Domestic Violence and its Effect on Oral Health Behaviour and Oral Health Status
Hansa Kundu1, Basavaraj P2, Ashish Singla3, Sunder Kote4, Shilpi Singh5, Swati Jain6, Khushboo Singh7, Vaibhav Vashishtha8
1 Tutor, Department of Public Health Dentistry, Modinagar, Ghaziabad, Uttar Pradesh, India.
2 Professor & Head Department, Department of Public Health Dentistry, Modinagar, Ghaziabad, Uttar Pradesh, India.
3 Reader, Department of Public Health Dentistry, Modinagar, Ghaziabad, Uttar Pradesh, India.
4 Reader Department of Public Health Dentistry, Modinagar, Ghaziabad, Uttar Pradesh, India.
5 Senior Lecturer, Department of Public Health Dentistry, Modinagar, Ghaziabad, Uttar Pradesh, India.
6 Tutor, Department of Public Health Dentistry, Modinagar, Ghaziabad, Uttar Pradesh, India.
7 Tutor, Department of Public Health Dentistry, Modinagar, Ghaziabad, Uttar Pradesh, India.
8 Tutor, Department of Public Health Dentistry, Modinagar, Ghaziabad, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Hansa Kundu, Tutor, Department of Public Health Dentistry, D.J. College of Dental Sciences and Research, Ajit mahal, Niwari Road Modinagar, Ghaziabad -201204 (U.P.), India. Phone : +919761925531, E-mail : hansa.bds@gmail.com
Introduction: Violence against women is one of the major public health and human rights problem in the world today. Hence, the present study was conducted with the aim to assess the effect of domestic violence on oral health behavior and oral health status of females attending community outreach programmes in and around Modinagar.
Materials and Methods: A cross-sectional study was conducted through the community outreach programmes organized in Modinagar. A structured questionnaire was used to illicit information regarding socio demographic characteristics, oral health behavior and domestic violence. The dental health examination was done to record dental health status, intraoral and extraoral soft tissue injury, tooth fracture and tooth avulsion due to the injury.
Results: Out of the total 304 women, 204(67.1%) reported positive domestic violence. Psychological violence was found to be severe whereas sexual violence was found to be mild in most of the cases. Significant difference was found between oral hygiene aids used , frequency of tooth brushing, periodontal status, missing teeth, intraoral soft tissue injuries and fractures between both the groups (p<0.05).
Conclusion: The present study confirmed that domestic violence had significant influence on oral health behavior and oral health status of women. Thus, the dental professionals also should make an attempt to help victims gain access to support and referral services and to provide adequate treatment to them so as to make a positive difference in their lives.
Abuse, Domestic violence, Oral health behaviour, Oral health status
Introduction
Health is a multifactorial phenomenon where physical, mental and social well being is of equal importance. Disturbance in any of these factors can influence the overall health of an individual. Violence is one such reason which causes ill-health and women are the common victims for the same. Violence against women is one of the major public health and human rights problem in the world today. It is one of the forms of violence against women and refers to violence emanating from the household and within relationships covered by familial or emotional (former or present) attachment. It remains a hidden problem for women attending clinical practice as they are hesitant to talk about it in public and contributes majorly to their mental ill health globally [1]. United Nations Declaration on the Elimination of Violence against Women, 85th plenary meeting, December 1993 defined “Violence against women as any act of gender-based violence that results in, or is likely to result in, physical, sexual or mental harm or suffering to women, including threats of such acts, coercion or arbitrary deprivation of liberty, whether occurring in public or in private life” [2]. However, despite the fact that domestic violence has been the focus of research since the 1970s, information about the prevalence of this problem is still scarce in many countries, especially in the developing world. Current studies indicate that 20% - 50% of women worldwide have experienced some form of domestic violence in their lifetime [3,4]. Domestic violence is an age old social evil which remained hidden from the eyes of the society for long because there is widespread hesitancy amongst most Indian women who experience domestic violence to report or prosecute against such crimes [5]. The results of this hesitancy to report cases is clear in that reported data overwhelmingly tends to underestimate actual prevalence occurrences of domestic violence. In a 2000 multi-site household survey conducted in India, it was found that while overall approximately 50% of women surveyed had experienced some form of domestic violence throughout their married life, the rates varied significantly by specific location as well as overall region. In rural areas and urban slums, that rate was approximately 55%, whereas in urban non-slum areas the rate was less than 40% [6].
Domestic Violence has been identified as a major contributor to the global burden of ill health in terms of female morbidity and mortality, leading to psychological trauma and depression, injuries, sexually transmitted diseases, suicide and murder [7–11].
The health related implications of the physical and psychological component of the domestic violence are not limited to general health but also may impact dental health. Physiological consequences of depression may lead to poor dental health due to xerostomia, cariogenic diet, and impaired immune functioning contributing to oral infection [12–14]. The potential fallout from stress and anxiety can lead to diseases like Mouth sores, including canker sores, cold sores, clenching of teeth, teeth grinding (bruxism), periodontal disease and dental caries [15]. It can also affect the oral health behavior and personality of individual. Dental neglect—“the inability to seek and follow through with treatment necessary to ensure a level of oral health essential for adequate function and freedom from pain and infection” is common in battered women. It is found that these abusive partners control their access to health care [16]. The physical component of the domestic violence can be related to the injuries of head and neck region including, ligature marks, scratches, abrasions, and scrapes, petechia on the neck, face, eyes, mouth, swelling, and difficulty in swallowing. It has been documented that 38.7% of DV injuries are related to head and neck region [17].
Although, it is assumed that oral health of a victim gets affected by domestic violence there has been no documented evidence of the correlation between the domestic violence and dental health. Hence, the present study was conducted with the aim to assess the effect of domestic violence on oral health behavior and oral health status of female attending community outreach programmes in and around Modinagar.
Materials and Methods
A cross-sectional study was conducted in the community outreach programmes conducted by Department of Public Health Dentistry, D.J College of Dental Sciences and Research Modinagar in the month of August and September 2013. All the married women belonging to lower socioeconomic strata (according to Modified Prasad classification 1970) [18], who were married for more than five years and gave informed consent were included in the study. Those women with any kind of Psychiatric disorder/ on any kind of medication were excluded from the study. A total of six outreach programs were organized to the nearby rural villages and all the female subjects were interviewed making a total of 304 study subjects. Ethical clearance for the study was taken from the institutional review board.
A pretested structured questionnaire was used to illicit information regarding socio demographic characteristics, oral health behavior and domestic violence. The socio demographic information included information about age, years of marriage, education, occupation and socio economic status. Name of the subjects was not recorded to ensure the confidentiality. The oral hygiene behavior was recorded on the basis of Oral hygiene aids used, frequency of brushing and past dental visits. For assessment of Domestic Violence a semi-structured interview schedule adapted from WHO multi-country study on women’s health and domestic violence (2005) was used [19]. (Annexure-1) Domestic violence was assessed on the basis of three components -physical, sexual and psychological violence. The responses to the questions of each component were recorded on 5-point Likert scale (1-none of the time, 2- very rarely, 3-sometimes, 4- most of the time, 5- always). For every subject the scores of each question were added up for the individual component and interpreted as follows.
Psychological violence- 4= negative, 5-8= mild, 9-12= moderate, ≥13= severe
Physical Violence- 6= negative, 7-12= mild, 13-18= moderate, ≥ 19= severe
Sexual violence- 3=negative, 4-6= mild, 7-9= moderate, ≥10= severe.
The oral health examination was done to record information regarding dental caries, periodontal status, intraoral and extraoral soft tissue injury, tooth fracture and tooth avulsion due to the injury. The clinical examination and interview were carried out by a single trained female investigator. The interview was taken in a separate room where only subject and interviewer were allowed to reduce the bias. Intraexaminer reliability was found to be good (cohens kappa value=0.86).
Statistical Analysis
The data was entered in Microsoft word excel sheet 2007 and processed using SPSS version 19. Mean value of age in both the groups was calculated and the proportions (percentage of responses) were calculated for each parameter (psychological, physical and sexual). Chi-square test was used to analyse the difference between proportions for responses of individual parameters. The level of significance was set at 0.05. Furthermore, the relation between psychological, physical and sexual domestic violence with oral health behavior and oral health status was assessed using Pearson’s correlation.
Results
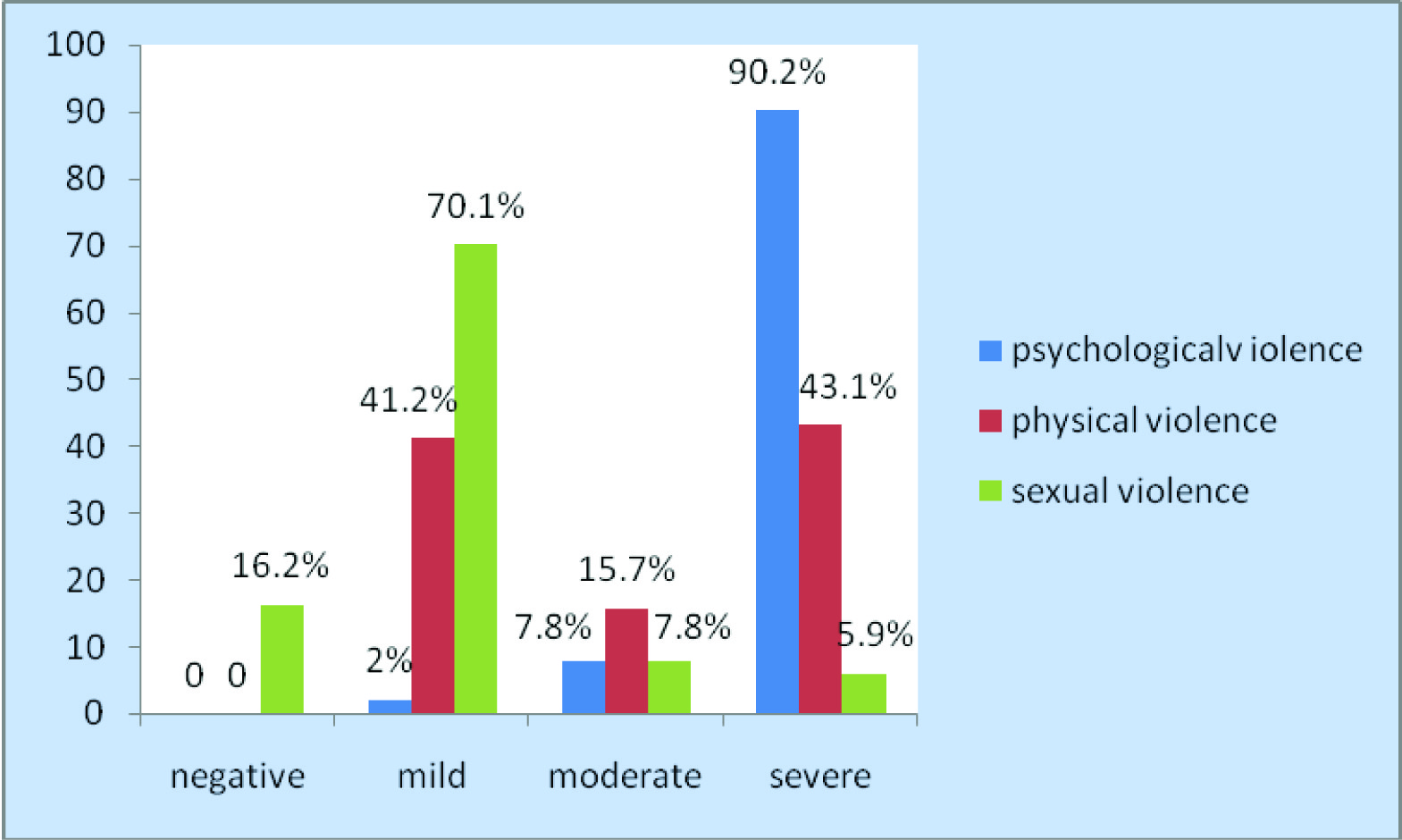
Out of the total 304 women, 204(67.1%) reported domestic violence in some form i.e. psychological, physical or sexual and 100(32.8%) reported no domestic violence. [Table/Fig-1] shows the percentage of subjects who reported psychological, physical and sexual violence. Psychological violence was found to be severe whereas sexual violence was found to be mild in most of the cases.
Percentage of subjects who reported different forms of domestic violence
Sociodemographic information of study population is shown in [Table/Fig-2]. [Table/Fig-3] shows poor oral health behavior among domestic violence group as compared to the non-domestic violence victims. [Table/Fig-4] compares the oral health status of both the groups. Periodontal status of domestic violence group was found to be poor than the non-domestic violence group. 37.3% victims had one or more teeth missing due to injury caused by violence. Dental caries was present in 47.5% victims whereas 36% non-affected had dental caries. (p-value=0.057) Although, the difference was significant, it cannot be fully attributed to domestic violence as dental caries is multifactorial. Furthermore, when the relation of individual psychological ,physical and sexual domestic violence was assessed with oral health status of those with domestic violence, significant correlation was found between psychological domestic violence and Periodontal status (p-value0.000) and physical domestic violence with tooth fracture (p-value=0.001).
Socio demographic information of study subjects
| Variable | Domestic violence group | Non-domestic violence group |
|---|
| Mean Age | 31.96 ±6.21 | 33.75± 6.90 |
| Education | | |
| Illiterate | 92(45.1%) | 13(13%) |
| Middle primary | 68(33.3%) | 21(21%) |
| Higher secondary | 44(21.6) | 56(56%) |
| Graduate | - | 10(10%) |
| Occupation | | |
| Non-Working | 72.5% | 68% |
| Working | 27.5% | 32% |
| Years of marriage | | |
| 5-10years | 7.4% | 20% |
| 11-15years | 51.5% | 56% |
| 16-20years | 26% | 1% |
| ≥20years | 15.1% | 23% |
Comparison of oral health behavior between domestic violence and no domestic violence group
| Oral health behavior | Domestic violence group | No Domestic violence Group | p-value |
|---|
| Oral hygiene aids |
| Finger | 32(15.6%) | 22(22%) | 0.026 |
| Toothbrush | 106(52%) | 60(60%) |
| Neem stick | 66(32.4%) | 18(18%) |
| Frequency of brushing |
| Once | 184(90.2%) | 82(82%) | 0.042 |
| More than once | 20(9.8%) | 18(18%) |
| Past dental visits |
| Never visited | 156(76.5%) | 79(79%) | 0.621 |
| Visited | 48(23.5%) | 21(21%) |
Comparison of oral health status among the domestic violence and non-domestic violence group
| Domestic violence group | No Domestic violence Group | p-value |
|---|
| Max. CPI |
| 1 | 0(0%) | 8(8%) | 0.000 |
| 2 | 52(25.5%) | 56(56%) |
| 3 | 120(58.8%) | 26(26%) |
| 4 | 32(15.7%) | 10(10%) |
| Max. LOA |
| 1 | 123(60.3%) | 88(88%) | 0.002 |
| 2 | 81(39.7%) | 12(12%) |
| Missing due to violence |
| Absent | 128(62.7%) | 100(100%) | 0.00 |
| Present | 76(37.3%) | 0 |
| Fracture |
| Absent | 170(83.3%) | 84(84%) | 0.512 |
| Present | 34(16.7%) | 16(16%) |
| Intraoral injuries |
| Absent | 140(68.6%) | 87(87%) | 0.00 |
| Present | 64(31.4%) | 13(13%) |
| Extraoral injuries |
| Absent | 160(78.4%) | 69(69%) | 0.073 |
| Present | 44(21.6%) | 31(31%) |
| Dental caries |
| Caries free | 107(52.5%) | 64(64%) | 0.057 |
| Caries present | 97(47.5%) | 36(36%) |
Discussion
Violence affects both victims and society at large. The present study depicted a significant impact of domestic violence on the oral health status of the women along with the documented psychological and physical effects. The results indicated that significant proportion of the study population had Psychological violence as the most prevalent form of domestic violence. This could be due to perceived fear and anxiety among the women. Similar results have been cited by Esmina Avdibegovi [7] and Pico Alfonso MA [20]. Also, there is mounting evidence that domestic violence (DV) has long-term negative consequences for survivors, even after the abuse has ended, which can translate into lower health status and lower quality of life [21]. Furthermore, the village backdrop of the study might have contributed to the increased stress factor as the women still lack complete independence in their mental outlook.
Physical component was also evident among the victims of domestic violence similar to the findings of Hendler J Tracey [21].The traumatic dental injuries in the form of dental fractures and tooth avulsions were present in the 16.7% and 37.3% of the subjects that are similar to the findngs of Garbin CA who reported dental trauma in the form of fractures (59.1%), luxations (27.2%) and avulsions (13.7%) in the subjects of domestic violence [17]. Physical consequences of DV extend well beyond the “tell-tale” bruising. The face is a common target in assault and consequently the dental professional has his and her part to play in identifying domestic violence [22]. Dental professionals may observe physical injuries such as chipped or cracked teeth, poor dental hygiene, a broken jaw, a black eye, a broken nose, bruises on the earlobes or chin, and finger marks on the neck, upper arms, or wrists [23].
Sexual component was least reported contrary to the findings of Campbell J [10], which is confluent with the cultural limitations of our country where majority of women still hesitate to discuss their sexual abuse. Most of the women in the domestic violence group were illeterate (45.1%) as compared to the control group where only 13% of the women were illeterate. Similar results were observed in the study by Avdibegovic E [7] where 14.4% abused women received no education as compared to 1.5% non abused women and Contrary results were found in the study by Vachher SA [24] where 81.7% women were literate which can be attributed to the fact that the study was conducted in upper middle colony of Delhi whereas the present study was conducted in the lower socioeconomic strata among the rural population.
When oral health behavior was compared within both the groups it was found that tooth brush was used more by the non domestic violence group and also the frequency of tooth brushing was more than once a day in the same group; the difference being statistically significant. This could be attributed to the fact that domestic violence causes anxiety, depression and stress which could lead to poor oral health behavior as well as poor attitude towards oral health [25].
Dental treatment can be particularly uncomfortable for victims of abuse, due to feelings of loss of control. On assessing the influence of domestic violence on oral health status of the subjects, significant impact was found on periodontal status, introral injuries, fractures of teeth and oral health behavior. In a study by Walker and others, women with a history of trauma reported greater dental fear, and women with high dental fear scores were nearly twice as likely to have been victims of multiple assaults [26]. This could be the possible reason for poor oral health status among domestic violence victims. A muti sectoral approach is the need of the hour to deal with the psychological and physical impact of domestic violence. This should further include long term follow up and assistance from Governmental and non Governmental agencies to improve the current scenario. The primary focus should be on the underlying cultural myths and taboos which encourage domestic violence against married females thus, debilitating their general and oral health. Health care professionals can play a vital role in providing victims with the necessary treatment and referral. They should be dealt sensitively even when oral health care is being provided which can help them raising their morale. The health sector must work with all other sectors including education, legal and judicial, and social services to significantly improve the health of the victims.
Conclusion
The present study creates the need to promote counseling for household women to express their voice against any kind of psychological, physical and sexual abuse. Regular counseling of these women is advocated to improve their status and instill positive attitude among these women. As the epidemic of violence is highly underreported, dentists being primary health care providers have an obligation to intervene. Changes at the national, provincial, educational, public health and private practice levels of dentistry are needed to make identification of DV and intervention a priority. The opportunity for dental professionals to help victims gain access to support and referral services and to provide adequate treatment to them so as to make a positive difference in their lives must not be overlooked. To our knowledge, the present investigation is the first community-based crossectional study that has evaluated the effect of domestic violence on both oral health behavior and oral health status because of which not much literature was available, hence it is recommended that further studies on large scale should be undertaken to assess this relation.
[1]. Hegarty K, What is domestic violence and how common is it?In Intimate Partner Abuse and Health Professionals: New Approaches to Domestic Violence (eds G Roberts, K Hegarty, G Feder) 2006 Elsevier:19-40. [Google Scholar]
[2]. UN General Assembly, Declaration on the Elimination of Violence against Women, 20 December 1993, A/RES/48/104, available at: http://www.refworld.org/docid/3b00f25d2c.html. Updated on 20th December 1993 [accessed 8 January 2014] [Google Scholar]
[3]. Krug EG, Mercy JA, Dahlberg LL, Zwi AB, Lancet. The World Report on Violence and Health 2002 360(9339):1083-88. [Google Scholar]
[4]. Europe C of Council of Europe Convention on preventing and Combating Violence against Women and Domestic Violence and Explanatory Report, Istanbul, Turkey: 11.v.2011, Cets. Council of Europe;2012 [Google Scholar]
[5]. Shireen JJ, Wife-Beating in Rural India: A Husband’s Right?Evidence from Survey Data by Economic and Political Weekly 1998 33(15):855-62. [Google Scholar]
[6]. Duvvury N, Domestic violence in India: A summary report of three studies 1999 Washington, DCInternational center for research on women:1-58. [Google Scholar]
[7]. Avdibegovic E, Sinanovic O, Consequences of Domestic Violence on Women’s Mental Health in Bosnia and HerzegovinaCroat Med J 2006 47:730-41. [Google Scholar]
[8]. Scholle SH, Rost KM, Golding JM, Physical abuse among depressed womenJ Gen Intern Med 1998 13:607-13. [Google Scholar]
[9]. Astin MC, Lawrence KJ, Foy DW, Posttraumatic stress disorder among battered women: risk and resiliency factorsViolence Vict 1993 8:17-28. [Google Scholar]
[10]. Campbell J, Jones AS, Dienemann J, Kub J, Schollenberger J, O’Campo P, Gielen AC, Wynne C, ’Intimate partner violence and physical health consequences’Arch Intern Med 2002 162(10):1157-63. [Google Scholar]
[11]. Guth AA, Pachter LH, ’Domestic violence and the trauma surgeon’Am J Surg 2000 179(2):134-40. [Google Scholar]
[12]. Coker AL, Sanderson M, Fadden MK, Pirisi L, ’Intimate partner violence and cervical neoplasia’J Womens Health Gend Based Med 2000 9(9):1015-23. [Google Scholar]
[13]. Sutherland CA, Bybee DI, Sullivan CM, ’Beyond bruises and broken bones: the joint effects of stress and injuries on battered women’s health’Am J Community Psychol 2000 30(5):609-36. [Google Scholar]
[14]. Friedlander AH, Mahler ME, Major depressive disorder. Psycho-pathology, medical management and dental implicationsJ Am Dent Assoc 2001 132(5):629-38. [Google Scholar]
[15]. Marques-Vidal P, Milagre V, Are oral health status and care associated with anxiety and depression? A study of Portuguese health science studentsJ Public Health Dent 2006 66(1):64-6. [Google Scholar]
[16]. Abel S, Kowal CH, Brimlow D, Uchin M, Gerbert B, A Collaboration to Enhance Oral Health Care for Survivors of Domestic Violence: Women’s Domestic Violence Shelters and Nova Southeastern University’s College of Dental MedicineJ Dent Educ 2011 76(10):1334-41. [Google Scholar]
[17]. Garbin CA, Guimarães e Queiroz AP, Rovida TA, Garbin AJ, Occurrence of traumatic dental injury in cases of domestic violenceBraz Dent J 2012 23:72-6. [Google Scholar]
[18]. Prasad BG, Changes proposed in Social classification of Indian familiesJ Indian Med Assoc 1970 55:198-99. [Google Scholar]
[19]. World Health Organization. WHO Multi-country Study on Women’s Health and Domestic Violence against Women: Summary Report of Initial Results on Prevalence, Health Outcomes and Women’s Responses. Geneva, Switzerland: World Health Organization. 2005:13-16 [Google Scholar]
[20]. Pico-Alfonso MA, Garcia-Linares MI, Celda-Navarro N, Blasco-Ros C, Echeburúa E, Martinez M, The impact of physical, psychological, and sexual intimate male partner violence on women’s mental health: depressive symptoms, posttraumatic stress disorder, state anxiety, and suicideJ Womens Health (Larchmt) 2006 15(5):599-611. [Google Scholar]
[21]. Hendler JT, Sutherland ES, Domestic Violence and its Relation to Dentistry: A Call for Change in Canadian Dental PracticeJ Can Dent Assoc 2007 73(7):617a-f. [Google Scholar]
[22]. Coulthard P, Warburton A, Dentistry and Domestic violenceBr Dent J 2006 201(10):611 [Google Scholar]
[23]. Berrios DC, Grady D, “Domestic Violence: Risk Factors and Outcomes,”Western J Med 1991 155(2):133-35. [Google Scholar]
[24]. Vachher SA, Sharma AK, Domestic Violence against Women and Their Mental Health Status in a Colony in DelhiIndian J Community Med 2010 35(3):403-05. [Google Scholar]
[25]. Dumitrescu AL, Gârnea L, Guzun O, Anxiety, stress, depression, oral health status and behaviours in Romanian hemodialysis patientsRom J Intern Med 2009 47(2):161-18. [Google Scholar]
[26]. Walker EA, Milgrom PM, Weinstein P, Getz T, Richardson R, Assessing abuse and neglect and dental fear in womenJ Am Dent Assoc 1996 127(4):485-90. [Google Scholar]