A Rare Case of Adult Acquired Tracheo-Oesophageal Fistula with Sub-Glottic Stenosis for Corrective Surgery- An Anesthetic Challenge
Smita Joshi1, Anitha Kulkarni2, Roopa S Holkunde3
1 Professor, Department of Anaesthesia, Padmashree Dr.D Y Patil Medical College, Pune, India.
2 Lecturer, Department of Anaesthesia, Padmashree Dr.D Y Patil Medical College, Pune, India.
3 Postgradute, Department of Anaesthesia, Padmashree Dr.D Y Patil Medical College, Pune, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Roopa S Holkunde, C/o Mr Shivkumar Yekkele, No 306 H block Dwaraka Vishwa Society Indrayaninagar, Bhosari Sector -7 , Pune-411026, India. Phone : 08149687103, E-mail : roopa_sh1@yahoo.co.in
Acquired trachea-esophageal fistula (TEF) is a rare condition in adults and causative factors include malignancy, trauma and various iatrogenic causes. The important causative factor of TEF in our case was percutaneous tracheostomy. The normal protective laryngeal reflexes are lost in TEF due to the patent tract from the airway to the upper gastrointestinal tract.
The TEF poses a challenge for the surgeon and the anaesthesiologist, as the fistula lies in close proximity to oesophagus, trachea, upper mediastinal contents and large blood vessel. Here we present a rare case of anesthetic management of a 26 year old male patient with complaints of regurgitation of part of swallowed food particles through an in-situ tracheostomy tube since two years.
Acquired TEF, Montgomery T tube, Sub-glottic stenosis, Tracheostomy tube
Case Report
A 26-year-old male patient came with complaints of regurtitation of food partly through tracheostomy tube since two years. Patient had suffered road traffic accident with head injury two years ago and was intubated and ventilated for 20 d and later tracheostomized. He was on metal tracheostomy tube at the time of admission to hospital. In spite of repeated regurgitation he was able to cough out GI contents. This prevented him from aspiration and subsequent development of any upper respiratory tract infections.
On admission to our hospital metal tracheostomy tube was replaced with 7mm portex cuffed tracheostomy tube.
On Examination: Patient was averagely built and well nourished, conscious, comfortable, and could speak clearly by closing tracheostomy tube [Table/Fig-1]. Patient was on nasogastric tube no.14 in-situ. On examination his vital parameters were pulse rate was 78/minute, blood pressure 110/74mmhg and respiratory rate 18/minute. His Spo2 was maintained 100% on room air on auscultation of lungs, bilateral air entry was equal and no added sounds were noted. Other systemic examination findings were within the physiological normal limit. Patient MPC was grade I. Chest X-ray showed the metal tracheostomy tube in-situ with sub-glottic stenosis above tracheostomy tube more evident in lateral view [Table/Fig-2,3].

Chest x-ray showing level of tracheostomy tube
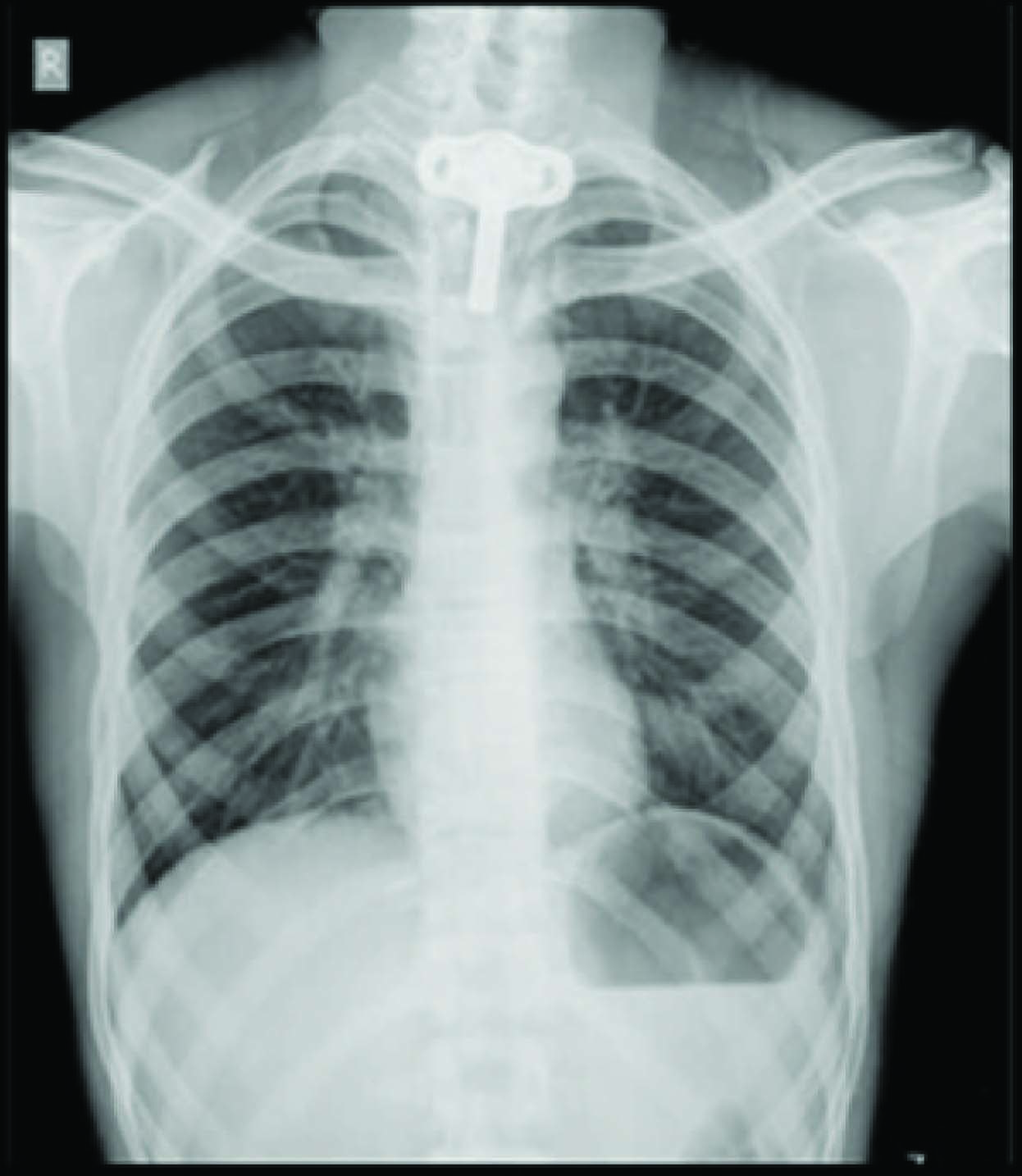
Level of sub glottis stenosis

Direct and video laryngoscopy confirmed sub-glottic stenosis with tiny aperture. Oesophagoscopy confirmed trachea-oesophageal fistula 19cms from incisors approximately 2-2.5cms long (tracheostomy tube could be seen through the defect). CT-scan showed a suspicious communication, seen in lower part of neck between trachea and esophagus.
Patient was posted for repair of fistula and sub-glottic stenosis under ASA grade II.
Anesthetic Management: In pre-anesthetic room, two 20’G IV cannulae were secured. In the theatre, non- invasive blood pressure (NIBP), electrocardiogram (ECG), pulseoximeter (SpO2) monitors were attached.
Pre-medication: with Ondansetron 4mg, Glycopyrrolate 0.2mg, Midazolam 1mg, Fentanyl 50μcg.
Pre-oxygenation -100%oxygen (O2) via Bain’s circuit through tracheostomy tube for three minutes. Induction- propofol 140mg and vecuronium 4mg. Patient ventilated with 100% O2 for three minutes, anaesthesia was maintained with cuffed tracheostomy tube after checking bilateral air-entry, and cuff was inflated.
Maintenance of Anaesthesia- O2: N2O (nitrous oxide), isoflurane and intermittent top-ups of fentanyl and vecuronium, via Bain’s circuit on manual ventilation. During the closure of fistula, the tracheostomy tube was removed and a sterile cuffed flexometallic tube no.7 was passed through the tracheostoma and distal end of flexometallic tube was fixed on patient’s chest with suture (prevent endo-bronchial intubation), after confirming bilateral equal air entry [Table/Fig-4].
Fixation of sterile flexometallic tube,
This was to facilitate surgeons to operate, by removing the tube out intermittently, with a period of apnea (2-3 min), [Table/Fig-5] monitoring SpO2 throughout. Before removing the flexometallic tube, ventilation was done with only 100% O2 for three minutes with additional propofol and vecuronium, to avoid hypoxia, light plane of anaesthesia and coughing.
Intermittent removal of flexometallic tube for closure of fistula,

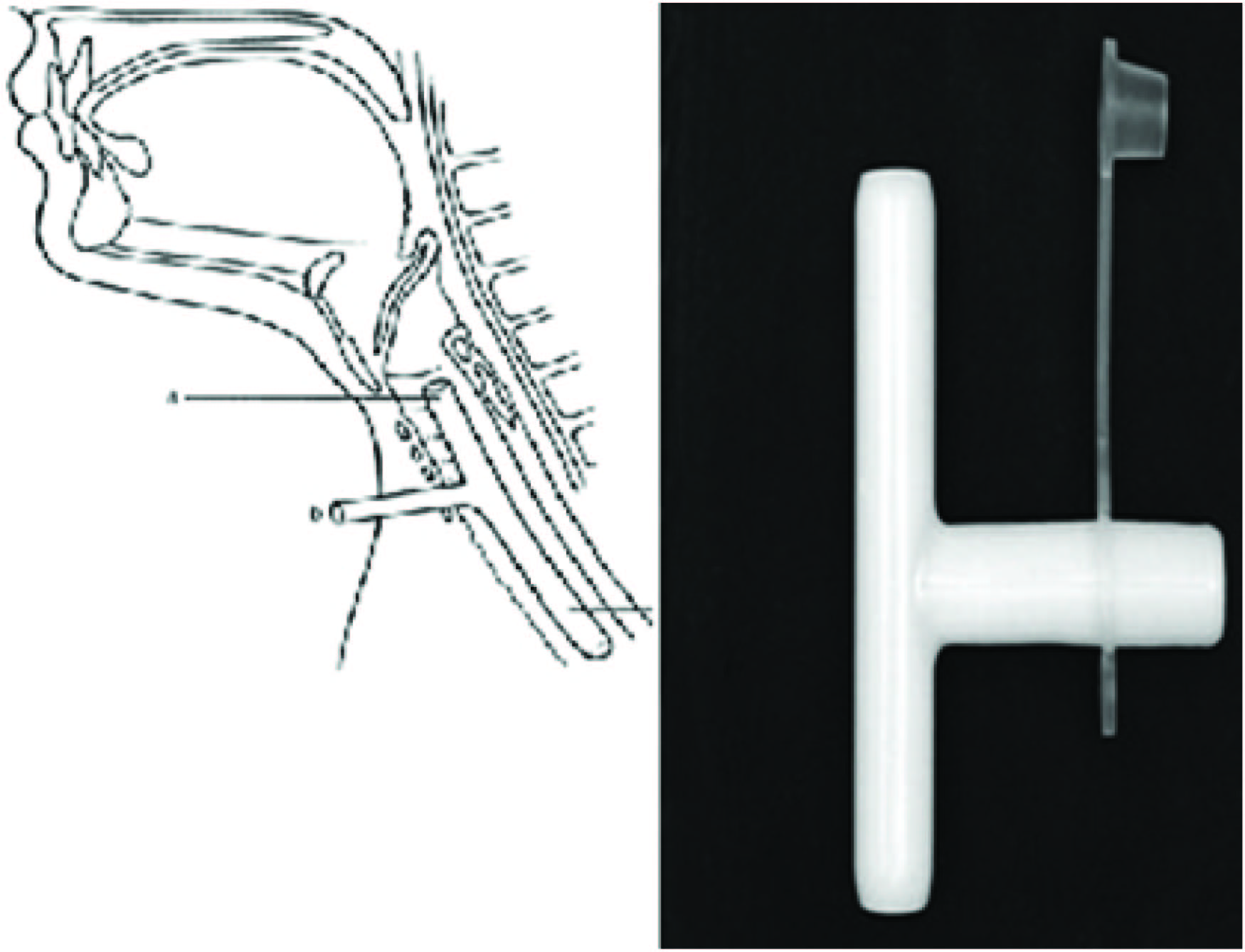
During these periods of intermittent apnea (7-8 times) the fistula was closed. Intermittent disconnection of anaesthesia circuit to aid closure of fistula, could lead to hypoxia, which was prevented by oxygenation before removal. The repair of sub-glottic stenosis and the Montgomery t-tube [Table/Fig-6] insertion was done in a period of apnea by Shiann Yann Lee technique by surgeons, after removing flexometallic tube. Ventilation and anaesthesia was carried out with short laryngeal part (a) after closing the extra-tracheal part (b) with cap provided. Before closure of trachea, part (a) of t-tube was packed with a sterile 10’F Foley’s catheter balloon which was passed orally by direct laryngoscopy through the cords and balloon was inflated to occlude the upper intratracheal limb [Table/Fig-7].
Diagrammatic positioning of Montgomery T-tube
Post insertion of Montgomery T-tube, upper end occluded with foley’s catheter

Ventilation was subsequently carried out through part (b) via a 5.5mm tracheal tube connector.
Isoflurane, fentanyl and vecuronium were with-held 20 min prior to end of surgery and patient’s respiratory attempts were observed. Patient was allowed to wake up after reversal of residual neuromuscular block with neostigmine 2.5mg and glycopyrrolate 0.4mg.
Foleys balloon was deflated and catheter was removed. At this juncture extratracheal part of the T-tube was plugged. Thus, allowing normal respiration via the intratracheal part through the larynx.
Discussion
An adult acquired tracheoesophageal fistula is a rare condition, as the chances of survival are less because there is high mortality due to aspiration and pulmonary sepsis [1]. But in our case, surprisingly the patient could cough out the regurgitant GI contents, which prevented him from pulmonary aspiration and infections [2].
Reported mechanisms of tracheal injury include: traumatic and prolonged intubation, airway suctioning, and vascular compression of the tracheal wall due to prolonged endotracheal and tracheostomy tube cuff over- inflation [1]. This results in ischemia, pressure necrosis and tissue damage leading to ulceration and formation of subsequent fistula [3]. So, timely tracheostomy is necessary. As our patient’s TEF was at the level of C7 and cuffed tracheostomy tube was beyond the fistula, we were not worried about gastric dilatation and so patient was maintained on controlled ventilation. The patient was hemodynamically stable throughout.
To aid surgeons to locate and repair the fistula, it was necessary that the tracheostomy tube be replaced by flexometallic tube and period of apnea was necessary.
The sterile flexometallic tube was fixed with suture distally and during repair it was pulled out, before which oxygenation with 100% O2 along with top-ups of inj.propofol and vecuronium was given. Thus, taking care that the patient was not in light plane of anaesthesia and did not cough during repair.
Anesthetic Challenges faced in this case were because of
A. Shared Airway
B. Montgomery T-Tube
A. Sharing of the Airway
Intermittent apneic periods during the closure of the fistula could have caused hypoxia, hypercarbia and atelectasis. To avoid these, continuous monitoring of SpO2 and EtCO2 are mandatory. Handling of the airway may lead to tracheal and laryngeal oedema and bleeding.
Intraoperative Modes of Ventilation:-
Controlled Ventilation to have quiet surgical field and to prevent hypoxia.
Spontaneous Ventilation has a risk of laryngospasm and bronchospasm and was avoided to prevent hypoventilation of both the lungs.
High Frequency Jet Ventilation: may have a possibility of barotrauma.
B. Montgomery t-tube
It is a silicon T-tube with silicon plug, used for supporting the reconstructed segment of stenotic trachea [4]. It is available in sizes 4.5 to 16.0 mm (external diameter). The silicon plug (extra-tracheal part) can be opened for suctioning and in case of supraglottic airway obstruction. Because of its unique design it doesn’t have standard connectors [5]. Loss of inspired gases through upper intratracheal limb can lead to hypoventilation and inadequate depth of anaesthesia. So this limb has to be blocked by either balloon of Foley’s catheter or Fogarty embolectomy catheter or with ribbon gauze [6]. As the tube is soft there are chances of misplacement of upper and lower limb and kinking leading to complete loss of airway.
Conclusion
A detailed discussion with the surgical team prior to surgery will avoid the potential problems due to sharing of the airway. We did this in our case and thus avoided problems due to sharing of the airway.
[1]. Didee R, Shaw IH, Acquired trachea esophageal fistula in adults continuing education in anaesthesiaCritical care and pain 2006 6:105-08. [Google Scholar]
[2]. Shah CP, Yeolekar ME, Pardiwala FK, Acquired trachea esophageal fistulaJ Post graduate Medicine 1994 40:83-84. [Google Scholar]
[3]. Kaur D, Anand S, Sharma P, Kumar A, Early presentation of post intubation trachea esophageal fistula : Peri operative anaesthetic managementJournal of Anaesthesia and clinical Pharmacology 2012 28:114-16. [Google Scholar]
[4]. Kulkarni VR, Kelkar VS, Salunkhe SA, Anaesthetic challenges of Montgomery t-tube insertion in a patient with fasciscapulo humeral dystrophyIndian Journal of Anaesthesia 2005 49:502-04. [Google Scholar]
[5]. Agarwal S, Payal YS, Montgomery t-tube:anesthetic managementJ clin anaesth 2007 19:135-37. [Google Scholar]
[6]. Kerai S, Gupta R, Wadhavan S, Bhadoria P, Aanaesthetic management of a patient with Montgomery t tube in situ for direct laryngoscopyJournal of Anaesthesia and clinical Pharmacology 2013 29(1):105-07. [Google Scholar]