Malignant Colojejunal Fistula First Discovered on CT: A Case Report
Griselda Philomena Noronha1, Rudresh Hiremath2, Aishwarya K.C.3, Deepthi Tippani4, Aruna C.R.5
1 Junior Resident, Department of Radio-diognasis, K.V.G. Medical College Hospital, Sullia, Dakshina Kannada, Karnataka, India.
2 Associate Professor, Department of Radio-diognasis, K.V.G. Medical College Hospital, Sullia, Dakshina Kannada, Karnataka, India.
3 Assistant Professor, Department of Radio-diognasis, K.V.G. Medical College Hospital, Sullia, Dakshina Kannada, Karnataka, India.
4 Junior Resident, Department of Radio-diognasis, K.V.G. Medical College Hospital, Sullia, Dakshina Kannada, Karnataka, India.
5 Senior Resident, Department of Radio-diognasis, K.V.G. Medical College Hospital, Sullia, Dakshina Kannada, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Griselda Philomena Noronha, Junior Resident, Department of Radio-diognasis, K.V.G. Medical College Hospital, Sullia, Dakshina Kannada-574239, Karnataka, India.
Phone: 9620500155
Benign coloenteric fistula is an uncommon condition. It may occur secondary to diverticular disease, peptic ulcer, inflammatory bowel disease and so on. Malignant coloenteric fistula is a rare occurrence. Here we present a rare case of malignant colojejunal fistula secondary to locally invading colonic malignancy.
Colonic malignancy, Colojejunal fistula, Locally invading
Case Report
A 55-year-old female patient presented with constipation, loss of appetite and significant weight loss since 3 months followed by watery diarrhea since two weeks. She also complained of abdominal pain since 10 days which was vague, dull aching and diffuse. There was no history of abdominal distension, vomiting or fever. On clinical examination, there was no abdominal tenderness or palpable abdominal mass. Bowel sounds were normal on auscultation. Ultrasound abdomen was performed elsewhere one week back which showed bowel wall thickening in the left hypochondrium suspicious for bowel malignancy. Contrast enhanced Computed Tomography (CECT) abdomen study was performed for confirmation and staging of the bowel malignancy. CT topogram after rectal contrast instillation showed opacification only upto proximal third of transverse colon [Table/Fig-1].
CT Topogram after rectal contrast instillation showing colonic opacification upto the distal third of transverse colon. Rest of the proximal two thirds of transverse colon and ascending colon are unopacified

CECT abdomen revealed diffuse circumferential heterogeneously enhancing wall thickening of short segment of proximal descending colon, splenic flexure and distal transverse colon. The maximum wall thickness measured 28 mm and the approximate length of large bowel that was involved measured 8.0cms. The wall thickening caused significant luminal narrowing as a result of which the rectal contrast failed to opacify the mid and distal thirds of transverse colon and ascending colon. The involved bowel segment showed pericolonic fat stranding. There were few subcentimetric minimally enhancing pericolonic lymph nodes adjacent to the lesion. Quite unexpectedly, the mass lesion was seen infiltrating the wall of the adjacent proximal jejunum with the luminal contrast from the colon entering the proximal jejunum. Since the patient was only given rectal contrast and no oral contrast was given, it was easier to demonstrate the fistulous communication between the colon and the jejunum with the positive colonic contrast entering the unopacified jejunum [Table/Fig-2,3,4]. The patient was treated conservatively with total parental nutrition and pain control. Patient refused to undergo surgery and further management. She was discharged as per her and her family’s request.
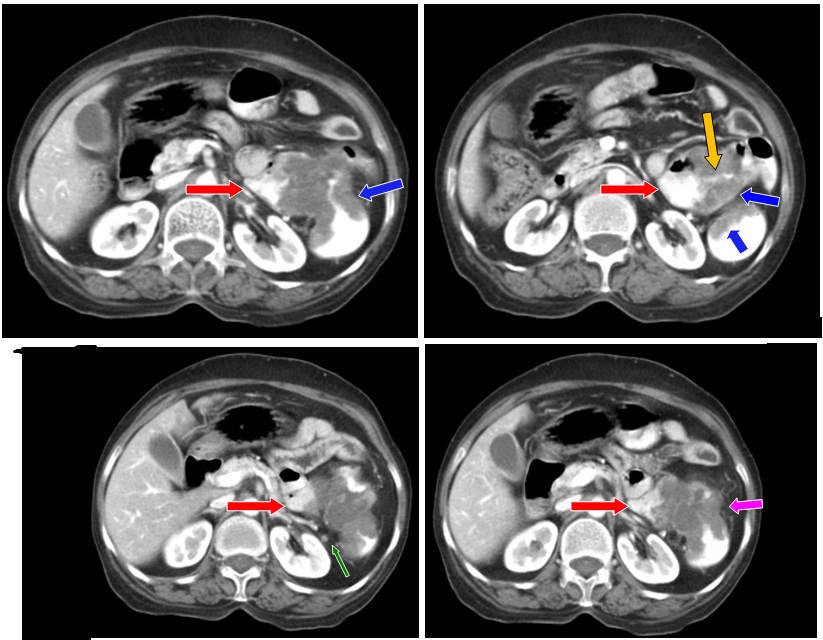
Contrast enhanced axial CT images with rectal contrast study shows heterogeneously enhancing mass lesion (blue arrow) in the splenic flexure causing significant luminal narrowing. The colonic mass lesion is seen infiltrating into the adjacent proximal jejunum (red arrow) with a short fistulous track (yellow arrow). A subcentimetric enhancing perilesional lymph node is noted (green arrow). Pericolonic fat stranding is noted (pink arrow)
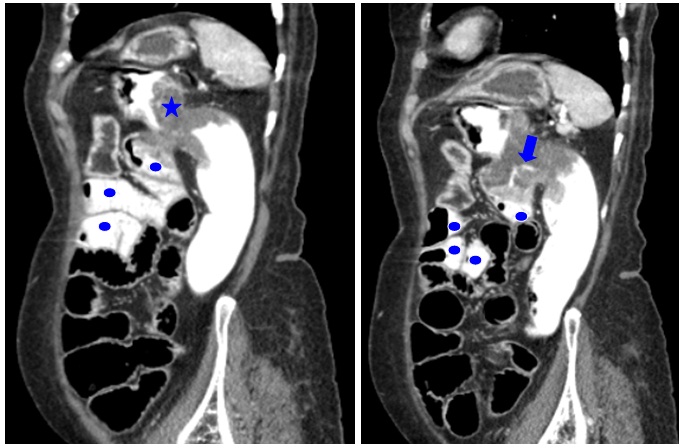
CECT abdomen with rectal contrast study saggital reformatted images shows short segment wall thickening (blue star) of splenic flexure extending into the distal transverse colon and proximal descending colon causing significant luminal narrowing. There is infiltration into the adjacent proximal jejunum inferiorly with short fistulous track (blue arrow).The rectal contrast is seen within few of the proximal jejunal loops (blue dot)
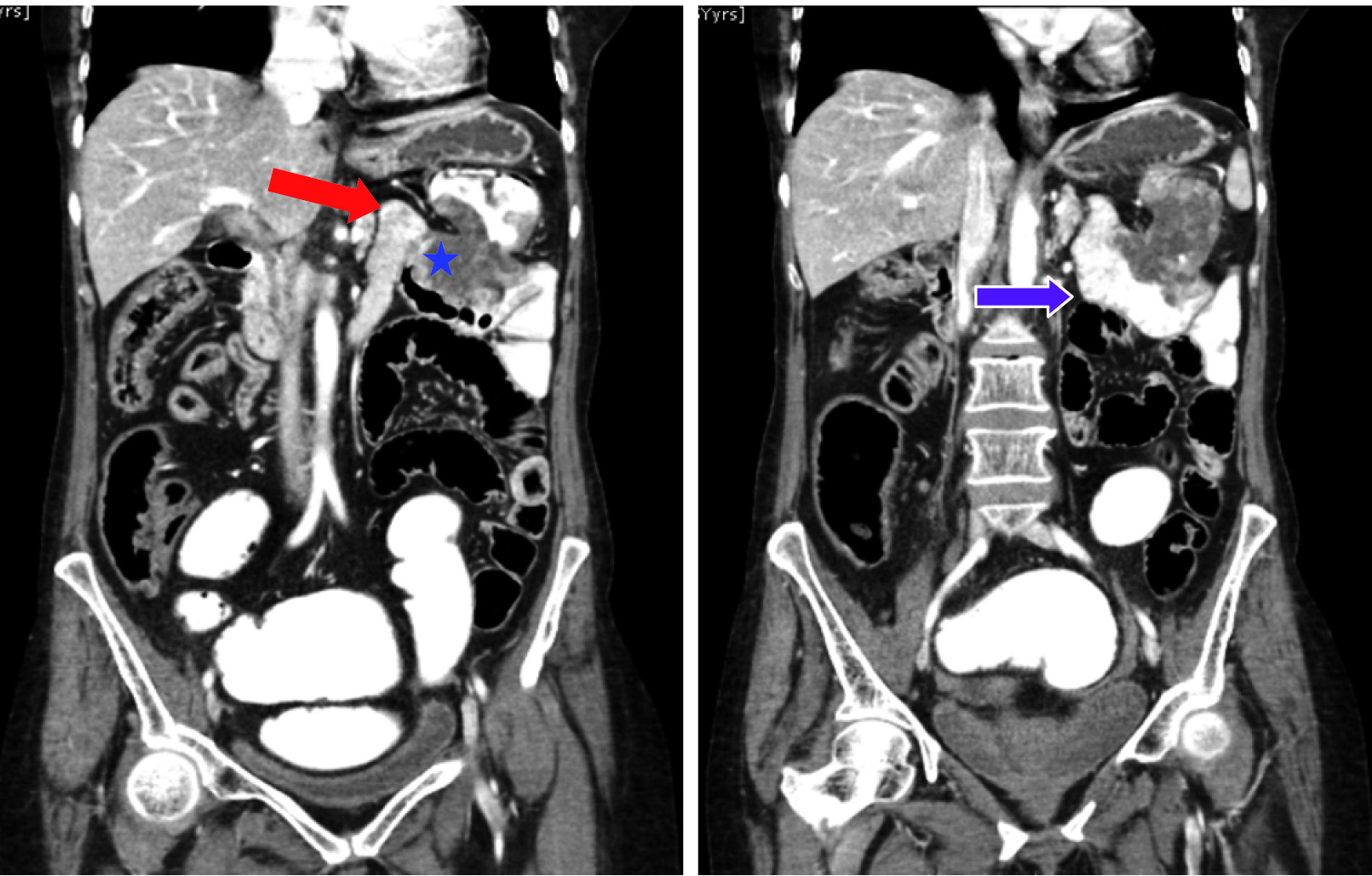
CECT abdomen with rectal contrast study coronal reformatted images shows normal duodeno-jejunal (DJ) junction (red arrow) and infiltration of proximal jejunum (blue star) by colonic malignant lesion. Note the evenly spaced valvulae conniventes of proximal jejunum (purple arrow) is faintly seen through the positive luminal contrast
Discussion
Malignant colojejunal fistula is rarely encountered and the exact incidence is unknown [1]. On review of literature, there are two schools of thoughts regarding the most common type of malignant coloenteric fistula. According to the two case reports, coloileal fistula usually secondary to adenocarcinoma of the sigmoid colon is the commonest [1,2]. On the other hand, one case report says that malignant coloduodenal fistula between the proximal transverse colon and the duodenum is common because of their close proximity [3]. Whatsoever, malignant colojejunal fistulas are of rare occurrence. SK Mahajan et al., reported a case of malignant colojejunal fistula with the primary being adenocarcinoma of the rectosigmoid junction [1]. Chun HB et al., reported another rare case of malignant colojejunal fistula secondary to lymphoma of the distal transverse colon [2].
In case of an internal intestinal fistulization, if the length of the bowel loop that is bypassed is short, it goes unrecognized. But if the length of the bypassed bowel loop is long, then there will be significant metabolic and nutritional deficiencies. It is a well-known fact that poor dietary intake due to decreased appetite secondary to malignancy leads to weight loss. In addition, fistualization adds on to the ongoing weight loss [1].
The route of spread in colojejunal fistula is postulated due to direct local invasion of jejunum by colon cancer via transverse mesocolon [4].
Clinical manifestation of gut to gut fistula is subtle as only gastrointestinal tract (GIT) is involved [5]. Diarrhoea with or without abdominal pain is the most common symptom [5]. Majority being clinically silent, it is often first discovered at imaging, sometimes accidentally on CT. Barium studies, endoscopy and CT enterography (CTE) are other useful diagnostic tools [2]. But these modalities can be used only when there is clinical suspicion of fistula. Barium studies and endoscopy have limitations as they are mainly luminal studies.
CT is more accurate and demonstrates both luminal and extraluminal pathology like abscess, bowel wall inflammation and metastasis. CTE which uses negative oral contrast medium has higher sensitivity in detecting luminal pathology and subtle mucosal lesions than routine CT which uses positive oral contrast medium. The main drawback of CTE over routine CT is that the former may miss small abscesses as they are obscured by the negative luminal contrast making it difficult to identify them amidst the low attenuation bowel loops. Hence routine CT is superior to CTE in identifying smaller abscesses [6]. The coexistence of fistula with intra abdominal abscess is reported to be 44%. The coexistent abscess must be treated to prevent sepsis and for fistula closure. Image guided percutaneous interventional therapy can be used in large abscesses [3].
Magnetic resonance imaging (MRI) is upcoming modality in small bowel imaging but has got suboptimal spatial and temporal resolution as compared to CT [3]. Colour Doppler Sonography may be tried for detection of fluid movement within the fistulous tract under manual and transducer compression. Kim HC et al., reported a case of gastro-colic fistula that was initially diagnosed on ultrasonography [7].
Malignant bowel fistula is associated with serious complications resulting in high morbidity and mortality rates. Firstly, advanced malignancy itself is a life threatening condition. Secondly, fistula related complications like fluid and electrolyte imbalances, malnutrition, abscess, sepsis, multi-organ failure and bleeding further reduces the patient survival [4].
The treatment of malignant colojejunal fistula is controversial. Malignant bowel fistula is less likely to close spontaneously [4]. Hence surgical correction is essential for successful treatment. Short life expectancy and high risk surgery makes few clinicians hesitant to proceed with the surgery. On the other hand few clinicians operate on the patient as palliative mode with careful surgical resection of the underlying obstructive malignancy. The prognosis of surgery in these patients is good when there is no nodal metastasis [1].
Conclusion
Malignant colojejunal fistula is rare and is usually from the primary in the sigmoid colon. It is associated with serious complications and subsequent high morbidity and mortality. The clinical manifestation is subtle and is often first discovered on imaging, sometimes serendipitously on Computed Tomography. Computed Tomography Enterography is preferred for the demonstration of fistula whereas routine Computed Tomography is preferred for extraluminal pathology like malignant growth and abscess. Detection of fistula and its complications has a great impact in the management and prognosis which when appropriately detected, reduces the debilitating metabolic and nutritional deficiencies, thereby improving the patient morbidity and mortality.
[1]. Mahajan SK, Sood BR, Vaidya P, Thakur S, Pal LS, Malignant colo-jejunal fistula- A Rare internal fistulaJAPI 2006 54:1336-37. [Google Scholar]
[2]. Chun BH, Baek IH, Lee MS, Kim JB, Shin SR, Kim BC, Jejunocolic fistula associated with an intestinal T cell lymphomaGut and Liver 2011 5(3):387-90. [Google Scholar]
[3]. Torosian MH, Zins JE, Rombeau JL, Malignant colojejunal fistula: case report and review of malignant coloenteric fistulaDiseases of the Colon & Rectum 1982 25(3):1-2. [Google Scholar]
[4]. Falconi M, Pederzoli P, The relevance of gastrointestinal fistulae in clinical practice: a reviewGut 2001 49(Suppl iv):iv2-iv10. [Google Scholar]
[5]. Pickhardt PJ, Bhalla S, Balfe DM, Acquired gastrointestinal fistulas: classification, etiologies, and imaging evaluationRadiology 2002 224(1):9-23. [Google Scholar]
[6]. Lee JK, Stein SL, Radiographic and endoscopic diagnosis and treatment of enterocutaneous fistulasClinics in Colon and Rectal Surgery 2010 23(3):149-60. [Google Scholar]
[7]. Kim HC, Yang DM, Jin W, Appearance of a gastrocolic fistula on sonography including color flowJ Ultrasound Med 2008 27:1767-69. [Google Scholar]