Background: Hypertensive disorders in pregnancy (HDP) complicate 3-10% of all pregnancies. Though there are several biochemical parameters which aid in predicting hypertension of pregnancy, human placental alkaline phosphatase (PLAP), synthesized in placenta during pregnancy by placental syncytiotrophoblast, assumes diagnostic relevance. The purpose of this study was to compare the total alkaline phosphatase (ALP) and heat stable placental alkaline phosphatase (PLAP) levels in the serum of normotensive and hypertensive disorders of pregnancy and to evaluate the clinical utility of ALP and PLAP as a reliable, sensitive, specific and economical biochemical marker of HDP.
Materials and Methods: This was a case control study, carried out on pregnant women with hypertension, of south Indian population.
Study included pregnant women, 60 patients with hypertension and 60 controls. Biochemical assays were carried out by the IFCC approved procedures based on spectrophotometric method and using fully automated random access chemistry analyser.
Data was compared by using student t-test. ROC was drawn to find out optimum cut off for ALP, PLAP and PLAP/ALP ratio in HDP. Pearson’s correlation was performed to ascertain the association among markers.
Results: Serum total ALP, PLAP and PLAP/ALP ratio levels were significantly higher in hypertensive pregnant women when compared to controls (p<0.05). There was significant correlation among ALP, PLAP and DBP. ROC analysis of ALP (169.5), PLAP (69) and PLAP/ALP (0.44) ratios showed optimum cut-offs in diagnosis of hypertension in pregnancy.
Conclusion: Serum heat stable ALP isoenzyme and PLAP/ALP ratio could be useful adjuvant markers in diagnosis of HDP in association with other relevant and economically viable biochemical tests.
Introduction
Hypertensive disorders in pregnancy (HDP) are one among the leading direct obstetric causes of maternal mortality worldwide, accounting for about 14% of maternal deaths [1]. HDP accounts 7-10% of all antenatal admission in India [2]. The prevalence of gestational hypertension and comorbidity increases with advancing age [3]. Hypertension in pregnancy is defined as a systolic blood pressure ≥ 140 OR diastolic blood pressure ≥ 90 mmHg or both. HDP comprise a spectrum of disorders Categorised into Gestational hypertension defined as new hypertension presenting at or after 20 wk gestation without proteinnuria or other features of preeclampsia, preeclampsia is hypertension with significant proteinuria, when preeclampsia develops in women with chronic hypertension, the classification is chronic hypertension with superimposed preeclampsia and eclampsia, chronic(pre-existing) hypertension is hypertension that is present before 20 wk of of gestation or prior to pregnancy [4,5]. Several biochemical parameters Viz; serum albumin, total protein, iron, iron binding capacity, hemoglobin, ferritin, uric acid, Magnesium, aminotransferases, total ALP, PLAP and urinary protein had been cited in the past which find wide use in predicting pregnancy hypertension. In recent years, however certain novel biochemical substances such as prostaglandins, Inhibin, Cell Adhesion Molecules have been shown to possess clinical relevance in monitoring the course and outcome of hypertensive disorders of pregnancy. There are studies showing a raised serum uric acid levels in HDP compared to normal pregnant women. Increase in uric acid is considered as predictor of severity of disease [6]. In spite of several research, causes for the development of the disease and the economical best marker for diagnosis of HDP remains vague till date. Several studies have documented preeclampsia as a disease of placenta and the best mode to treat is to deliver the placenta [7].
Several Alkaline phosphatase (ALP) isoenzymes are elaborated in human tissues including placental isoform and as independent genetic loci [8,9].
The existence of four human isoenzymes, each encoded by independent genetic loci, has been well documented and includes an intestinal isoenzyme, localized in the brush border of the mucus membrane. A second isoenzyme, derived from placental syncytiotrophoblasts, appears in the second trimester. Placental like ALP (tissue nonspecific), includes enzymes originating from bone, liver, lung, and leukocytes [10].
The primary source of human placental Alkaline Phosphatase (PLAP) is the syncytiotrophoblastic plasma membranes, during the second & third trimesters of pregnancy. As gestation progresses, the concentration of PLAP rises till term and this can be caused by the detachment of ALP from the membrane into the maternal circulation [11,12].
In normal pregnant women it rises to a level 2-3 times higher than that of non pregnant women and do possess a long half life (seven days postpartum) [13].
The placental-type human ALP, which often occurs in human non-trophoblastic tumours, has been considered a marker for malignant transformation. Yet, the appearance of this heat-stable enzyme is not universal for human tumours, many of which may produce heat-labile ALP enzymes [14].
Till date, studies on placental alkaline phosphatase (heat stable fraction) as a marker in diagnosis of HDP in Puducherry population are sparse. Hence, we undertook this study in order to compare the activities in HDP with normal pregnancy and to assess their diagnostic utility as reliable and economical biochemical markers of pregnancy induced hypertension (PIH).
Materials and Methods
The present study was carried out in the Department of Biochemistry in association with the Department of Obstetrics and Gynaecology, Mahatma Gandhi Medical College and Research institute between January 2010 and July 2011, 120 patients (60 hypertensive women and 60 normotensive women) were recruited into the study. The study was a clinical based case control study and was carried out after obtaining a clearance from Institute human ethical committee and informed consent from each study subjects in their local language. Inclusion criteria for HDP: pregnant women with a blood pressure of ≥ 140/90 mmHg, which included patients in all the category of HDP according to NHBPEP classification [5]. Inclusion criteria for control: 60 healthy pregnant women with no history of pregnancy related complications, diabetes mellitus or any other chronic medical illness. Five subjects in the control group were not considered for statistical analysis since three patients had anemia and two of them had premature rupture of membranes. The age of the study groups was between 18 and 35 years and their gestational ages were between 36 and 40 week(peak PLAP rise is between 34 and 40 week of gestation).
Exclusion criteria: Pregnant women with Diabetes mellitus, Jaundice, chronic liver disorders, anaemia and other pregnancy associated disorder like gestational diabetes mellitus, complicated pregnancies (vaginal bleeding after 28 wk, fetal distress and congenital abnormalities) were excluded.
Five ml of blood sample (from both normal and hypertensive mothers) was collected in a plain vacutainer. The individual samples were centrifuged at 1200 rpm for 10 min and the separated serum was used for the analysis of Alkaline Phosphatase - ALP (Total), Placental alkaline phosphatase - (PLAP) and uric acid. The biochemical assays were carried out using procedures approved by the IFCC [15,16]. The analyses were essentially carried out on the same day within four hours so as to minimise the inactivation of ALP by denaturation.
Alkaline phosphatase [15] and uric acid [16] in serum was estimated based on a spectrophotometric method by a fully automated random access chemistry analyser.
The initial values obtained without heat inactivation pertained to the serum total ALP activity. Serum PLAP (heat stable fraction of ALP) was measured by the thermal inactivation method [17].
0.5 ml of sera samples were added into small thin walled glass tubes placed in thermostatically controlled water bath stabilised at 650C. The water level was at least 3 cm above the samples. Exactly following 30 minutes, the serum tubes were rapidly removed and placed in an ice bath for 3 min before returning it to room temperature. The ALP activities of the processed samples were determined similar to that of total ALP and this represented the heat stable fraction of ALP (PLAP).
Statistical Analysis
The data was analysed using the SPSS software, version 17. The values were expressed as mean and standard deviation. The independent Students t-test was performed to compare the mean values in hypertension and normotensive pregnant women. Pearson’s correlation analysis was performed to ascertain the association between various test parameters. A p-value of < 0.05 was considered to be significant. Receiver operating curves (ROCs) were drawn to elicit the optimum sensitivity, specificity and cut-off values. The sample size was calculated by using the Master 2.0 software, CMC, Vellore, India with a power of 80%.
Results
As compared to the control group, the patients with hypertension disorders of pregnancy were found to have significantly high levels of serum ALP, PLAP and uric acid with p-values of <0.001. The ratio of PLAP/ALP was significantly higher in hypertensive disorders of pregnancy with p-values of <0.001 [Table/Fig-1]. Pearson’s correlation analysis was performed to assess the association between the various test parameters in the case group. It has been depicted in [Table/Fig-2] that there were significant positive correlation of serum PLAP with ALP, DBP, PLAP / ALP ratio and MAP in hypertensive disorders of pregnancy with p-values of <0.05.
Comparison of parameters between Cases and Controls
| Parameter | Hypertensives n =60 | Normotensive n =55 | ‘p’ values |
|---|
| Mean | ±SD | Mean | SD | |
|---|
| Systolic BP (mmHg) | 154.47 | ± 11.14 | 114.98 | ± 7.3 | < 0.001 |
| Diastolic BP (mmHg) | 102 | ± 9.3 | 73.8 | ± 6.2 | <0.001 |
| PLAP (U/L) | 169.8 | ± 52.4 | 93.8 | ± 17.4 | <0.001 |
| ALP (U/L) | 286 | ± 72.16 | 206.13 | ± 39 | <0.001 |
| PLAP/ALP | 0.6 | ± 0.2 | 0.45 | ± 0.01 | <0.001 |
| Uric Acid mg/dl | 5.1 | ±1.10 | 3.7 | ±0.7 | <0.001 |
Mean and S.D of blood pressure and biochemical parameters in Cases and control. ; Data represented are mean ± SD. Independent T- test was used to analyse the data. ; Systolic BP- systolic blood pressure, Diastolic BP- Diastolic blood pressure, PLAP- Placental alkaline phosphatase, ALP- Alkaline phosphatase and PLAP/ALP ratio- Placental alkaline phosphatase/ Alkaline phosphatase
Correlation analyses of serum PLAP and uric acid with other parameters
| Parameters | ‘r’ value | ‘p’ value |
|---|
| PLAP | Vs DBP | 0.726 | <0.05 |
| PLAP | Vs ALP | 0.793 | <0.05 |
| PLAP | Vs PLAP/ALP ratio | 0.649 | <0.05 |
| PLAP | Vs Uric acid | 0.381 | <0.05 |
| PLAP | Vs MAP | 0.886 | <0.05 |
| Uric acid | Vs DBP | 0.788 | <0.05 |
| Uric acid | Vs MAP | 0.826 | <0.05 |
Pearson correlation analysis was performed; p < 0.05 considered significant. PLAP- Placental alkaline phosphatase, ALP – Alakaline phosphatase, DBP- Diastolic blood pressure, MAP- Mean arterial blood pressure
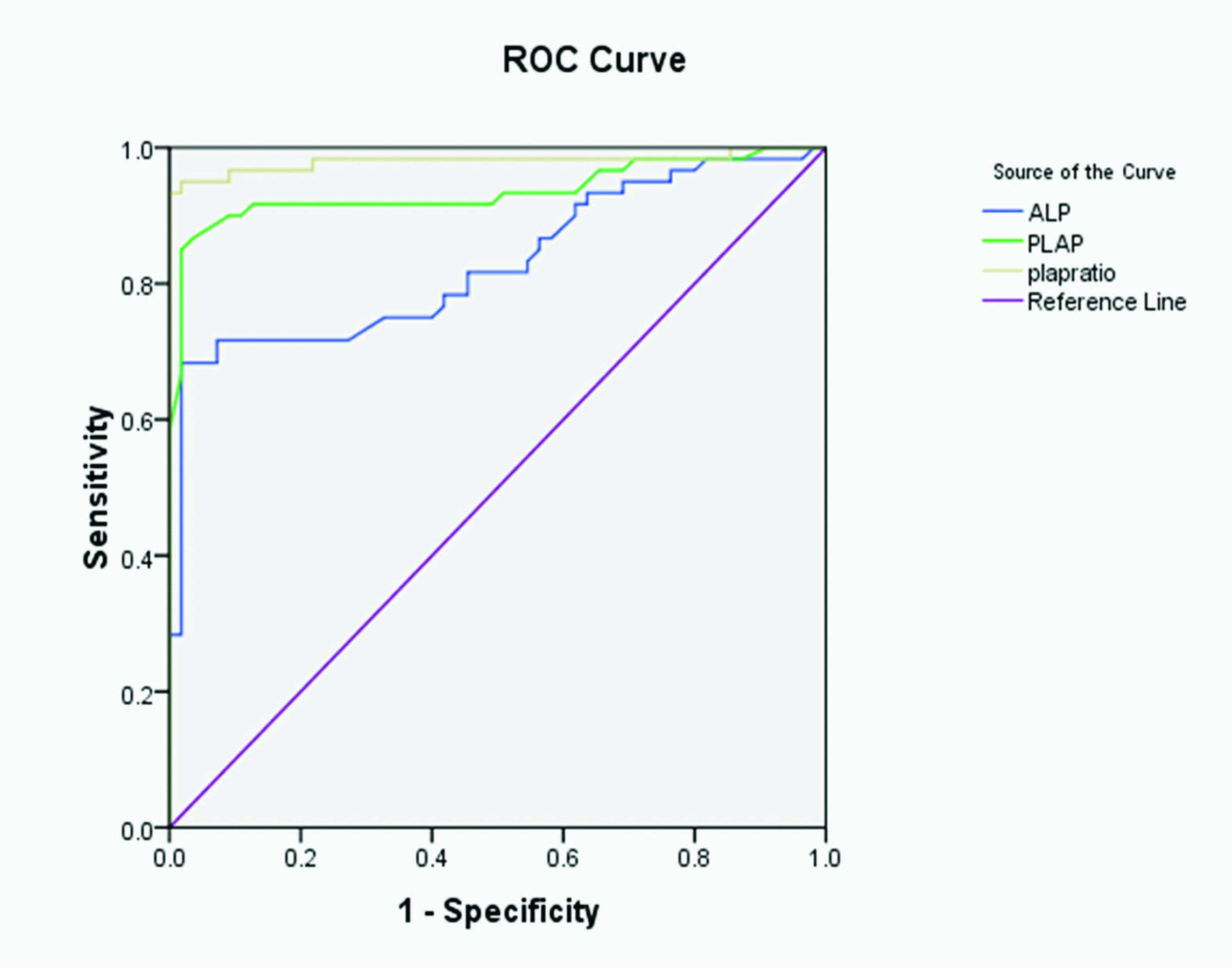
[Table/Fig-3]. The Receiver Operating characteristic curve (ROC) of PLAP/ALP ratio showed an optimum cut off at 0.44 with 100% sensitivity and 98% specificity, with a significant area under the curve (AUC=0.980). The PLAP showed an optimum cut off at 69 with 100% sensitivity and 90% specificity, with a significant area under the curve(AUC = 0.935). The ROC of ALP showed an optimum cut off at 169.5 with significant area under the curve (AUC = 0.829) in patients with hypertensive disorders of pregnancy [Table/Fig-4].
ROC of ALP, PLAP and PLAP/ALP ratio.
ROC of ALP, PLAP and PLAP/ALP ratio
| Parameters | Optimum cutoff | sensitivity | specificity | AUC |
|---|
| ALP | 169.5 | 98% | 80% | 0.829 |
| PLAP | 69 | 100% | 90% | 0.935 |
| PLAP/ALP ratio | 0.44 | 100% | 98% | 0.980 |
ROC of serum ALP, PLAP and PLAP/ALP ratio in hypertensive disorders of pregnancy. Placental alkaline phosphatase, ALP – Alakaline phosphatase, AUC- Area under the curve
Discussion
In the present study, the serum ALP and PLAP were significantly higher in pregnant mothers with hypertension, which was similar to those seen in other studies [18–21]. Our study also shows that there is a good positive correlation between PLAP and blood pressure. Alkaline phosphatase is a ubiquitous enzyme involved in the transport of sugar and phosphate across the trophoblast cell membranes [22]. In normal pregnancy, the serum level of Total ALP is raised, attributable to the placental isoenzyme. The increase is about twice the upper limit of the reference range for non-pregnant women. A peak raise in total ALP and PLAP is observed during 34 and 40 weeks of gestation. The highest levels are noticed at 38 weeks of pregnancy [11,21].
The mean values of ALP in normal pregnant women between 36-40 weeks was 206.13 ± 39 IU/L and the PLAP levels were 93.8 ± 17.4 IU/L, which reflects that the PLAP contributes 45% of the total ALP in pregnant women with normal BP and 55% in the hypertensive women. This correlates well with the previous studies [11,20,21].
In contrast, Yamaguchi et al., have observed that heat stable alkaline phosphatase was elevated in normal pregnancy and there was a fluctuating pattern (unstable) in toxaemia of pregnancy [23].
Zhonghua Fu and Chanke Za Zhi have shown that ALP and PLAP increased with the advance of gestational weeks. In pregnant women with severe hypertensive, ALP was elevated, but PLAP remained at consistently low levels [24].
A deviation from the normal values of PLAP during pregnancy helps in predicting impaired placental function. Decreased serum PLAP in pregnant women could be associated with intrauterine growth retardation (IUGR), premature rupture of membranes and premature labour [25]. It has been observed that in human fetal fibroblasts, PLAP stimulates DNA synthesis and cell proliferation in synergism with insulin, Zinc and Calcium, thus playing an important role in promoting fetal development [22].
The elevated levels of serum PLAP and ALP in hypertensive pregnant women may be attributed to placental dysfunction, which results in increased serum levels of these enzymes. Shedding of syncytiotrophoblast into the maternal circulation is a normal part of pregnancy, but is increased during pre-eclampsia. In pre-eclampsia, this process of syncytio-trophoblast renewal is overactive and complicated by necrosis and apo necrosis of the syncytio-trophoblast particles [26]. As it is a well known fact that when there is cell lysis the enzyme from the plasma membrane of syncytio-trophoblastic cells are released into circulation. The decreased ALP activity in the damaged area conceivably brings about a compensatory increase of ALP activity in the undamaged area, thereby contributing to the raised ALP and PLAP levels. ALP is a membrane associated enzyme and participates in membrane transport mechanism that might be imperative for placental metabolism, this in turn to the fetus.
Further the ALP, PLAP and their ratio are index of placental function and a sudden rise in their activity in the serum indicates an abnormality in placental functioning and forewarns about the impending fetal wellbeing.
There are reports that point to the fact that mean arterial pressure is a better indicator rather than DBP, and it is a better predictor of HDP [27]. However, due to ease of reporting DBP values, MAP has not been widely used. In the present study MAP had a better correlation with PLAP then that of DBP.
The other aspect in this study is raised serum uric acid levels in HDP and its positive correlation with blood pressure. Uric acid is a potent inhibitor of endothelial function, found to induce systemic and glomerular hypertension in animals [28]. Also, increased tubular reabsorption and decreased tubular secretion of uric acid in tubules or diminished renal blood flow, similar to the physiologic response to hypovolemia bay be the cause for hyperurecimia.
However, it may not be a pragmatic approach to estimate several biochemical parameters, especially in healthcare centres with associated small and medium sized biochemistry laboratories. Hence, a better and practical approach towards the assessment of hypertensive disorders of pregnancy would be to utilize heat stable ALP isoenzyme (PLAP) and PLAP/ALP ratio as an adjuvant marker in the armamentarium of biochemical tests, especially since the same is simple to assay and reliable as well as economical and sensitive. HDP continues to be a major cause of maternal and fetal mortality and morbidity in developing countries. The prevention of HDP lies in early detection, effective institutional treatment and prudent termination of pregnancy during preeclampsia. Hence it could be an adjuvant biomarker of HDP and could be helpful in assessing the severity and in predicting fetomaternal prognosis.
However, in this study we didn’t study regarding the future outcome of pregnancy, which could have provided more information regarding both maternal and fetal outcome. This could be the scope of future studies, to further document the utility of these markers in the management of HDP.
Conclusion
Heat stable ALP (PLAP) measurement can afford a simple, reliable and economical adjunctive laboratory parameter in hypertensive disorders of pregnancy.
Measurement of PLAP/ ALP ratio and serum uric acid could be utilised as pragmatic and reliable biochemical markers, especially in small and medium sized diagnostic laboratories. Moreover, it is economically viable for the semi-urban and rural population.
Mean and S.D of blood pressure and biochemical parameters in Cases and control. ; Data represented are mean ± SD. Independent T- test was used to analyse the data. ; Systolic BP- systolic blood pressure, Diastolic BP- Diastolic blood pressure, PLAP- Placental alkaline phosphatase, ALP- Alkaline phosphatase and PLAP/ALP ratio- Placental alkaline phosphatase/ Alkaline phosphatase
Pearson correlation analysis was performed; p < 0.05 considered significant. PLAP- Placental alkaline phosphatase, ALP – Alakaline phosphatase, DBP- Diastolic blood pressure, MAP- Mean arterial blood pressure
ROC of serum ALP, PLAP and PLAP/ALP ratio in hypertensive disorders of pregnancy. Placental alkaline phosphatase, ALP – Alakaline phosphatase, AUC- Area under the curve
[1]. Say L, Chou D, Gemmill A, Tunçalp Ö, Moller A-B, Daniels J, Global causes of maternal death: a WHO systematic analysisThe Lancet Global Health 2014 2(6):e323-33. [Google Scholar]
[2]. Prakash J, Pandey LK, Singh AK, Kar B, Hypertension in pregnancy: hospital based studyJ Assoc Physicians India 2006 54:273-8. [Google Scholar]
[3]. Shruthi SD, Wani RJ, Priti C, Hegde CV, PIH- confounding situations, management dilemmas and severe consequences: does antenatal care have a role?Bombay hospital journal 2008 50(1):34-37. [Google Scholar]
[4]. American College of Obstetricians and Gynecologists, Task Force on Hypertension in PregnancyHypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in PregnancyObstet Gynecol 2013 122(5):1122-31. [Google Scholar]
[5]. Report of the National High Blood Pressure Education Program Working Group on High Blood Pressure in PregnancyAm J Obstet Gynecol 2000 1831:S1-22. [Google Scholar]
[6]. Many A, Hubel CA, Roberts JM, Hyperuricemia and xanthine oxidase in preeclampsia, revisitedAm J Obstet Gynecol 1996 174:288-91. [Google Scholar]
[7]. Williams PJ, Broughton Pipkin F, The genetics of pre-eclampsia and other hypertensive disorders of pregnancyBest Practice & Research Clinical Obstetrics & Gynaecology 2011 25(4):405-17. [Google Scholar]
[8]. Pantegghini M, Bais R, van Solinge WW, Enzymes. In Burtis CA, Ashwood ER, Bruns DE, editorsTietz text book of clinical chemistry and Molecular Diagnostics 2006 4Philadelphia, PAElsevier Saunders:597-643. [Google Scholar]
[9]. Donald WM, Alkaline Phosphatase lsoenzymesClin Chem 1982 28(10):2007-16. [Google Scholar]
[10]. Griffiths G, Black J, Separation and identification of alkaline phosphatase isoenzymes and isoforms in serum of healthy persons by isoelectric focusingClin chem 1987 33(12):2171-77. [Google Scholar]
[11]. Mangal A, Gaur U, Jain A, Goyal U, Tripathi R, Rath R, Alkaline phosphatase and placental alkaline phosphatase activity in serum of normal and pregnancy induced hypertensive mothersJIMSA 2007 20(2):117-20. [Google Scholar]
[12]. Mangal A, Shrivastava P, Gaur U, Jain A, Goyal U, Rath G, Histochemical Analysis of Placental Alkaline Phosphatase in Hypertensive Disorders complicating PregnancyJournal of the Anatomical Society of India 2005 54(2):2005-12. [Google Scholar]
[13]. Boronkai A, Than NG, Magenheim R, Bellyei S, Szigeti A, Deres P, Extremely high maternal alkaline phosphatase serum concentration with syncytiotrophoblastic originJ Clin Pathol 2005 58(1):72-76. [Google Scholar]
[14]. Galski H, Fridovich SE, Weinstein D, De Groot N, Segal S, Folman R, Synthesis and secretion of alkaline phosphatase in vitro from first-trimester and term human placentasBiochem J 1981 194(3):857-66. [Google Scholar]
[15]. IFCC method for the measurement of ALPJ Clin Chem Clin Biochem 1983 21:731-48. [Google Scholar]
[16]. Trivedi R, Berta E, Rebar L, Enzymatic uric acid determination at 500nm by Trinder methodClin chem 1976 22:1223 [Google Scholar]
[17]. Fishman WH, Ghosh NK, Isoenzymes of human alkaline phosphataseAdv clin chem 1967 10:255-370. [Google Scholar]
[18]. Dabare AA, Nouri AM, Cannell H, Moss T, Nigam AK, Oliver RT, Profile of placental alkaline phosphatase expression in human malignancies: effect of tumour cell activation on alkaline phosphatase expressionUrol Int 1999 63(3):168-74. [Google Scholar]
[19]. Marshall BR, Parisi F, Maternal serum heat-stable alkaline phosphatase in normal and high-risk pregnanciesObstet Gynecol 1975 45(2):136-41. [Google Scholar]
[20]. Aleem FA, Total and heat stable serum alkaline phosphatase in normal and abnormal pregnanciesObstet Gynae 1972 40(2):163-72. [Google Scholar]
[21]. Okesina AB, Donaldson D, Lascellesc PT, Morris P, Effect of gestational age on levels of serum alkaline phosphatase isoenzymes in healthy pregnant womenInternational Journal of Gynecology & Obstetrics 1999 48(1):25-29. [Google Scholar]
[22]. She QB, Mukerjee JJ, Huang JS, Grilly KS, Kiss Z, Growth factor like effects of placental alkaline phosphatase in human fetus and mouse embryo fibroblastsFEBS letters 2000 469:163-67. [Google Scholar]
[23]. Yamaguchi R, Noda K, Fujiyama T, Relationship between Histochemical Alkaline Phosphatase Activity in the Placenta and Patterns of Serum Heat-stable Alkaline Phosphatase in Late PregnancyThe Tohoku Journal of Experimental Medicine 1971 105(2):129-35. [Google Scholar]
[24]. Zhonghua Fu, Chanke Za Zhi, Clinical significance of serum Alkaline phosphatase, heat stable alkaline phosphatase, liver alkaline phosphatase and Gamma GT determination in high risk pregnancy 1989 24(2):66-69. [Google Scholar]
[25]. Rodin A, Duncan A, Quartero HWP, Pistofidis G, Mashiter G, Whitaker K, Serum Concentrations of Alkaline Phosphatase Isoenzymes and Osteocalcin in Normal PregnancyThe Journal of Clinical Endocrinology & Metabolism 1989 68(6):1123-27. [Google Scholar]
[26]. Hutchinson ES, Brownbill P, Jones NW, Abrahams VM, Baker PN, Sibley CP, Utero-Placental Haemodynamics in the Pathogenesis of Pre-EclampsiaPlacenta 2009 30(7):634-41. [Google Scholar]
[27]. Cnossen JS, Vollebregt KC, de Vrieze N, ter Riet G, Mol BW, Franx A, Accuracy of mean arterial pressure and blood pressure measurements in predicting pre-eclampsia: systematic review and meta-analysisBMJ 2008 336(7653):1117-20. [Google Scholar]
[28]. Kang DH, Finch J, Nakagawa T, Karumanchi SA, Kanellis J, Granger J, Uric acid, endothelial dysfunction and pre-eclampsia: searching for a pathogenetic linkJ Hypertens 2004 22(2):229-35. [Google Scholar]