Saliva contains both host- derived and microbial derived factors, including several enzymes that degrade proteins, proteoglycans lipids and carbohydrates. The interplay between periodontal pathogens and the inflammatory–immune system leads to development of chronic inflammation [1,2]. In diseased states, cytokines may be secreted not only by resident cells but also by locally infiltrated immune-competent cells [3]. The balance between T helper cells 1 (TH1) and T helper cells 2 (TH2) phenotypes determines the successful resolution of inflammation. The TH1 response partially results from the availability of IL-12, which drives uncommitted T helper cells (TH0) cells into the TH1 phenotype; the influence of IL-12 continues the establishment of the cell-mediated response [4]. The TH1 response is maintained by interferon-gamma (IFN-γ), which inhibits the TH2 response [5]. IL-12 is a cytokine with both pro inflammatory and immuno-regulatory activity, and has a major role in the initiation and enhancement of gingival inflammation [4]. Saliva is a primary growth environment for flora of the oral cavity. As the physico-chemical properties are changed, it effects the microorganisms which grow in the mouth [6]. Salivary secretions are protective in nature because they maintain the oral tissues in a physiologic state. The protective effect of saliva may be accomplished by means of secretion rate, buffering capacity, calcium and phosphate concentration and antibacterial system [7]. The fluid with or without stimulation is readily accessible via a totally non-invasive collection method, and contains locally produced microbial and host response mediators. Since the 1990s, saliva has been used in disease diagnosis in internal medicine [8]. Subsequently, saliva has been used in the diagnosis of periodontal disease and monitor response to treatment [9]. It is desirable to determine whether non-surgical periodontal therapy can alter the levels of these markers, so that a novel link between periodontal disease and other systemic inflammatory diseases can be explored. Therefore, the aim of this study was to compare IL-12 levels between healthy subjects and patients with periodontal disease, and observe whether the levels IL-12 changed after one month of non-surgical periodontal therapy.
Materials and Methods
Subjects
The present interventional study was approved by the Institutional Review Board of Swami Vivekanand Subharti University. Subjects were recruited from age group between 30 and 45yrs with moderate to severe Generalized Chronic Periodontitis (GCP) from out-patient at Subharti Dental College and Hospital and a written informed consent obtained from them. Each subject had at least 20 standing teeth, with at least five teeth with sites probing 5mm or deeper and radiographic evidence of alveolar bone loss. Subjects had received no previous periodontal treatment, antimicrobial therapy or periodontal surgery in the preceding six months had no periapical lesions, or restorations. Subjects with systemic diseases, pregnancy, lactating mothers, or smokers were excluded. Generalized Chronic Periodontitis was diagnosed according to the criteria of the American Academy of Periodontology [10].
Sample collection
Patients were appointed during early hours between 8-10 AM. Paraffin -Stimulated saliva was collected for five minutes (~5-10 ml) from each subjects sitting in an upright posture, into sterile tubes according to the method described by Navazesh [11]. The subjects refrained from eating, drinking, and oral hygiene for two hours prior to saliva collection. Saliva was immediately centrifuged at 3500 rpm at – 4°C for 10 min and stored at - 800C till analysis. Samples were thawed and analysed within six months of collection using a commercially available sandwich immunoassay kit procured from (WELDON Biotech India Pvt. Ltd).
Clinical Parameters
Clinical and radiographic examination was performed by a single, experienced examiner after collection of saliva. Plaque index (P.I)[12], Gingival index (G.I) [13], Bleeding on probing (BOP), Probing pocket depth (PPD) and Clinical attachment level (CAL) using UNC 15 probe were measured at six sites per tooth.
Treatment
Following collection of saliva, subjects received single sitting of full mouth scaling and root planing. No antibiotic, anti-inflammatory or any form of chemical plaque control aid was prescribed following treatment. The patients were re-evaluated one month after completion of phase I therapy and saliva was re-sampled. The periodontitis group before phase I therapy was called the BT group, and the same group after completion of 1 month of therapy was called the AT group.
Statistical Analysis
The data were analysed using a statistical SPSS Package (version-10), Mann-Whitney U-post hoc pair wise comparisons was performed to determine the difference of IL-12 levels between the groups. The Wilcoxon signed-rank test was used for comparisons between clinical parameters pre and post therapy. The correlations between IL-12 levels and clinical parameters were assessed using Spearman rank correlation analysis. p-values <0.05 were considered statistically significant.
Results
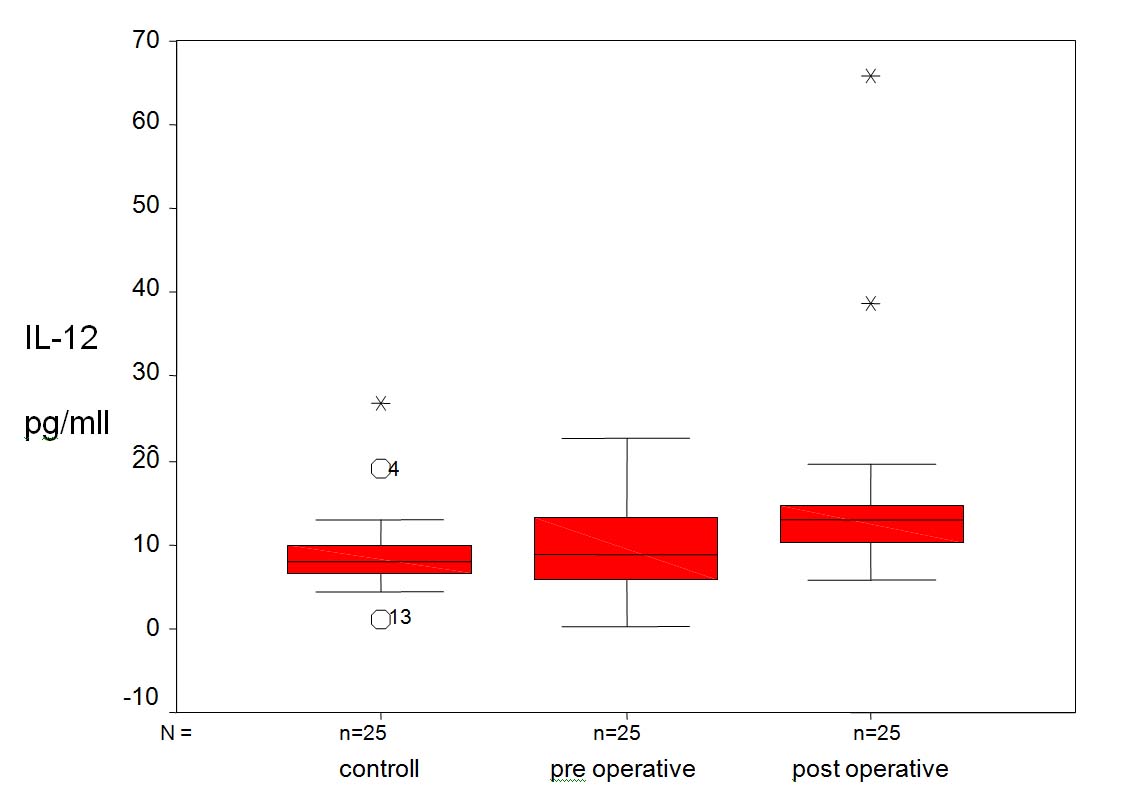
Detectable levels of IL-12 were found in all saliva samples of cases and controls. The range (Mean ± SD (min-max) of IL-12 levels in controls and patients with periodontitis (BT and AT) were 9.18±4.94 (1.15-26.54), 9.79±5.70 (.38-22.31), 15.93±12.09 (5.76-65.76) respectively. Mean IL-12 levels in patients with periodontitis at baseline were lower (p=.54) than in controls (Wilcoxon signed-rank test). IL-12 levels in patients with periodontitis increased significantly (p= 0.001) post-treatment, and significantly higher (p<.001) than baseline values of controls (Man Whitney U Test) Increase in IL-12 levels was observed in all patients with periodontitis, in whom elevated levels were noted post-therapy [Table/Fig-1]. The median (interquartile range) values of IL-12 levels in the control, BT, and AT groups were 3.74 pg/ml, 7.96 pg/ml and 4.92 pg/ml respectively [Table/Fig-2]. IL-12 showed no significant positive correlation with any of the clinical parameters (Spearman rank correlation analysis) [Table/Fig-3]. Treatment improved plaque scores, bleeding scores, and gingival score; there was a gain in CAL and reduction in probing depths.
Test of significance for clinical and immunological characteristic of control and patients with periodontitis
| Characteristics | Control(n=25) Mean±SD (min-max) | Periodontitis (n=25) |
|---|
| Before therapy | After therapy |
|---|
| AGE(yrs) | 34 (30-45) | 38(30-45) | 38(30-45) |
| GI | 0.04±0.12(0-0.42) | 1.84±.22 | 1.23±.47 |
| PI | 0.10±.14(0-0.54) | 1.78±.22 | 1.12±.22 |
| BOP | 3.80±2.53(0-7.80) | 89.26±10.57 | 35.47±19.84 |
| PPD | 1.86±0.27 | 3.32 ±0.50 | 2.67±.50 |
| CAL | 0 | 3.99±0.62 | 3.34±1.48 |
| IL-12 | 9.18±4.94(1.15-26.54)# | 9.79±5.70(0.38-22.31)*# | 15.93±12.09(5.76-65.76)*# |
*comparing the periodontitis patients (Wilcoxon Signed Rank Test p=.001, #comparing the control with periodontitis patients (Mann Whitney U Test), Control vs preoperative p=0.54 and control vs postoperative p<0.001
Box Whisker Plot for IL-12., The above figure shows the level of IL-12 between control and periodontitis patients. The upper margin of the boxes represent the third quartile and the lower margin indicate the first quartile. The horizontal line within each boxes is the median. The end of the whiskers represents the maximal and minimal values.
Correlation Coefficient of IL-12 with Clinical Parameter
| Group | Clinical Parameter | Interleukin-12 |
|---|
| r | P- Value |
|---|
| Control n=25 | GI | 0.24 | 0.24 |
| PI | 0.37 | 0.07 |
| BOP | 0.07 | 0.78 |
| PPD | 0.12 | 0.56 |
| CAL | -- | -- |
| Preoperative n=25 | GI | -0.11 | 0.59 |
| PI | 0.34 | 0.09 |
| BOP | 0.15 | 0.45 |
| PPD | 0.23 | 0.25 |
| CAL | -- | -- |
| Postoperative n=25 | GI | 0.06 | 0.75 |
| PI | 0.03 | 0.87 |
| BOP | 0.05 | 0.81 |
| PPD | 0.03 | 0.85 |
| CAL | -0.11 | 0.59 |
r = Spearman rank correlation coefficient
Discussion
The intensity, duration and resolution of inflammation depend on shifting the balance between the activities of proinflammatory and anti-inflammatory cytokines during the periodontal inflammation [14,15].
Periodontal disease results from release of inflammatory mediators, and the consequence is a significant breakdown of tooth-supporting tissues, finally leading to tooth loss [16]. IL-12 has multiple biological activities. Early application or production of IL-12 during infection may activate macrophages and augment a host’s cell-mediated immunity while shaping the ultimate antigen-specific immune responses. Successful periodontal therapy results clinically in shallow probing depths and a low tendency towards BOP and microbiologically, in a low detection level of periodontal pathogens [17]. In addition it reduces the size of inflamed lesion and causes a decrease in the periodontal tissues of inflammatory cell subsets, like B cells, T cells and plasma cells [18].
In humans, the major effect of IL-12 is to stimulate IFN-γ production by Th1cells and regulate the transition from an early innate immune response to an adaptive immune response [19]. The results of the present study showed minute amount of IL-12 in saliva, with the levels increasing in GCP subjects post therapy. The present study also demonstrated that the concentration levels of IL-12 had no significant correlation with any of the above clinical parameters, indicative of periodontal inflammation, in the entire group. Tsai et al., [20] showed that the total amount of IL-12 in GCF was significantly higher in Chronic Periodontitis (CP) than in Gingivitis and healthy subjects, while they reported significantly higher concentrations of IL-12 in healthy compared with CP subjects. These authors suggested that IL-12 could be related to the pathogenesis of inflammatory periodontal disease. Another study [21] demonstrated that very little concentrations of IL-12 in GCF were detected, with the levels decreasing with increasing inflammation. It is well established that with increasing inflammation, there are increasing amounts of GCF [22,23]. This could partly be the reason for the higher concentrations of IL-12 in healthy sites in the previous studies. Although the expression pattern is variable, these findings, together with our results, indicate that there is an association between IL-12 and periodontal disease.
Yucel et al., [24] in their study found that the total amount of IL-12 was significantly higher in CP subjects than that in Control group (p<0.05). IL-12 concentrations did not differ among the groups. They found no correlation of IL-12 with any of the clinical parameters. Our study revealed significant differences in IL-12 concentrations in severe Chronic Periodontitis and Control group (p=0.54). There was a significant difference between control and post treatment (AT) (p<.001) but found no significant correlation of IL-12 with any of the clinical parameters. The expression pattern is variable, these findings, together with our results, indicate that there is an association between IL-12 and periodontal disease, although, the time interval (one month) between the two clinical examinations, before and after treatment, may be too short to observe any clinical change in some patients. The present study also demonstrated that both the total amounts and the concentration levels of IL-12 had no significant correlation with any of the above clinical parameters, indicative of periodontal inflammation, in the entire group.
In a study by Fokkema et al., [25], it was suggested that antigen presenting cells (APCS) from Periodontitis patients have a Th2- promoting phenotype, i.e. releasing low levels of PGE2.This suggested that APCS from Periodontal patients might have an intrinsic characteristic in driving specific Th2 cell responses, and thereby promoting the humoral immunity in periodontitis.
Paschalina Goutoudi et al., [26] in their study found that periodontal treatment led to improvements in all clinical parameters. At six weeks, mean PD, CAL, PI, and GI scores were significantly decreased (p<0.01). In non diseased sites, periodontal therapy resulted in a significant decrease only in PI and GI scores at six weeks (p<0.01). Thus, the progression of periodontal inflammation may be due to a lacking or inappropriate response of anti-inflammatory cytokines.
Conclusion
The local action of cytokines, which is heavily dependent on recruitment, interaction and activation of immune competent cells can explain the site specific nature of cytokine expression. The findings of elevated salivary IL-12 levels post-therapy in patients with severe chronic periodontitis compared to healthy controls suggest a close association between salivary IL-12 and periodontal status. Thus, IL-12 might be potentially useful in distinguishing health from disease and monitoring periodontal disease activity. Future longitudinal studies with larger sample sizes are needed to validate salivary IL-12 as a marker for periodontal disease.
*comparing the periodontitis patients (Wilcoxon Signed Rank Test p=.001, #comparing the control with periodontitis patients (Mann Whitney U Test), Control vs preoperative p=0.54 and control vs postoperative p<0.001
r = Spearman rank correlation coefficient