Context: Drug-drug interactions(DDIs) are significant but avoidable causes of iatrogenic morbidity and hospital admission.
Aim: To detect potential drug-drug interactions among medications received by hypertensive patients.
Materials and Methods: Patients of both sex and all adult age groups, who were attending medicine out -patient department (OPD) of a tertiary care teaching rural hospital since last six months and were being prescribed antihypertensive drug/s for essential hypertension, were selected for the study. Hypertensive patient with co-morbities diabetes mellitus, ischemic heart diseases, congestive heart failure, and chronic renal diseases were also included in the study. Potential drug drug interactions were checked with medscape drug interaction software.
Results: With the help of medscape drug interaction software, 71.50% prescriptions were identified having atleast one drug-drug interaction. Total 918 DDIs were found in between 58 drug pairs. 55.23% DDIs were pharmacodynamic, 4.79% pharmacokinetic type of DDIs. 32.24% DDIs were found affecting serum potassium level. 95.42% DDIs were found significant type of DDIs. Drug drug interaction between atenolol & amlodipine was the most common DDI (136) followed by metoprolol and amlodine (88) in this study. Atenolol and amlodipine ( 25.92%) was the most common drugs to cause DDIs in our study.
Conclusion: We detected a significant number of drug drug interaction in hypertensive patients. These interactions were between antihypertensive agents or between hypertensive and drug for co-morbid condition.
Introduction
Drug–drug interactions (DDIs) are an emerging threat to public health. They may present with harmful outcomes, resulting in about 2.8% of all hospitalizations in older patients and an estimated cost of more than U$1 billion per year, to government exchequer health care systems [1-3]. Previous studies [4,5] which were mainly centered around patients of emergency departments and hospital wards showed that the cardiovascular drugs were the most common culprits to cause DDIs. The present study however intends to examine drug-drug interactions DDIs among medications prescribed to the hypertensive patients but in an outpatients setting. It will be prudent to mention here, that literature pertaining to the same, (in the recent years) is extremely scarce, if not nonexistent, to the best of our knowledge.
Hypertension is an important public health challenge all across the globe. Raised blood pressure is one of the leading behavioural and physiological risk factor to which about 13% of all global deaths are attributed. Hypertension is reported to be the fourth largest contributor to the premature deaths occurring in developed countries and seventh in developing ones [6]. High blood pressure, in a significant number of patients is not controlled by one medication alone; therefore, to achieve therapeutic goal of blood pressure(<140/90 mmHg, or <130/80 mmHg for patients with diabetes or chronic kidney disease) ,multiple antihypertensive drugs are prescribed by the physicians. Besides this, drug therapy for other co-morbid conditions such as diabetes mellitus, myocardial infarction, congestive cardiac failure and chronic kidney disease, which are much frequent with hypertension, make drug-drug interactions(DDI) inevitable.
In 2007, a meta-analysis of 23 clinical studies from around the world revealed that drug–drug interactions (DDIs) cause approximately 0.054% of emergency room visits, 0.57% of hospital admissions, and 0.12% of rehospitalizations [7]. There are 136.1 million emergency room visits [8] and 34.1 million hospital discharges uly2 [9] in the USA alone each year. If these percentages are correct, Americans experience DDI events serious enough to send them to the emergency room almost 74 000 times per year, and hospitals admit nearly 195 000 patients per year because of DDIs. Unsurprisingly, DDIs also contribute to increased cost and duration of hospital stays [10].
This study was conducted to find out potential drug drug interactions medications prescribed to hypertensive patients.
Materials and Methods
This was an observational, cross section study conducted in a tertiary care teaching hospital of central Gujarat, India. The study was conducted over a period of one year from August 2012 to August 2013 after approval from Institutional Ethics Committee. Total 899 patients were enrolled in the study. Patients were included from all the three medicine units equally to prevent bias. Patients of both sex and all adult age groups, who were attending medicine out -patient department (OPD) since last six months and were being prescribed antihypertensive drug/s for essential hypertension, were selected for the study. Hypertensive patients with co-morbidities diabetes mellitus, ischemic heart diseases, congestive heart failure and chronic renal diseases were also included in the study. Patients with hypertensive emergency and cerebral stroke were excluded from this study. Patient with any concurrent acute medical condition e.g. acute myocardial infarction, acute left ventricular failure etc were excluded from this study.
The diagnosis and line of treatment to be given were decided by the physician. No additional drugs or investigations were advised by us during the study period. Data of patients matching inclusion criteria were recorded. Before including in the study, patients were explained about the aspects of research work. Written informed consent was taken from each patient before including him or her into the study. Identity of patient was kept confidential.
To analyze drug- drug interaction, software namely medscape drug interaction checker (URL- http:// reference.medscape.com/drug-interaction checker) [11]- freely available on the website www. medscape.com was used.
Clinical relevance was defined according to the criteria used by the DDI-checker software programs, which considered the ‘potential’ of DDIs for both adverse event risk and lack of efficacy. All DDIs were classified as minor, significant and serious clinical relevance on the basis of potential clinical outcomes and type, quality, and relevance of supporting clinical and pharmacological documentation. In serious type of DDIs, use of alternative drug is advocated. While in significant type of DDIs, pharmacotherapy is advised to monitor closely. Sample size was calculated based upon other studies [12,13] .
Results
Medscape drug interaction checker [11] was applied to detect potential drug-drug interaction. In this study, 120 patients were prescribed only one drug. Therefore, number of patients who were at risk of potential drug-drug interaction was 779. With the help of software, 557(71.50%) prescription were identified having atleast one DDI [Table/Fig-1].
In these 557 patients, total 918 potential drug-drug interactions were detected with the help of medscape drug interaction checker software. These interactions were of total 86 types and were between 58 drugs pairs. There were total 34 such drug pair which potentially showed one DDI. Remaining 24 drug pairs potentially showed more than one DDI. Out of these, 21 drug pairs showed two DDIs, and two drug pairs showed three DDI. Maximum DDI between one drug pair was four which was in between carvedilol and digoxin. Three potential DDI were detected with the software between drug pair aspirin- losartan and digoxin-hydrochlorothiazide. In this study, most common drug pair to cause DDIs was found atenolol- amlodipine drug pair (136) followed by metoprolol – amlodipine drug pair (88). Both drug pairs showed only one DDI between respective drugs according to software. Next three common drug pairs to cause potential DDIs were found- aspirin- atenolol, aspirin-enalapril and metformin- hydrochlorothiazide. These drug pairs showed 56, 52 and 48 DDIs respectively [Table/Fig-2].
Medscape drug interaction software classified total 918 potential DDIs into three categories- minor, significant and serious. Out of 918 DDIs, 28 were of minor type and seen in three drug pairs while 14 were of serious type and seen in three drug pairs. Drug pairs which showed minor type of DDIs had aspirin as a one drug. Drug pair which showed serious type of DDI were in between ACE inhibitor and angiotensin receptor blocker drug. Rest of the DDIs were significant type [Table/Fig-3].
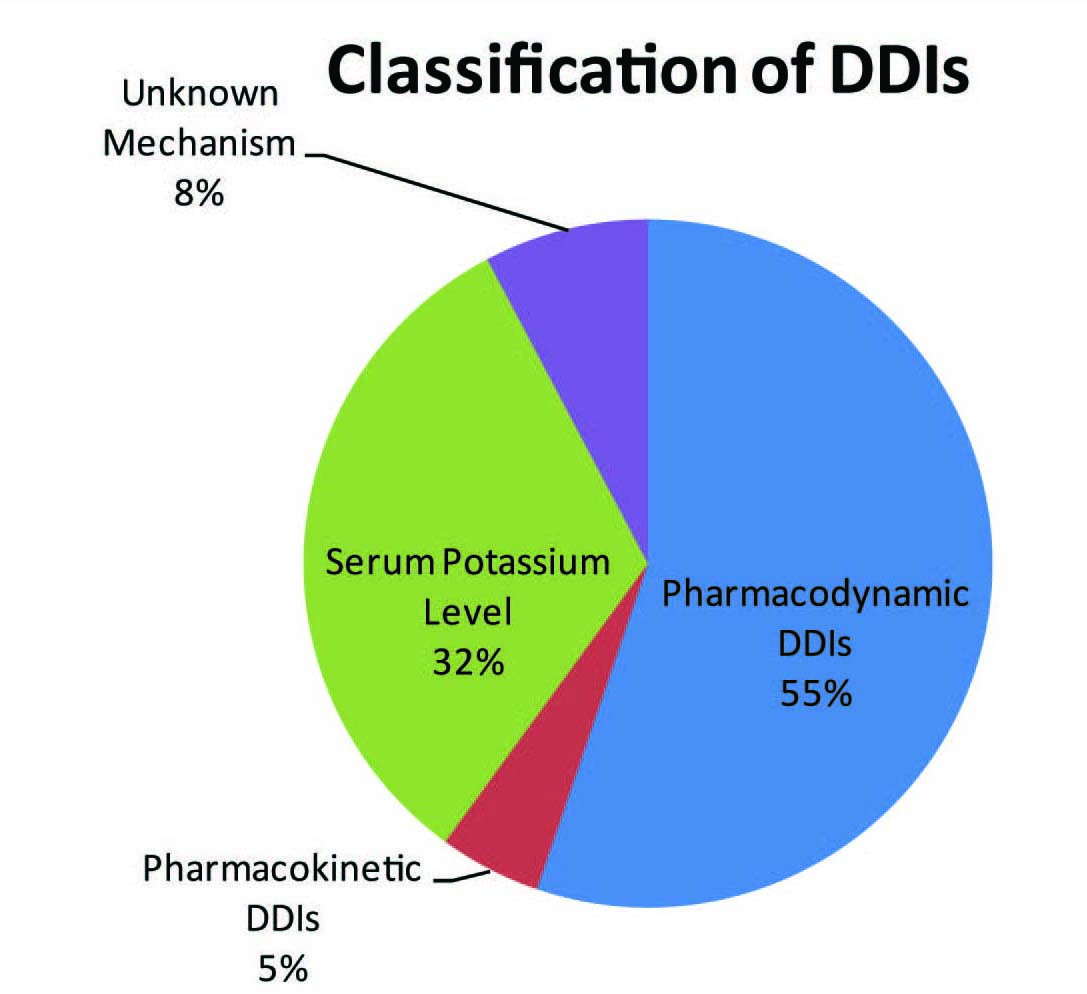
Medscape drug interaction checker software detected 55.23% pharmacodynamic type of DDIs out of 918 DDIs. Next common DDIs was affecting serum potassium level (32.24%). DDIs having unknown mechanism were 71 (7.73%) and pharmacokinetic DDIs were only 44 (4.79%) [Table/Fig-4].
Out of 507 pharmacodynamic DDIs, 366 were synergistic type while 141 were of antagonistic type. Majority of synergistic pharmacodynamic DDIs, the software found, were between beta blocker- calcium channel blocker (CCB) drug pair and beta blocker- angiotensin receptor blocker (ARB) drug pair. Beta blocker and CCB both increase anti-hypertensive property of each other [Table/Fig-5].
Aspirin caused maximum number of pharmacodynamic type of antagonism. It showed antagonism with atenolol, enalapril, metoprolol and furosemide in 28, 26, 21 and 18 frequencies respectively [Table/Fig-6].
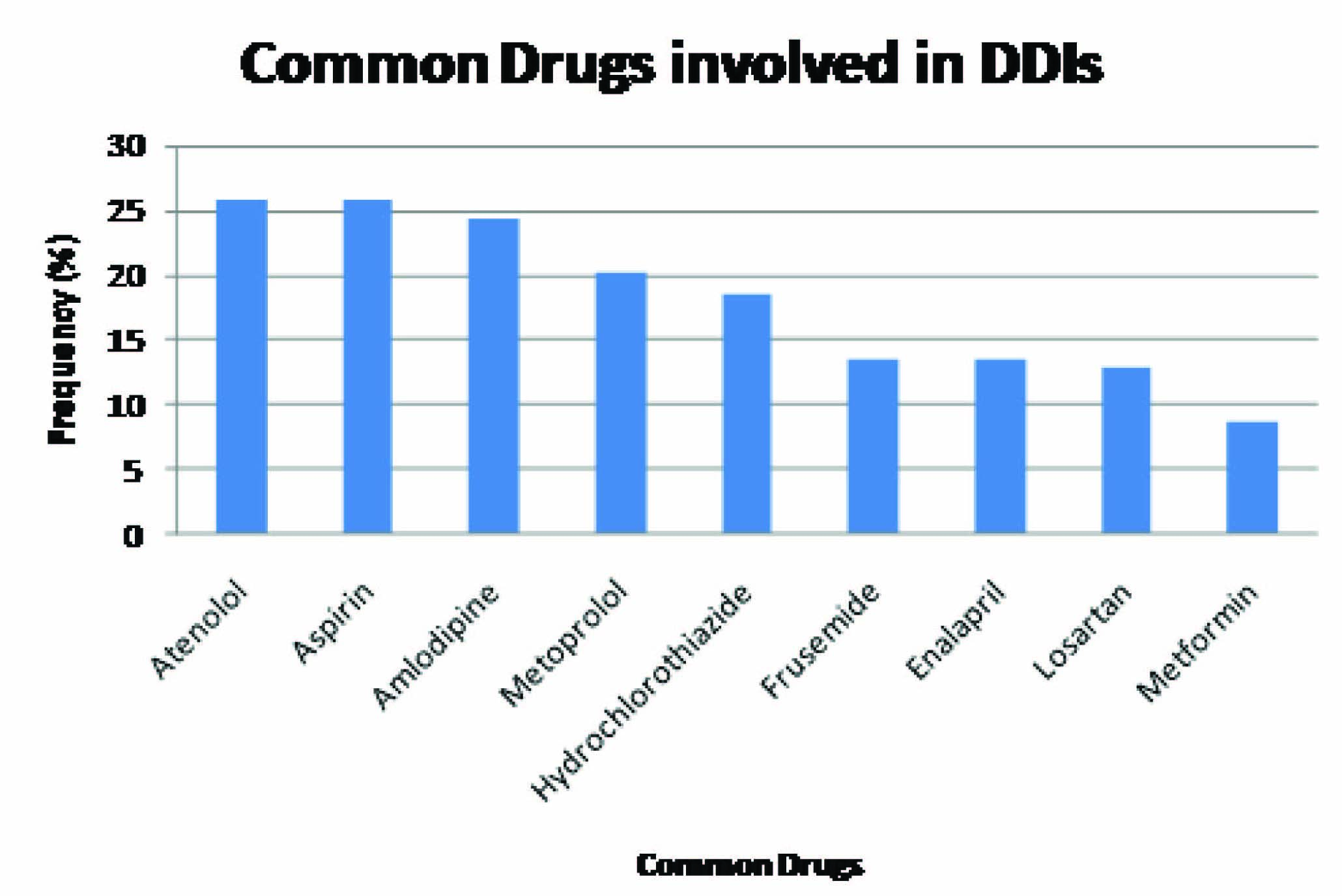
In this study, software found atenolol and aspirin as the most common drugs to cause DDIs. Each one of them caused 238 DDIs. Amlodipine was involved in 224 DDIs while metoprolol, hydrochlorothiazide,frusemide, enalapril and metformin was involved in 185,170,124, 123 and 80 DDIs respectively [Table/Fig-7].
Discussion
Drug interaction refers to modification of response to one drug by another when they are administered simultaneously or in quick succession. The modification is mostly quantitative, i.e. the response is either increased or decreased in intensity [14].
In this study, we detected potential DDIs with the help of medscape drug interaction checker software [11]. Medscape is a reputed online portal from WebMD that is a part of of WebMD Health Professional Network that includes the Heart.org and eMedicine.com [11]. Other studies conducted at Sweden [12] and Nepal [13], software FASS computer program and micromedex electronic source were used respectively.
In our study, prevalence of DDIs (71.50%) was detected much than found by Bjorkman et al., (41.50 %) [13]. It is may be attributed to the fact that because cardiovascular drugs are the most common drugs to cause DDIs [4,5] and DDIs were checked solely here only in patients taking antihypertensive drugs.
The possibility of drug interaction rises whenever a patient concurrently receives more than one drug, and the chances increase with the number of drugs taken [12]. In present study patients at risk of developing DDIs, were prescribed on average 3.54 drugs which is lesser than the average number of drugs prescribed in study by Bjorkman conducted at Sweden (7.0) [13].
In this study, patients’ mean age was 63.50 year that developed potential DDI. This was similar to studies in US [14,15], which showed mean age to be more than 60 y. In this study, most common drug group involved in potential DDIs was the beta blocker (46.07%); diuretics were involved in 32.08% of DDIs. Study conducted by Bjorkman [13] at Sweden, although it did not involved only hypertension cases, showed diuretics were involved in 46% of DDIs while beta blocker caused 11% DDI.
Maximum DDIs between one drug pair were four which was in between carvedilol and digoxin. Between carvedilol- digoxin, two DDI were pharmacokinetic type, one pharmacodynamic type and one was related to increase of serum potassium level. Three potential DDI were detected with the software between drug pair aspirin- losartan and digoxin-hydrochlorothiazide. Between aspirinlosartan, one DDI was pharmacodynamic type, second related to serum potassium level and third was of increasing toxicity of the either drug by unknown mechanism. Between digoxinhydrochlorothiazide, one DDI was pharmacokinetic, second was pharmacodynamic and third was related to serum potassium level. Drug pair which showed serious type of DDI were in between ACE inhibitor and angiotensin receptor blocker drug. Both ACE inhibitor and ARB cause blockade of renin- angiotensin system and increase risk of hypotension, hyperkalemia and renal impairment [14].
In this study, majority of the DDIs were of pharmacodynamic type (55.23%). Study done in Austria- found similar results [16]. These types of interactions derive from modification of the action of one drug at the target site by another drug, independent of a change in its concentration. This may result in an enhanced response (synergism), an attenuated response (antagonism) or an abnormal response [12]. In this study, 366 out of 507 pharmacodynamic DDIs were of synergistic type while 141 were of antagonistic type.
Few synergistic antihypertensive drug combinations are recommended by JNC-VIII guidelines [17]. Among them, combination ARB+ diuretics and beta blocker + diuretic are found in this study; were prescribed in 76 prescriptions and 73 prescriptions respectively. ARB, being a vasodilator, causes fluid retention which is counteracted by diuretic if given concurrently. ARB also reduced plasma renin activity which is increased by concurrently given diuretic [18]. Potency of hypotensive action of beta blocker increases when it is combined with diuretic [19].
In this study, beta blocker- amlodipine was the commonest drug combinations to be prescribed which have opposite effect on plasma renin activity that is beneficial for the patient to keep ADR in check [18].
In this study, atenolol and aspirin both caused similar number of DDIs (25.92%). Study conducted by Bista D et al., [4] also found aspirin was the most common drug causing DDIs. It is expected from aspirin because aspirin increases serum potassium level andserum potassium level is altered by almost all antihypertensive drugs including ACE inhibitors, ARBs, BB and diuretics.
Number of patients who were prescribed more than one drug
| Number of drugs in prescription | No of patients | Total drugs prescribed |
| 2 | 206 | 412 |
| 3 | 185 | 555 |
| 4 | 198 | 792 |
| 5 | 143 | 715 |
| 6 | 31 | 186 |
| 7 | 16 | 112 |
| Total | 779 | 2772 |
Drug pair showing potential drug- drug interactions
| S. No. | Drug pair | Frequency |
| (i) Drug pair which have one DDI b/w partner drugs |
| 1 | Atenolol- Amlodipine | 136 |
| 2 | Metoprolol- Amlodipine | 88 |
| 3 | Hydrochlorothiazide- Losartan | 31 |
| 4 | Atenolol- Hydrochlorothiazide | 23 |
| 5 | Enalapril- Frusemide | 20 |
| 6 | Atenolol- Chlorthalidone | 2 |
| 7 | Atenolol- Frusemide | 16 |
| 8 | Atenolol-Torsemide | 2 |
| 9 | Metoprolol- Chlorthalidone | 3 |
| 10 | Metoprolol- Frusemide | 4 |
| 11 | Hydrochlorothiazide- Valsartan | 15 |
| 12 | Hydrochlorothiazide- Telmisartan | 14 |
| 13 | Chlorthalidone- Losartan | 11 |
| 14 | Chlorthalidone- Valsartan | 2 |
| 15 | Chlorthalidone- Telmisartan | 3 |
| 16 | Enalapril- Losartan | 14 |
| 17 | Enalapril- Telmisartan | 1 |
| 18 | Enalapril- Torsemide | 4 |
| 19 | Ramipril- Losartan | 10 |
| 20 | Ramipril- Valsartan | 3 |
| 21 | Ramipril- Frusemide | 12 |
| 22 | Ramipril- Torsemide | 2 |
| 23 | Carvedilol- Frusemide | 4 |
| 24 | Metformin- Chlorthalidone | 6 |
| 25 | Glimepiride- Enalapril | 11 |
| 26 | Glimepiride- Ramipril | 11 |
| 27 | Glimepiride- Hydrochlorothiazide | 2 |
| 28 | Glipizide- Enalapril | 16 |
| 29 | Glipizide- Ramipril | 5 |
| 30 | Pioglitazone+ Hydrochlorothiazide | 2 |
| 31 | Aspirin- Torsemide | 4 |
| 32 | Digoxin- Enalapril | 5 |
| 33 | Digoxin- Ramipril | 1 |
| 34 | Metoprolol- Hydrochlorothiazide | 20 |
| (ii) Drug pair which have two DDI b/w partner drugs |
| 35 | Atenolol- Losartan | 15 |
| 36 | Aspirin- Atenolol | 28 |
| 37 | Aspirin – Enalapril | 26 |
| 38 | Metformin-Hydrochlorothiazide | 24 |
| 39 | Aspirin- Metoprolol | 21 |
| 40 | Atenolol- Valsartan | 4 |
| 41 | Atenolol- Telmisartan | 4 |
| 42 | Metoprolol-Losartan | 7 |
| 43 | Metoprolol- Valsartan | 4 |
| 44 | Metoprolol-Telmisartan | 2 |
| 45 | Carvedilol- Losartan | 1 |
| 46 | Carvedilol- Valsartan | 1 |
| 47 | Metformin- Frusemide | 13 |
| 48 | Aspirin – Ramipril | 11 |
| 49 | Aspirin- Hydrochlorothiazide | 6 |
| 50 | Aspirin- Chlorthalidone | 4 |
| 51 | Aspirin- Frusemide | 18 |
| 52 | Digoxin-Atenolol | 1 |
| 53 | Digoxin-Metoprolol | 1 |
| 54 | Digoxin- Valsartan | 1 |
| 55 | Digoxin- Frusemide | 3 |
| iii) Drug pair which have three DDI b/w partner drugs |
| 56 | Aspirin- Losartan | 2 |
| 57 | Digoxin- Hydrochlorothiazide | 1 |
| (iv) Drug pair which have four DDI b/w partner drugs |
| 58 | Digoxin-Carvedilol | 4 |
Classification of DDIs according to their severity
| S.No. | DDI | Frequency |
| (i) Minor DDI |
| 1 | Aspirin- Chlorthalidone | 4 |
| 2 | Aspirin- Frusemide | 18 |
| 3 | Aspirin- Hydrochlorothiazide | 6 |
| (ii) Serious DDI |
| 1 | Enalapril- Telmisartan | 1 |
| 2 | Ramipril- Losartan | 10 |
| 3 | Ramipril- Valsartan | 3 |
| (iii) Significant DDI |
Drug pairs showing pharmacodynamic synergism
| Drug pair | Frequency |
| Beta Blocker + CCB | 224 |
| Atenolol- Amlodipine | 136 |
| Metoprolol- Amlodipine | 88 |
| Beta Blocker + ARB | 46 |
| Atenolol- Losartan | 15 |
| Metoprolol-Losartan | 15 |
| Atenolol-Valsartan | 4 |
| Metoprolol- Valsartan | 4 |
| Atenolol- Telmisartan | 4 |
| Metoprolol- Telmisartan | 2 |
| Carvedilol- Losartan | 1 |
| Carvedilol-Valsartan | 1 |
Drug pair showing pharmacodynamic antagonism
| Drug pair | Frequency |
| Aspirin- Atenolol | 28 |
| Aspirin-Enalapril | 26 |
| Metformin- Hydrochlorothiazide | 24 |
| Aspirin-Metoprolol | 21 |
| Aspirin-Frusemide | 18 |
| Aspirin-Ramipril | 11 |
Common drugs involved in DDI’s
Limitation
There were some limitations of this study. We have collected data from only one institute, therefore population is relatively homogenous. We included hypertensive patients only co-morbid with diabetes mellitus, ischemic heart disease, chronic heart failure and chronic kidney disease. The utilization of DDI-checker software provides only a ‘potential’ estimate of DDI occurrence. This approach cannot be taken into account whether the potential DDI produced an adverse event or negatively influenced the therapeutic effect of a drug. However, despite these limitations, this approach is currently widely used to assess the clinical relevance and risk of exposure to potential DDIs.
Conclusion
Knowledge of the prevalence and predictors of clinically important potential DDIs will help physicians and pharmacists identify patients at higher risk of DDI-related adverse drug reactions, who require more cautious pharmacotherapy management to avoid negative outcomes.
[1]. MU Shad, C Marsh, SH Preskorn, The economic consequences of a drug–drug interactionJ Clin Psychopharmacol 2001 21:119-20. [Google Scholar]
[2]. RA Hamilton, LL Briceland, MH Andritz, Frequency of hospitalization after exposure to known drug-drug interactions in a Medicaid populationPharmacotherapy 1998 18:1112-20. [Google Scholar]
[3]. MT Grymonpre, PA Mitenko, DS Sitar, FY Aoki, PR Montgomery, Drug-associated hospital admissions in older medical patientsJ Am Geriatr Soc 1998 36:1092-98. [Google Scholar]
[4]. D Bista, A Saha, P Mishra, S Palaian, PR Shankar, Pattern of potential drugdrug interactions in the intensive care unit of a teaching hospital in Nepal: a pilot studyJournal of Clinical and Diagnostic Research 2009 3:1713-16. [Google Scholar]
[5]. J Doucet, P Chassagne, C Trivalle, Drug-drug interactions related to hospital admissions in older adults: a prospective study of 1000 patientsJ Am Geriatr Soct 1996 44:944-48. [Google Scholar]
[6]. Third Indian Guidelines on Hypertension (IGH)- IIIhttp://www.sjapi.org/february_2013_special_issue_hypertension_guideline/06_epidemiology_of_hypertension.html [Cited 2013, October 14] Available from [Google Scholar]
[7]. ML Becker, Hospitalisations and emergency department visits due to drug–drug interactions: a literature reviewPharmacoepidemiol. Drug Saf 2007 16:641-51. [Google Scholar]
[8]. Centers for Disease Control/National Center for Health Statistics (2010) National Hospital Ambulatory Medical Care Survey 2009, Centers for Disease Control/National Center for Health Statistics. [Google Scholar]
[9]. MJ Hall, National hospital discharge survey: 2007 summaryNatl Health Stat Repc 2010 29:1-20. [Google Scholar]
[10]. CS Moura, Drug–drug interactions associated with length of stay and cost of hospitalizationJ Pharm Pharm Sci 2009 12:266-72. [Google Scholar]
[11]. Drug interaction checker, computer program. NewYork: Medscape. Available from URL :http://reference.medscape.com/drug-interactionchecker cited 2013, 3 [Google Scholar]
[12]. IK Björkman, J Fastbom, IK Schmidt, CB Bernsten, The Pharmaceutical Care of the Elderly in Europe Research (PEER) Groupa. Drug–Drug Interactions in the ElderlyAnn Pharmacother 2002 36:1675-81. [Google Scholar]
[13]. JF Kurfees, RL Dotson, Drug interactions in the elderlyJ Fam Pract 1987 25:477-88. [Google Scholar]
[14]. KD Tripathi, Drug interaction. Essentials of medical pharmacologyJ Am Dent Assoc 2013 7th EditionDelhiJaypee:928-34. [Google Scholar]
[15]. AJ Costa, Potential drug interactions in an ambulatory geriatric populationFam Pract 1991 8:234-36. [Google Scholar]
[16]. J Schuler, C Dückelmann, W Beindl, E Prinz, T Michalski, M Pichler, Polypharmacy and inappropriate prescribing in elderly internal-medicine patients in AustriaThe Middle European Journal of Medicine. 2008 120:733-1. [Google Scholar]
[17]. AV Chobanian, GL Bakris, HR Black, WC Cushman, LA Green, JL Izzo, The seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. The JNC 7 reportJAMA 2003 289:2560-72. [Google Scholar]
[18]. T Michel, BB Hoffman, Treatment of Myocardial Ischemia and Hypertension. In: Brunton LL, Chabner BA, Knollman BC. editors. Goodman & Gillman's –The Pharmacological Basis of Therapeutics 2011 12th EditionNew YorkMc Graw Hill:745-88. [Google Scholar]
[19]. TA Kotchen, Hypertensive vascular disease. In: Longo DL, Kasper DL, Jameson JL, Fauci AS, Hauser SL, Loscalzo J. ed.. Harrison's Principles of InternalMedicine 2012 18th EditionNew YorkMc Graw Hill:2042-59. [Google Scholar]