Simultaneous Primary Hydatid Cysts of Liver and Spleen with Spontaneous Intraperitoneal Rupture of Liver Cyst
Sanjeev Kumar1, Shefali Gautam2, Ravi Prakash3, Suresh Kumar4, Vinod Kumar Srivastava5
1 Senior Resident, Department of General Surgery, K.G.’s Medical University, Lucknow U.P., India.
2 Senior Resident, Department of Anaesthesiology, K.G.’s Medical University, Lucknow U.P., India.
3 Senior Resident, Department of Anaesthesiology, K.G.’s Medical University, Lucknow U.P., India.
4 Professor, Department of General Surgery, K.G.’s Medical University, Lucknow U.P., India.
5 Senior Resident, Department of Anaesthesiology, K.G.’s Medical University, Lucknow U.P., India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ravi Prakash, MIG-82, Sector E, Aliganj, Lucknow, U.P., India. Phone : 9450610553, E-mail : drraviprakash94@gmail.com
Hydatid cyst, Intraperitoneal, Liver, Spleen, Shock
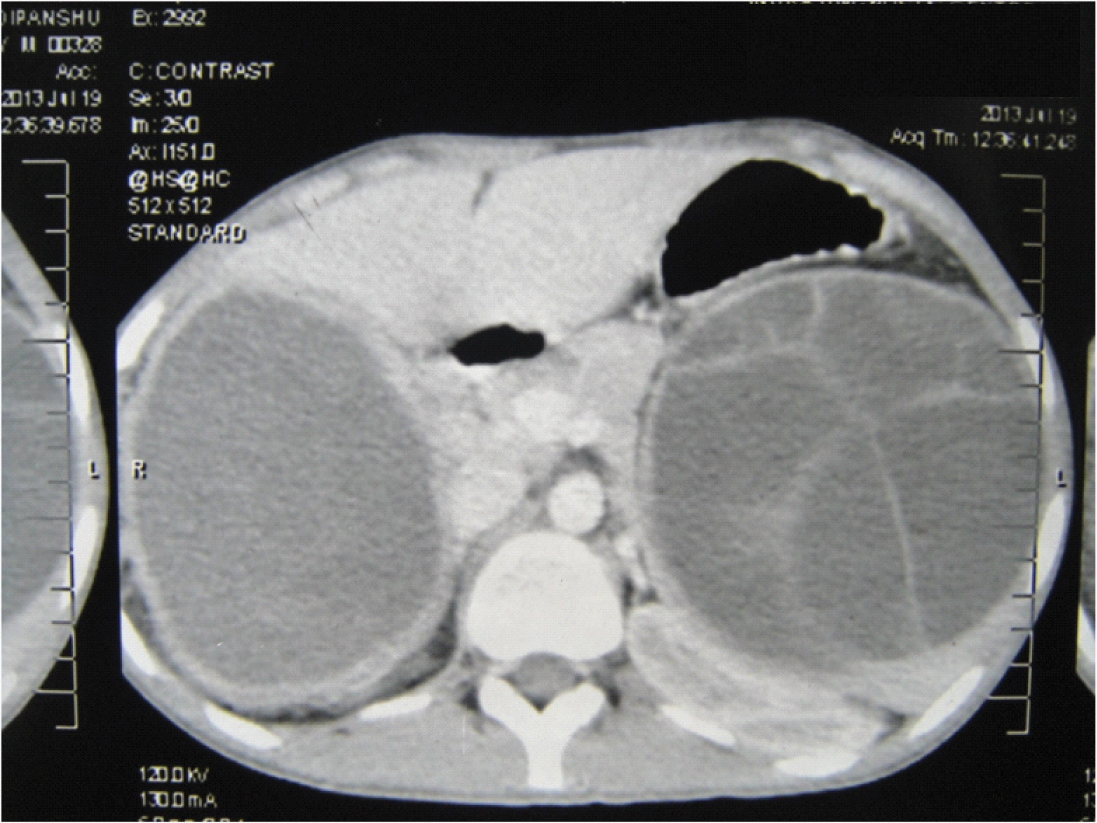
An 18-year-old male patient presented with recurrent vomiting, dull aching pain, heaviness and fullness in upper abdomen for approximately six month duration. On examination there was hepatosplenomegaly with mild tenderness and dullness on percussion. USG abdomen was suggestive of large cystic lesion in right lobe of liver and spleen. Patient underwent CECT abdomen which show large cyst of liver and spleen [Table/Fig-1]. Patient was planned for surgery and discharge on preoperative albendazole 400 mg BD with advice to follow weekly. Three days later, same patient presented to emergency department with sudden onset pain in abdomen associated with abdominal distention. On examination there was tachycardia (pulse 112/min), blood pressure was 90/60 mmHg, abdomen was tender and diffuse peritonitis was there.
CECT abdomen showing large cysts in liver and spleen
Patient was resuscitated for anaphylactic shock and peritonitis with intravenous fluid, antibiotics, antihistaminic and steroid. After resuscitation, emergency laparotomy was performed. On exploration, a ruptured liver cyst with collection in perihepatic area was revealed. Splenic cyst was also present but it was intact. The germinal membrane was removed from hepatic cyst pouch and splenectomy was performed [Table/Fig-2]. Specimen of spleen was consisting of multiple daughter cysts [Table/Fig-3]. The peritoneal as after renumbering only three figure will remain cavity was irrigated with warm 3% hypertonic saline for 15 min followed by tube drainage of cyst cavity. Post operative period was uneventful and patient was discharge on 9th postoperative day with albendazole therapy for three months. Three months later, there was no evidence of residual disease present.
Hepatic cyst after removal

Splenic cyst showing multiple daughter cysts

Discussion
Hydatid cysts compose of three layers: pericyst, laminated membrane and endocyst (germinal layer).The cyst fluid is a transudate of serum that contains proteins which is antigenic [1]. The most common site is liver (75%) and lung (15%). Kidney (3%), bone, brain, spleen, pancreas and omentum are other organ rarely involved [2,3]. Rupture of intraperitoneal cyst occur less often (3.2% to 16%) and usually occurs after trauma. Significant risk factors for spontaneous rupture are younger age, superficial cyst location, cyst diameter >10cms [4,5]. Intra-peritoneal rupture of a hydatid cyst is considered an urgent clinical event, and dissemination of cyst content poses a 1-2.5% risk of severe, life threatening anaphylactic shock [6]. Signs and symptoms of ruptured cyst are non-specific and patient presents with acute abdomen. USG abdomen is the investigation of choice, and diagnostic in 95% of cases. However, contrast CT gives more precise information regarding morphology (size and location) with 100% sensitivity.
[1]. Col C, Col M, Lafci H, Unusual localizations of hydatid diseaseActa Med Austriaca 2003 30:61-64. [Google Scholar]
[2]. Hamamci EO, Besim H, Korkmaz A, Unusual locations of hydatid disease and surgical approachANZ J Surg 2004 74:356-60. [Google Scholar]
[3]. Hayrullah D, Tugrul T, Enver R, Dogan Ali B, Okay N, Acute intraperitoneal rupture of hydatid cystsWorld J Surg 2006 30:1879-83. [Google Scholar]
[4]. Gulalp B, Koseoglu Z, Toprak N, Ruptured hydatid cyst following minimal trauma and few signs on presentationNeth J Med 2007 65:117-18. [Google Scholar]
[5]. Akcan A, Akyildiz H, Artis T, Peritoneal perforation of liver hydatid cysts: clinical presentation, predisposing factors, and surgical outcomeWorld J Surg 2007 31:1284-91. [Google Scholar]
[6]. Khan PS, Hayat H, Mushtaque M, Dar LA, Simultaneous primary hydatid cysts of liver and spleen with spontaneous intraperitoneal rupture of both cystsEastern Journal of Medicine 2012 17:130-32. [Google Scholar]