 day | 3.15 (0.66) |
| Anaerobic colony count (ABC) | 0 day | 7.89 (0.68) | 0.01** |
| 22 day | 7.8 (0.67) |
* P<0.05,Wilcoxan sign rank test, ** P<0.05, Student t test
Mean organoleptic scores (ORG1 and ORG2)
Both ORG1 and ORG2 scores were measured and compared. The mean objective organoleptic scores were similar at the baseline among the three groups [Table/Fig-2]. However there was statistically significant difference (p<0.05) in scores post intervention [Table/Fig-3]. Post hoc test was done. It showed that difference in mean scores was statistically significant (p<0.05) between chlorhexidine and placebo group and between oil and placebo group [Table/Fig-7]. Also reduction in the mean objective organoleptic scores within chlorhexidine and oil pulling group was statistically significant after 21 d (p<0.05) [Table/Fig-4–6]. Similar results were seen for mean subjective organoleptic scores, except that significant reduction within placebo group was also observed (p<0.05) [Table/Fig-6]
Post hoc test for statistically significant parameters
| Parameter | Groups | Groups | Mean difference | p- value* |
|---|
| Objective organoleptic test (ORG1) | Placebo | CHX | 1.85 | 0.000 |
| Oil | 1.90 |
| Subjective organoleptic test (ORG2) | Placebo | CHX | 1.4 | 0.000 |
| Oil | 1.75 |
| Anaerobic bacterial colony count (ABC) | Placebo | CHX | 0.866 | 0.000 |
| Oil | 0.747 |
Anaerobic bacterial colony count (ABC)
Anaerobic bacterial colony count was measured in colony forming units (CFU/ ml). The samples were taken from tongue. The mean count was similar at the baseline among the three groups [Table/Fig-2]. However, there was statistically significant difference (p<0.05) among the groups in scores post intervention [Table/Fig-3]. Post hoc test was done. It showed that difference in mean scores was statistically significant (p<0.05) between chlorhexidine and placebo group and between oil and placebo group [Table/Fig-7]. Student t-test showed statistically significant (p<0.05) in counts within the three groups after 21 d [Table/Fig-4-6]. Study subjects reported problems long duration time for oil pulling and lingering aftertaste with chlorhexidine.
Discussion
The present randomized controlled trial compared the efficacy of oil pulling and chlorhexidine in reducing oral malodor and microorganisms causing it. Oil pulling is a traditional Indian folk remedy. It is an ayurvedic practice that involves swishing of oil in the mouth for oral and systemic health benefits [16–18]. The saponification and emulsification process during oil pulling is responsible for cleansing action of sesame oil [25]. It also generates antioxidants which kill microbes and cause their cell wall damage. In the present trial sesame oil was used for oil pulling as it is the most commonly used oil for the therapy and is known for several medicinal properties and desirable health benefits [12–15]. Its palatability is better compared to the other refined edible oils. It does not cause staining, lingering after taste and allergy unlike chlorhexidine. It is five to six times cost-effective than chlorhexidine and is readily available in every household [18]. However, duration of procedure is longer compared to chlorhexidine.
Chlorhexidine is considered most effective antiplaque and antigingivitis agent [2,26,27]. It provides a significant reduction in volatile sulphur compounds (VSC) levels and organoleptic scores (ORG) because of its strong antibacterial effects and superior substantivity in the oral cavity [2,26–28]. Hence, it was used as the positive control in this present clinical trial. The water with colorant acted as placebo.
Efficacy of oil pulling
The present study also showed significant reduction (p<0.05) in plaque and gingival index scores within all three groups. The finding is in accordance with the studies done by Amith et al., and Ashokan et al., [18–20]. There was no statistically significant difference (p<0.05) in the mean plaque and gingival index scores post intervention between chlorhexidine and oil group. The finding is similar to that reported by Ashokan et al., [19]. A significant reduction in the scores was seen in placebo group as well. It may be attributed to the disruption of the plaque due to rinsing action. The other studies have not taken placebo group.
In the present study there was statistically significant (p<0.000) reduction in the mean objective and subjective organoleptic scores within oil pulling and chlorhexidine group. Similar results were reported by Ashokan et al., [18]. The antimicrobial and anti oxidant action of sesame oil and chlorhexidine is responsible for decreased bacterial count, reduction in volatile sulphur compounds and hence scores [16,17]. The subjective ORG scores showed significant reduction (p<0.05) in placebo group in the present study. It may be attributed to the fact that subjects were aware that they were using some agent for prevention of oral malodor. The disruption of plaque and hence oral bacteria might be responsible for reduction in scores though placebo doesnot have any antibacterial action. Post intervention no statistically significant (p<0.05) reduction in scores was reported between oil and chlorhexidine group. A similar finding was reported by Ashokan et al., [18]. In the present study oil pulling group had significant reduction in organoleptic scores compared to placebo group post intervention.
Also, the mean anaerobic bacterial colony count reduced significantly (p<0.000) post intervention within oil pulling and chlorhexidine group. In two studies done by Ashokan et al., a definite reduction in the bacterial colony count was reported but it was not significant [18,20]. This may be attributed to the fact that duration of present study was 21 d compared to 14 and 10 d duration of other studies. There was statistically significant difference (p<0.000) between placebo and oil group and chlorhexidine and placebo group post intervention. The result is in accordance with Ashokan et al., studies [18,20].
The study subjects were also asked about their experience of using the interventions. The oil pulling group felt that the duration of procedure was long and the amount of oil was more. The palatability improved after one to two uses. Few of the study subjects from chlorhexidine group reported lingering aftertaste. This is in accordance with the study done by Amith et al., where subjects reported that a lot of motivation is required to do oil pulling [19].
The present study was conducted only among girls of relatively younger age group. However their selection was based on the relevant inclusion and exclusion criteria to keep bias at the minimum. The results cannot be generalized to other age groups. Also, oral chroma and halimeter were not used to record organoleptic scores due to cost considerations. However, the examiner was trained and calibrated to record objective organoleptic scores.
Conclusion
It can be concluded from this study that oil pulling therapy is equally effective like chlorhexidine in reducing oral malodor and microorganisms causing it. It promises to be a better preventive home care therapy in developing countries like India where accessibility, affordability, availability and sustainability are important issues. Further studies should be carried out with larger samples, varying time period of trial and reduced time period for oil pulling to establish its efficacy in prevention of oral malodor and open new doors in the field of research in oral health care.