Classifications of serotypes recognized so far are based on genetic differences of their polysaccharide capsule. Serotypes of 4, 9V,18C, 19F, 23F, and 6B are the most important causes of invasive pneumococcal infections during childhood [4]. Among children with new pneumococcal serotypes, the disease in 15% of cases is likely to occur within one month after the microorganism enters the body. Pneumococcal infections occurring due to different serotypes are more widespread in autumn, and more frequently observed among infants, young adults, and elders [5].
In a study, six serotypes of e (1, 19A, 15C, 9V, 11A, and 19F) were found in Zahedan, Iran [6]. Colonization of S. pneumoniae in nasopharynx was also analysed, discovering that 40-50% of 8-week-old infants were carriers of S. pneumoniae and as the infants grew, acquired pneumonia increased among them [7]. Also among S. pneumoniae serotypes isolated from nasopharynx of the carrier children, the six serotypes of 23f, 19f, 6b, 14, 6a, and 3 were more widespread [8]. The heptavalent S. pneumoniae protein conjugate vaccine (PCV7) has polysaccharide conjugates of serotypes 4, 6B, 9V, 14, 18C, 19F and 23F. PCV7 was licensed for use in the United States in February 2000 and then added to the childhood immunization schedule in 2000 [9]. In a study in the USA, the incidence of invasive pneumococcal disease (IPD) decreased by 27% after the introduction of the PCV7 [10]. In another study a reduction was observed in pneumococcal meningitis cases in children under 16 within a 4 y period after universal pneumococcal conjugate vaccination in infancy [11].
Regarding that the rate of incidence and mortality due to infection with these bacteria is growing in children and the potential bacteria resistance to antibiotics.
Materials and Methods
This cross-sectional study was conducted in Cellular and Molecular Research Center of Shahrekord University of Medical Sciences, Shahrekord, Iran from September 2010 to September 2011 and approved by Research Ethics Committee of the University. In the present study, 372 children less than five years referred to the health care centers in Shahrekord, Chaharmahal and Bakhtiari (southwest Iran) were enrolled. All parents of the patients included in this project signed informed consent form. The information regarding the demographic data, result of throat culture, and serotypes were recorded.
Assuming 21% prevalence of carrier rate in the population, confidence interval of 95%, and relative error of 20%, the sample size was determined as 362 patients. For a more precision the sample size was raised to 372 children. A two stage sampling method was used, in the first stage 26 day care centers were chosen by simple random sampling and in the second stage, 15 children were selected from each center by convenience sampling. Healthy children under five years were enrolled in this study. Children with respiratory tract infection, otitis media, chronic disease or children who had received antibiotic within two weeks prior to entering into study were excluded.
The samples were obtained from nasopharyngeal secretion of these patients and specimens were streaked cultured on blood and chocolate agar plates. All media were overnight incubated for 18h to 24h at 35°C under 5% to 8% CO2.
On blood agar, colonies of differentiating S. pneumoniae produced a zone of alpha (green pigment) hemolysis. These colonies were streaked cultured again on blood agar and a filter paper disk, impregnated with Optochin, were placed in the streaked area. An inhibition zone of 14 mm or more around a 6-mm disk was used for identification of the viridance group streptococcus (VGS) and S. pneumoniae. If the inhibition zone was less than 14 mm, bile solubility or serology tests would be used for identification of S. pneumoniae.
DNA Extraction
Bacterial DNA was extracted from each colonies using DNPTM Kit (Cinna Gen, Iran) according to the manufacturer’s recommendation. The isolated DNA was quantified by spectrophotometric measurement at 260 nm wavelength according to the method described by Sambrook and Russell [12]. The extracted DNA of each sample was kept frozen at -20°C until used.
Multiplex PCR Assay
In the present study, Multiplex PCR technique was used for investigation of serotypes of S. pneumoniae. Also, the oligonucleotide primers described by Jourdain et al., and Brito et al., were used in this study. The sequences of primers [13,14] for amplification of serotypes of S. pneumonia are given in [Table/Fig-1].
Primers used for identification of Streptococcus pneumoniae serotype
| Primer | Sequences | Accession number (GenBank) | Amp-licon size (bp) |
|---|
| S.pne4-F S.pne4-R | 5’-CTGTTACTTGTTCTGGACTCTCGATAATTGG-3’ 5’-GCCCACTCCTGTTAAAATCCTACCCGCATTG-3’ | AF316639 | 430 |
| S.pne6B-F S.pne6B-R | 5’-CGACGTAACAAAGAACTAGGTGCTGAAAC-3’ 5’-AAGTATATAACCACGCTGTAAAACTCTGAC-3’ | AF316640 | 220 |
| S.pne9V-F S.pne9V-R | 5’-CTTCGTTAGTTAAAATTCTAAATTTTTCTAAG-3’ 5’-GTCCCAATACCAGTCCTTGCAACACAAG-3’ | AF402095 | 753 |
| S.pne14-F S.pne14-R | 5’-GAAATGTTACTTGGCGCAGGTGTCAGAATT-3’ 5’-GCCAATACTTCTTAGTCTCTCAGATGAAT-3’ | X85787 | 189 |
| S.pne18C-F S.pne18C-R | 5’-CTTAATAGCTCTCATTATTCTTTTTTTAAGCC -3’ 5’-TTATCTGTAAACCATATCAGCATCTGAAAC-3’ | AF316642 | 573 |
| S.pne19F-F S.pne19F-R | 5’-GTTAAGATTGCTGATCGATTAATTGATATCC-3’ 5’-GTAATATGTCTTTAGGGCGTTTATGGCGATAG-3’ | U09239 | 304 |
| S.pne23F-F S.pne23F-R | 5’-GTAACAGTTGCTGTAGAGGGAATTGGCTTTTC-3’ 5’-CACAACACCTAACACTCGATGGCTATATGATTC-3’ | AF057294 | 384 |
S. pneumoniae ATCC strain 33400 was used as a positive control. A negative-DNA control was performed by adding 1 μL of sterile ultrapure deionized water. For investigation of S. pneumoniae serotypes, the samples were amplified in a Gradient Palm Cycler (Corbett Research, Australia) and Multiplex PCR reaction was performed in a total volume of 25 μL in 0.5 ml tubes containing 1 μg of genomic DNA, 1 μM of each primers, 2 mM Mgcl2, 200 μMdNTP, 2.5 μL of 10X PCR buffer, and 1 unit of Taq DNA polymerase (Roche applied science, Germany). PCR cycles consisted of an initial denaturation step (95°C for 5 min) followed by 30 amplification cycles (Denaturation at 94°C for 1 min, annealing at 65°C for 1 min, and elongation at 72°C for 1 min) with a final elongation at 72°C for 5 min,and amplified samples were holed at 4°C.
Analysis of Multiplex PCR Products
The amplified products were detected in 1% agarose gel electrophoresis. The electrode buffer was TBE (Tris-base 10.8 g 89 mM, Boric acid 5.5 g, 2 mM EDTA (pH 8.0), 4 ml of 0.5 M EDTA (pH 8.0) concentration), combined all components in sufficient H2O and stir to dissolve. Aliquots of 10 μL of PCR products were applied to the gel. Constant voltage of 80 V for 30 min was used for products separation. The DNA fragment size was compared with a standard molecular weight (100 bp DNA ladder of Fermentas, Germany). After electrophoresis, the amplicons were visualized with ultraviolet light after Ethidium bromide (5 μg.mL–1) staining and photographs were obtained in gel documentation systems.
Statistical Analysis
The prevalence rates were calculated and analysed using the chi-square and t-test by SPSS. P-values less than 0.05 were considered statistically significant.
Results
This research aims to determine vaccine-related serotype distribution in nasopharyngeal carrier and healthy children less than five years.
Three hundred seventy two specimens were totally taken. Nine specimens of the participants older than five years old were excluded to ensure that all specimens are under five years. Some characteristics of the cases have been summarized in [Table/Fig-2].
Some characteristics of the cases under the study
| Variable | Frequency | Percent |
|---|
| Gender | Girl | 191 | 52.6 |
| Boy | 172 | 47.4 |
| Smoking among family members | Yes | 53 | 14.6 |
| No | 310 | 85.4 |
| Antibiotic taking | Yes | 220 | 60.6 |
| No | 143 | 39.4 |
| Hospitalization | Yes | 30 | 8.3 |
| No | 333 | 91.7 |
| Otitis media | Yes | 53 | 14.6 |
| No | 310 | 85.4 |
| Adenoidectomy | Yes | 35 | 9.6 |
| No | 328 | 90.4 |
Overall, 107 samples were positive, so the rate of pneumococcal carriers obtained as 29.5% with 95% confidence interval as 24.8-34.5%.
Carriers were largely 4-5 y old and the mean age of the participants with positive and negative culture was 4.23±0.84 and 4.29±0.95 y respectively (range: 0-5). No significant relationship was observed among prevalence of pneumococcal carriers, age and gender (p>0.05).
The pneumococcal prevalence was 30.9% in girls and 27.9% in boys, and no significant difference was seen between prevalence of pneumococcal carriers and gender (p>0.05).
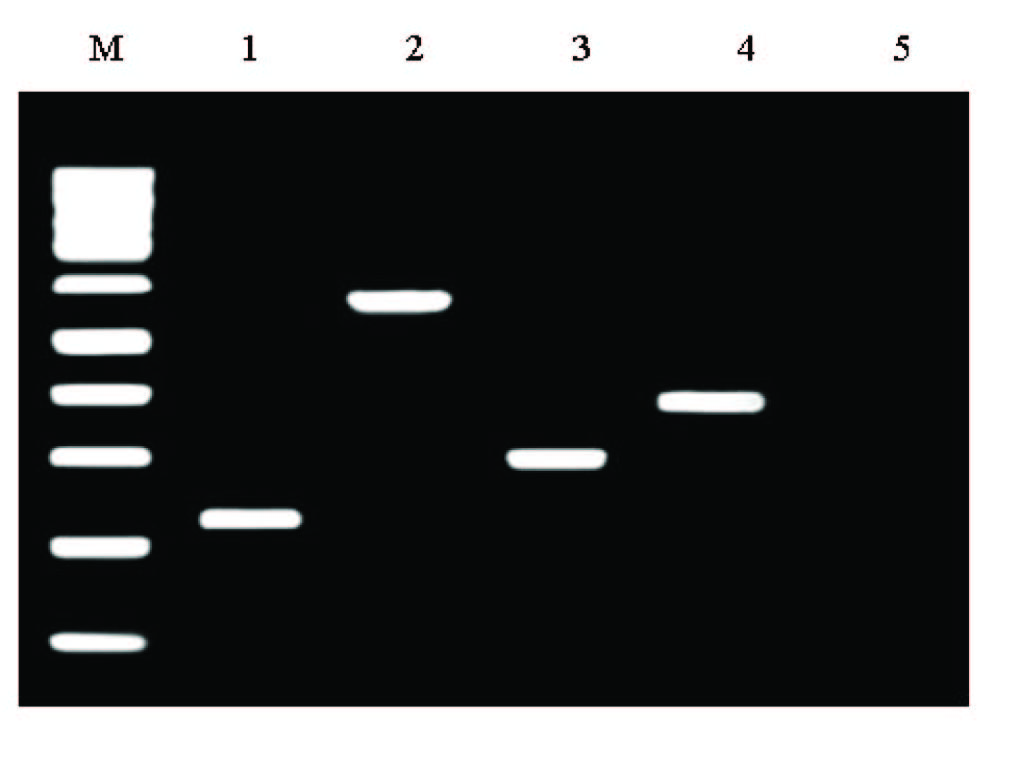
Electrophoresis of PCR products and positive cultures for detection of serotypes of S. pneumonia have been shown in [Table/Fig-3,4,5].
Frequency of different serotypes of Streptococcus pneumonia that detected from electrophoresis
| Serotype | Size (bp(s)) | Number | Percent |
|---|
| 23F | 384 | 16 | 43 |
| 6B | 220 | 13 | 34 |
| 19F | 304 | 7 | 18 |
| 18C | 573 | 2 | 5 |
| Total | - | 38 | 100 |
Frequency of different serotypes of Streptococcus pneumonia that detected from positive culture
| Serotype | Percent |
|---|
| 23F, 6B, 19F, and 18C | 2.7 |
| 19F and 18C | 2.7 |
| 23F and 6B | 21 |
| 23F, 6B, and 19F | 13 |
| 6B and 19F | 2.7 |
Line M: 100 bp DNA ladder (Fermentas, Germany), lines 1-5 represent 6B, 18C, 19F, and 23F serotypes of S. pneumoniae and negative control without DNA, respectively, in Gel electrophoresis of multiplex PCR for detection of serotypes of S. pneumoniae isolated from nasopharyngeal of patients
Discussion
For effective control of invasive pneumococcal infection, the composition of vaccine must match the prevalence of serotypes at local regions. In this study the prevalence of different serotypes of these bacteria in the children under the age of five was analysed. It has been already proved that this incidence is more prevalent among this age group. The findings of this study are consistent with those of studies done in other countries; as children get older, the acquisition of these bacteria increases [8].
In this study, four various serotypes of S. pneumoniae bacteria including 23F, 6B, 19F, and 18C using Multiplex-PCR with prevalence of each serotype reported as 43%, 34%, 18%, and 5% respectively were isolated and other serotypes of these bacteria were not found; while in a study in Zahedan, Iran six serotypes of 19F, 1, 19A, 15C, 9V, and 11A were the most common ones [15].
In Taiwan, six serotypes of 23F, 19F, 6B, 14, 6A, and 3 in comparison to other serotypes were more common [9], that is consistent with the discovered serotypes in the present study.
In a study carried out in Brazil on the meningitis patients varying one month old to 85 y old, serotypes of 5, 23F, 18C, 10A, 6B, 6A, 7F, 3, 19F, 14, and 34 were found [16].
Besides, in the present study no meaningful difference was observed between the increase of Streptococcus carriers, age, sex, the number of family members, and state of being smoker, history of hospitalization during the last 6 mnth, history of otitis media during the last 6 mnth, history of suffering from adenoidectomy, and consumption of antibiotic. It is assumed that there is no relationship between these parameters and pneumococcal carrier.
The occurrence of IPD and pneumococcal meningitis in children under 2-year-old was respectively 2 and 10 times higher compared to the general population, highlighting the importance of pneumococcal vaccination in children [17]. PCV7 vaccine was introduced by FDA in 2000 [9,18]. In the year after the introduction of PCV7, the Centers for Disease Control and Prevention Active Bacterial Core sites reported a 69% decrease in the rate of IPD for 0- to 24-month children [19]. PCV7 has an efficacy of 94% against IPD due to serotypes included in the vaccine and 89% against any IPD, regardless of serotype, in a large pre-licensure clinical trial in California [20]. Since PCV7 introduction, the most common IPD isolates in Belgium, France, Germany, Greece, Norway, Portugal, Spain, and the UK were serotypes 1, 19A, 3, 6A, and 7F [21]. Infant PCV7 vaccination in Germany caused a decrease in pneumococcal meningitis similar to what happened in England and Wales [11]. In the USA, introduction of PCV7 was followed by a 27% reduction in IPD among under 18 years and a 35% reduction among children under 2-year-old [15]. For PCV7 and other PCV13, the safety efficacy and effectiveness have been, in practice, established in different settings [22,23]. 13-valent pneumococcal conjugate vaccine includes capsular antigens of serotypes 1, 3, 4, 5, 6A, 6B, 7F, 9V, 14, 18C, 19A, 19F, and 23F [24]. The implementation of the 13-valent pneumococcal conjugate vaccine for children under 2-year-old in Argentina could be an effective strategy to be implemented in other countries for the decrease in invasive disease [25] and nasopharyngeal carriage of S. pneumonia [26]. In a study, 82.2% of S. pneumoniae serotypes were included in the 13-valent pneumococcal conjugate vaccine in children of 48.3 month age [27].
In our country heptavalent vaccination against S. pneumonia bacteria has not yet been implemented while most carriers of serotypes under study (23F, 6B, 19F, 18C) were discovered in heptavalent vaccine.
Based on the studies done, heptavalent vaccination against S. pneumoniae bacteria has not yet been implemented in our country while most carriers of serotypes under study (23F, 6B, 19F, 18C) were discovered in heptavalent vaccine.
Conclusion
In addition, regarding to high statistics of pneumonic carriers (relatively 30% in children under the age of five) in Shahrekord region, attributable to coldness of weather and lack of vaccination, the necessity of use of this vaccine seems inevitable. Based on the findings of the present study, it could be concluded that since Streptococcus pneumonia is pathogenic in children, PCV-7 should be also administered for children under five years old in Iran. This vaccine can be made based on the discovered serotypes. Further research on unconsidered serotypes is required.