Mobile phone users are at risk of developing various repetitive strain injuries (RSI) type of conditions to the soft tissues due to repetitive use of the phone in text messaging. RSI can manifest as musculoskeletal pain which can be described as any pain that may involve the muscles, nerves, tendons, ligaments, bones or joints [1–5]. Musculoskeletal problems of the upper limb and especially the thumb has been reported in mobile phone users due to text messaging [6–8]. There have been isolated cases reported of “texting tendinitis”, playstation thumb and Wittis [9–17] all these studies have reported De Quervain’s as a result of text messaging on mobile phones, in these patients based on clinical examination.
Repetitive movements of the thumb can produce symptoms of De Quervain’s disease with pain over the radial styloid and tender swelling of the extensor compartment [18,19], But sometimes extensor pollicislongus (EPL) tenosynovitis whose symptoms were very similar to De Quervain’s disease may also be present. Case reports of EPL tenosynovitis presenting as De Quervain’s disease has been reported [20–24]. But no study has been done to investigate the changes that may occur in the soft tissues of these two compartments or the other muscles of the thumb that may be involved because of excessive use of the mobile phone text messaging.
Hence, the aim of this study was to document any involvement of the thumb muscles and note the subclinical changes that may occur in these two compartments of the thumb with excessive text messaging on the mobile phones in subjects who were found to have thumb pain because of text messaging.
Materials and Methods
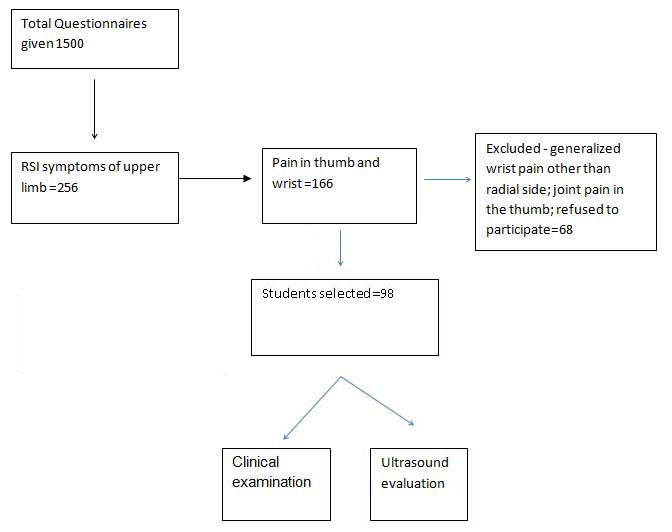
The study was approved by the Institutional Research Committee and the Institutional Ethical Committee.A preliminary survey was done to find the prevalence of RSI type of symptoms of upper limb among students who were regular mobile phone users. All the students between the age of18-29 years were included. Those who had recent injury (less than six months) to the hand or upper limb or were suffering from any inflammatory, degenerative or neuromuscular conditions of the hand or upper limb affecting the usage of the limb for activities of daily living were excluded from the survey. The questionnaire was given to 1500 students. This sample size was calculated based upon a pilot study done to find the prevalence of RSI in mobile phone users, where prevalence was found to be 21%. The flow of participants finally included in the study is shown in [Table/Fig-1]. Ninety eight students were finally included for the ultrasound evaluation. Other causes of thumb pain like recreational activities involving hand and computer keyboard use was excluded by personal interview.
Flow of participants through the study
Age and sex matched controls without any thumb pain and who were regular users of the phone were also subjected to ultrasound evaluation. Informed consent was taken from all the subjects before the evaluation.
Special tests like Finkelstein test and resisted movements for thumb abduction and extension were done. Tenderness was checked at the radial styloid. Lateral and tip pinch strengths were measured bilaterally between thumb and index fingers, using a JAMAR®Hydraulic Pinch Gauge (SammonsTM Preston) for both the groups. Manual functions of the participants were measured using the Disabilities of the Arms, Shoulder and Hand (DASH) questionnaire. Pain was recorded on a Numerical pain rating scale (NPRS).
The ultrasound evaluation was carried out by a radiologist with special interest in musculoskeletal imaging. The radiologist was totally blinded to the clinical findings of the partcipants.The machine used for the purpose was Voluson 730 Expert Series (3D -4D capabilities) with a high frequency probe of 12 MHz for dedicated muscular skeletal imaging. The thumb was examined in transverse and longitudinal orientations, both at rest and dynamically. For each hand, tendons on the radial side of the hand were examined in transverse and longitudinal orientations, both at rest and dynamically. To take into account both acute and degenerative tendon changes, the following ultrasonography findings were recorded: (1) nonhomogeneity of tendinous bundle echotexture; (2) thickening of the tendinous bundle; and (3) anechoic halo around any one tendon.
Ultrasound evaluation was done for the involvement of the following tendons:
APL-abductor pollicis, EPB-extensor pollicisbrevis, EPL-extensor pollicislongus
FPL-flexor pollicislongus and Thenar eminence.
Statistical Analysis
Mann Whitney U-test was used to analyse the number of messages sent by the cases and controls as the variation in the standard deviation was large. Severity of pain (0-10 NPRS) and the number of messages were reported as median with interquartile ranges as the standard deviation was high. Differences between the cases and controls were calculated using 2-tailed independent t-tests for comparing pinch strengths. Descriptive data of each variable was summarized as percentages p<0.05 was considered significant for all the tests.
Results
The number of messages sent per day was significantly more in the cases = 55, (2-200) than in the controls which was 15 (0-150), Za=6.9,p=0.00
On NPRS, pain was reported by the cases from 0 to 8 with the median at 4 and interquartile range of three.
Clinical examination
Tenderness was found in the wrist in 18.8% cases but no swelling was seen in the extensor compartments. Finkelstein test was positive in 40% of the cases. Resisted movements were tested for abduction and extension of the thumb and were painful to one movement in 21% and positive to both the movements in 34% of the subjects. Both tip and lateral pinches were significantly reduced in the cases as compared to the controls [Table/Fig-2]. Functional outcome scale DASH was within normal range with a score of 10.2.
Pinch strength variations between the cases and the controls
| Pinch/ Group | N | Mean± Std. Deviation | t | p |
| Lat (r) Pinch |
| Cases | 98 | 12.9±4.1 | 2.3 | .02* |
| Controls | 98 | 14.2±4.2 |
| Tip (r) Pinch |
| Cases | 98 | 9.3±3.6 | 3.1 | .002* |
| Controls | 98 | 10.9±3.9 |
* - Significant at p<0.05
r=right, Lat = lateral pinch, Tip = tip pinch, N = number of participants
Ultrasound evaluation
It showed presence of fluid around the dorsal compartments in 19 subjects (19%). In addition to this, fluid was also seen around the flexors of the thumb in two subjects [Table/Fig-3] therefore, in total ultrasound showed involvement of the tendons in 21 subjects which is 1/5 of the total.
Results of the ultrasound analysis of the cases
| Area involved | Frequency |
|---|
| 1st Dorsal compartment | 11 |
| 3rd Dorsal compartment | 7 |
| Around the flexor tendons | 2 |
In the control group, 107 subjects agreed to undergo ultrasound evaluation. It was negative for any findings for all these subjects.
Discussion
Repetitive and/or forceful thumb movements can aggravate or cause cumulative trauma disorders like EPL tenosynovitis and de Quervain’s tenosynovitis [18–25]. Tenosynovitis of the tendons in the first dorsal compartment of the wrist , the extensor pollicis brevis and abductor pollicis longus, was first mentioned in the thirteenth edition of Gray’s Anatomy in 1893 and subsequently in 1895 de Quervain published a report of five cases of chronic tenovaginitis in the first dorsal compartment [26] De Quervains disease, is a common condition affecting the hand/wrist with prevalence ranging from 0.5% to 1.3 % in the general population [27]. Sometimes symptoms of tenosynovitis of extensor pollicislongus, may mimic De Quervain’s disease because it may cross the first dorsal compartment [20,21].
According to classification by Harrington, the diagnostic criteria for De Quervain’s disease includes pain over the radial styloid and tender swelling of the extensor compartment and either pain produced by resisted thumb extension or positive Finkelstein test. According to another classification system both the movements (abduction and extension) should be checked in addition to Finkelstein test [28]. In our study, Finkelstein test was found to be positive in 40%. Resisted movements were tested for abduction and extension of the thumb and were painful to one movement in 21% and positive to both the movements in 34% of the subjects. On diagnostic ultrasound 1st compartment showed peritendinous fluid in 11% of the cases [Table/Fig-4]. Tender swelling of the extensor compartment was not noted in any case. Forget N and Piotte F have noted in their study that Finkelstein test was positive in the asymptomatic hand of patients with unilateral De Quervain’s disease without meeting all the diagnostic criteria of De Quervain’s disease.This they attributed to the generalized inflammatory response after a few weeks of a repetitive reaching and grasping activities. This systemic response increases the inflammatory susceptibility of tissues in the contralateral limb, where previously harmless tissue insults could lead to an acute inflammatory response and thus producing a positive Finkelstein test [18]. It has also been seen that repetitive movements of the thumb can produce localized soft tissue inflammatory responses causing pain [19]. These two mechanisms may be the cause of the high percentage of Finkelstein test being positive in our study. Another reason could be the involvement of EPL in 7% of our cases as seen on ultrasound [Table/Fig-5], which produced a positive Finkelstein’s test. Sometimes Extensor pollicis longus tenosynovitis may mimic de Quervain’s disease because of its course through the first extensor compartment distally. The clinical presentation is similar to that of de Quervain’s disease [20,21]. Though tenosynovitis of the first dorsal compartment, or De Quervain’s disease, is a common hand problem, only a few cases of tenosynovitis of the extensor pollicis longus (EPL), or third compartment, have been reported in the literature [22–24]. This is an unusual condition that may be difficult to diagnose initially [24]. Simultaneous passive flexion of the thumb at the carpometacarpal and metacarpophalangeal joints does not cause pain; however, when the interphalangeal (IP) joint of the thumb is then passively flexed, there is severe pain along the EPL sheath. The diagnosis of EPL tenosynovitis can then be made. Thus, mobile phone users complaining of thumb pain may not only have involvement of the first dorsal compartment but also the third dorsal compartment as evidenced by ultrasound investigation. This is a new finding and it stresses that in addition to doing the Finkelstein test for thumb pain in cell phone users, special tests should also be done to rule out involvement of EPL.
Ultrasound image of peritendinous fluid in the first dorsal compartment.

Ultrasound image of peritendinous fluid in the third dorsal compartment

Most of the previous studies have clinically reported tendinitis, witis etc but no ultrasonic evaluation was done to confirm the clinical findings. Hence, there is no evidence to say as to which tendons are actually involved. This study clearly shows that on ultrasonic investigation tendon involvement was confirmed in the form of fluid present around the tendons of the first and third extensor compartments in19% of the cases. In addition fluid was also seen around the flexor tendons which suggest that subclinical changes are present in the tendons of the thumb in a substantial number of subjects.
Pinch strength measurements are often used clinically to quantify weakness of the thumb [18], and are a useful determinant of thumb function [29]. Measurement of lateral pinch is a standard procedure for the evaluation of hand function as well as for impairment assessment [30] and is also considered the strongest of the pinches. In our study, the lateral pinch was found to be significantly different between the cases and controls. We also checked the tip pinch as we hypothesized that it will simulate the position of messaging on the phone and a highly significant difference was noted in the tip pinch between the two groups. The decrease in the lateral and tip pinches in the cases shows that the strength of the thumb was decreased. This is in accordance with other studies [18]. Since in our cases involvements of both the first and third compartments were seen, these two pinches can be used in the evaluation of thumb strength. DASH was within normal limits and indicates that it did not cause major difficulty in functions of daily living. But this study clearly shows that excessive use of cell phones for text messaging can lead to obvious clinical and subclinical changes in the muscles of the thumb.
Limitations of Our Study
The design of the phones used by the subjects was not taken into account in this study and the different types of phone types could have had an influence in the presentation of symptoms in these subjects.
Key Points
Excessive text messaging causes damage to the third compartment in addition to the first compartment of the wrist extensors.
EPL should be evaluated in subjects complaining of thumb pain with excessive use of mobile phones.
Ultrasound imaging can detect subclinical changes in the tendons of the thumb in subjects with thumb pain with text messaging.