Carcinosarcoma Masquerading as Giant Cystic Hematomasurekha
Surekha B Hippargi1, Anita P Javalgi2, Anirudh V Kushtagi3, Padmaja R Kulkarni3, Mamta K3
1 Professor, Department of Pathology, Shri B M Patil Medical College, Sholapur Road, Bijapur, India.
2 Assistant Professor, Department of Pathology, Shri B M Patil Medical College, Sholapur Road, Bijapur, India.
3 Assistant Professor, Department of Pathology, Shri B M Patil Medical College, Sholapur Road, Bijapur, India.
4 Associate Professor, Department of Pathology, Shri B M Patil Medical College, Sholapur Road, Bijapur, India.
5 Post Graduate, Department of Pathology, Shri B M Patil Medical College, Sholapur Road, Bijapur, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Anita P Javalgi, Professor, Department of Pathology, Bldeu’s Shri B M Patil Medical College, Sholapur Road Bijapur-586103, India. Phone : 09739619068,
E-mail: javalgianita@gmail.com
Carcinoarcoma of breast is rare tumor with aggressive behaviour and poor prognosis. Histologically it is biphasic tumor with epithelial and mesenchymal component. Very few cases of carcinosarcoma, its presentation and behaviour have been reported in the literature, and due to its bizarre behaviour it is a diagnostic challenge to pathologist and clinicians. Here we present a rare case of carcinosarcoma breast in a 55-year-old female who initially presented with cystic mass( lump) in right breast which was reported as organised hematoma on FNAC, on frozen section it was diagnosed as malignant cystic tumour. This was followed by mastectomy. Histopathology with immune markers, the case was diagnosed as metaplastic carcinoma with biphasic type called carcinosarcoma. The case merits presentation because of its rare presentation as cystic lesion and difficult to diagnose mainly due to sarcomatous elements. An accurate diagnosis of this aggressive tumour is essential in order to optimally tailor adjuvant therapy.
Breast cancer, Carcinosarcoma, Cystic mass, Organised hematoma
Case Report
A 55-year-old female presented with lump in the right breast since 4 months, on clinical examination-a well-defined solid to cystic mass noted in the upper outer quadrant of right breast measuring 7x5 cm. axillary lymphnode were clinically not palpable. Nipple, aerola, skin over the swelling and left breast was normal Repeated aspirations from the lump yielded 5ml of hemorrhagic fluid, smears studied from the aspiration showed hemosiderin laden macrophages and few spindle shaped cells and reported as organized hematoma and advised USG guided Fine needle aspiration cytology to rule out malignancy. Lumpectomy was performed with frozen section study which was reported as malignant cystic tumour.
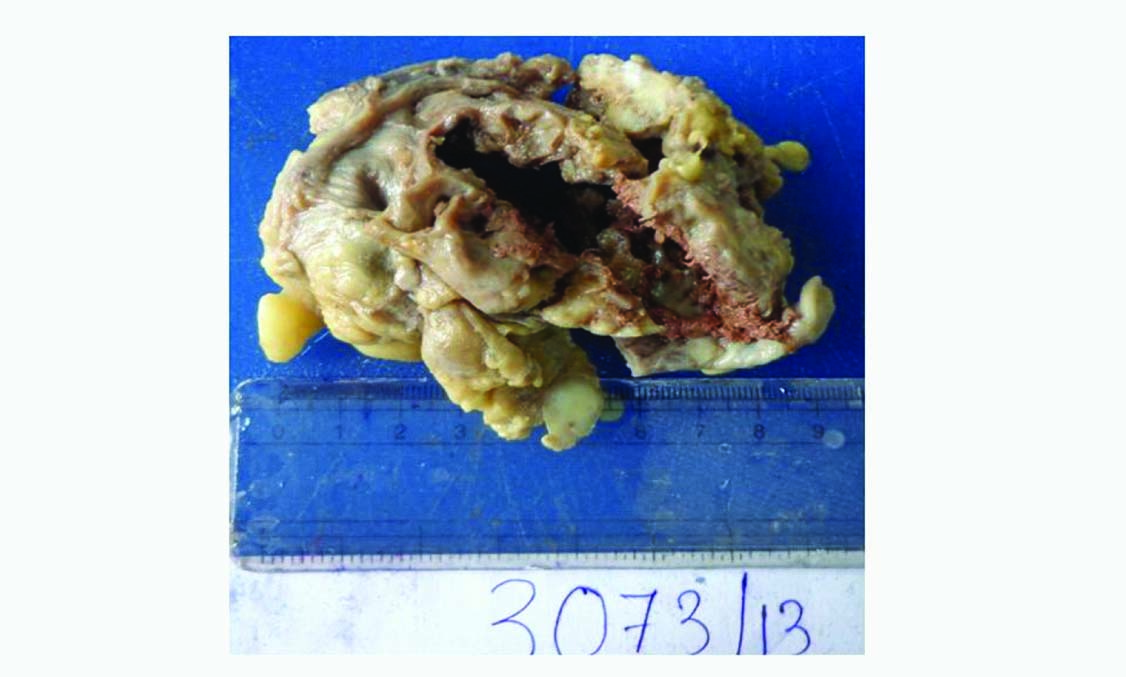
Lumpectomy [Table/Fig-1] mass revealed cystic mass measuring 8x8x3cms, 20ml of haemorrhagic brown fluid was drained. Cut section of cystic mass showed an irregular grey white growth measuring 3x2cm. Microscopically sections studied showed tumour tissue arranged in diffuse sheets and interlacing fascicles, tumour cells showed hyperchromatic nuclei and moderate eosinophilic cytoplasm.Reported as positive for malignancy, surgical procedure was followed with modified radical mastectomy and specimen was sent for histopathological examination.
Lumpectomy specimen showing alarge cyst measuring 8x8x3cm
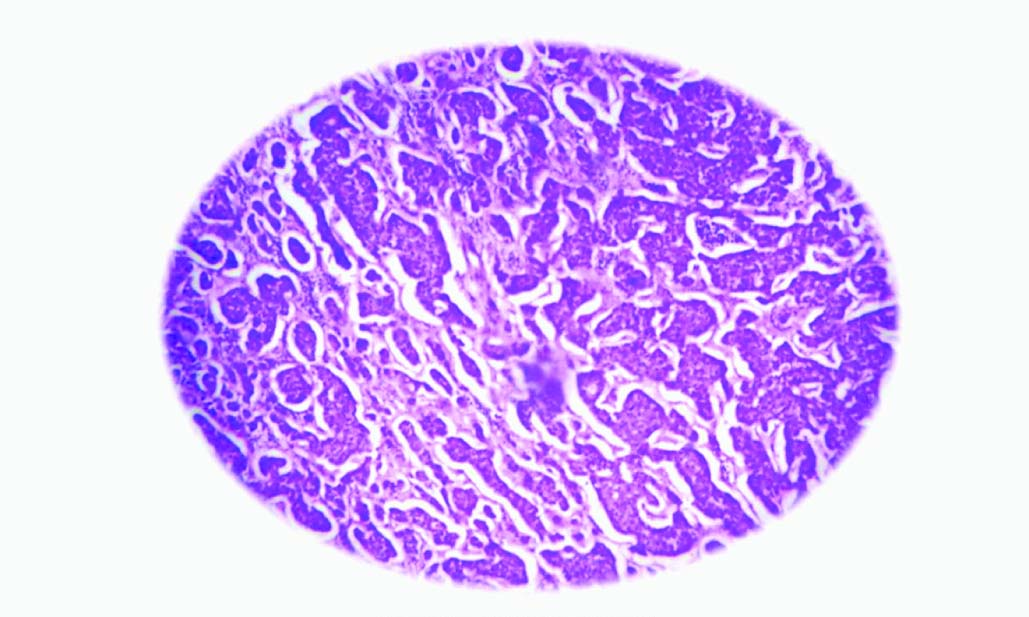
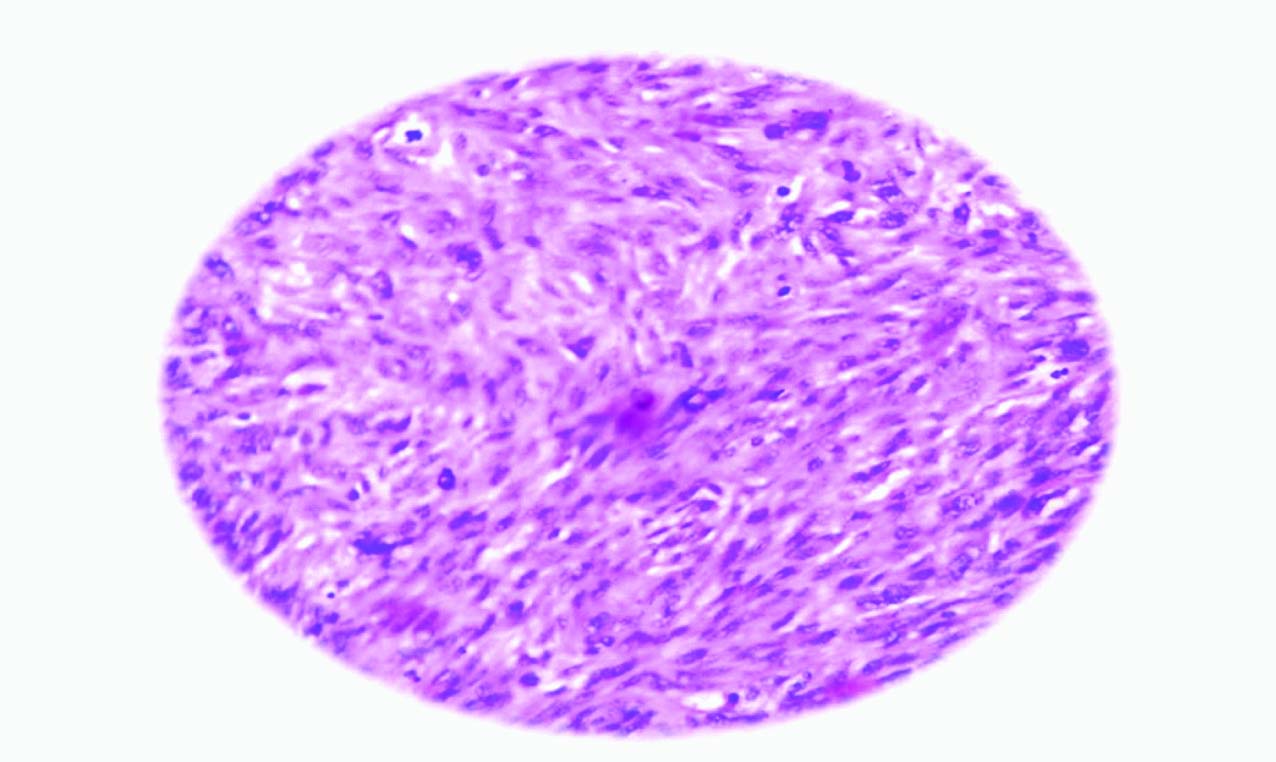
Microscopically, there was bifocal tumour tissue, tumour cells arranged in syncytial sheets, cords separated by variable amount of fibrous septa. Individual tumour cells are large round to oval with round to oval pleomorphic, hyperchromatic nuclei and moderate amount of eosinophilic cytoplasm suggestive of invasive ductal carcinoma [Table/Fig-2]. Also noted, tumour tissue arranged in sheets comprised of spindle cells having elongated vesicular nuclei with coarse chromatin having prominent nucleoli and moderate eosinophilic cytoplasm resembling malignant fibrous histiocytoma and fibrosarcoma (sarcoma like component) [Table/Fig-3]. This was evident of gradual transition of tumour cells from carcinoma to sarcoma. The tumour tissue is infiltrating into the surrounding stroma, with dense areas of necrosis, chronic inflammatory cell infiltrate. Surrounding breast tissue showed features of ductal carcinoma in situ & fibrocystic change. All surgical margins were free from tumour tissue. Lymph nodes showed tumour tissue deposits. Pectoralis muscle was free from tumour tissue.
H & E Stain 200X Microscopy showing intraductal component
H & E Staining 200X Microscopy showing sarcomatous component
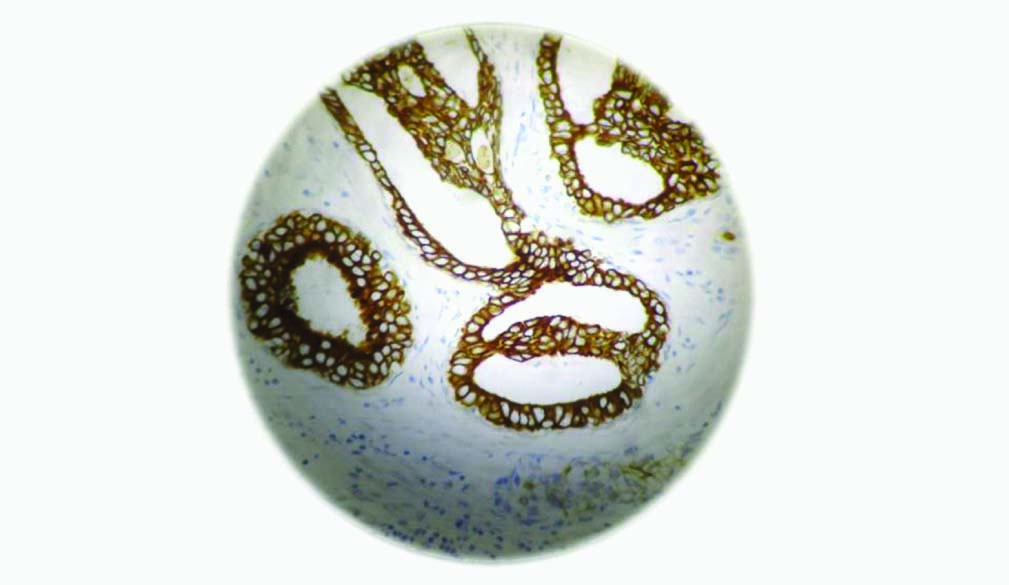
Immunohistochemistry is postive for pancytokeratin/ck7 and vimentin & negative for CK 5&6 / CK 20/ P63/ HMW CK/ GCDFP 15/ mammoglobin [Table/Fig-4,5]. The case was diagnosed as carcino-sarcoma of right breast (metaplastic carcinoma - biphasic type).
Immunohistochemistry shoing positive cytokeratin (CK) 7
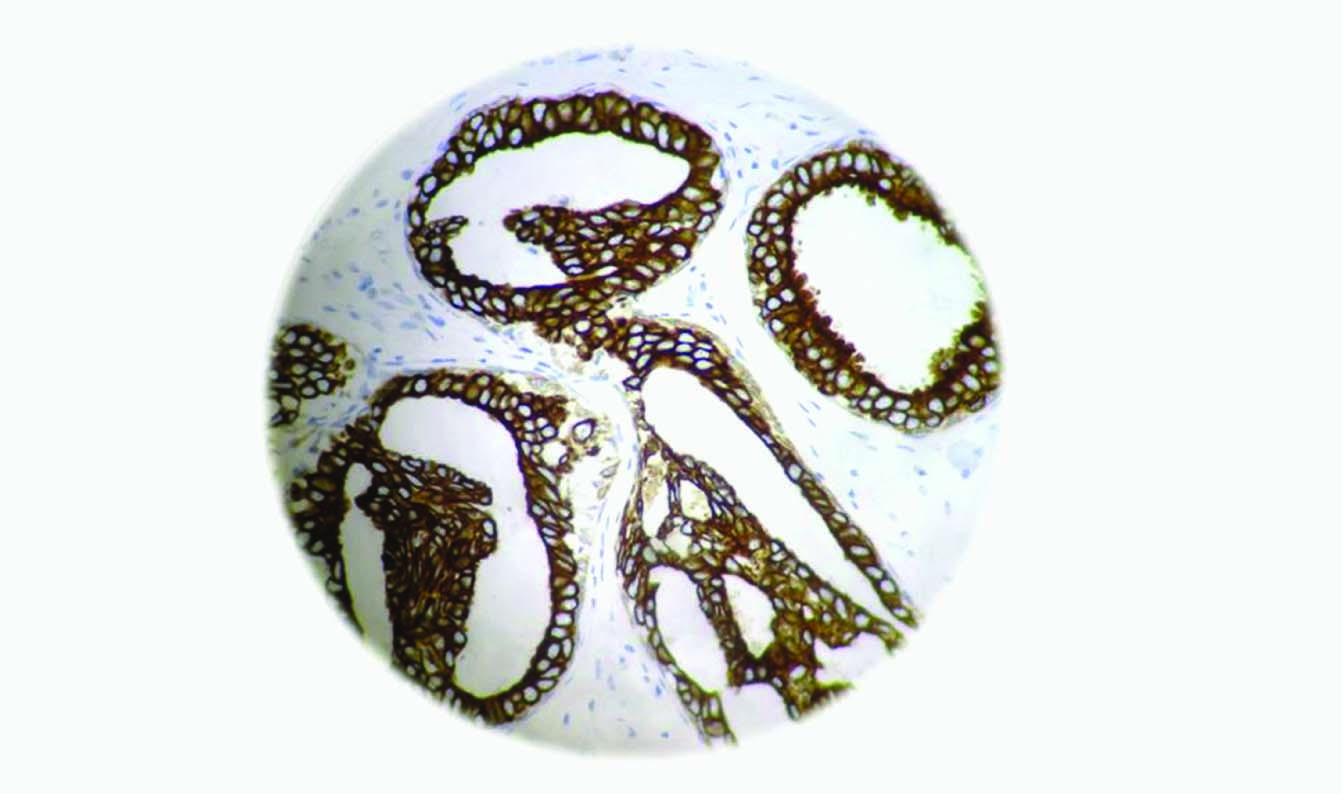
Immunohistochemistry showing positive for pancytokeratin (PAN CK)
Discussion
Clinical findings often reveal swelling in the breast or a palpable mass. Rarely, nipple discharge, nipple retraction or skin ulceration may also be present [1]. Rarely, they present with large cystic mass though necrosis and cystic degeneration may be evident in few areas of malignancy. Clinically carcinosarcoma of the breast is an aggressive breast cancer [1,2].
Breast cancer is a heterogeneous disease with regard to histopathological types. The most common histopathology is infiltrating ductal carcinoma, which accounts for about 80% of all breast cancers. Carcinosarcoma of the breast is an aggressive and rare neoplasm [3]. Its reported incidence is 0.1% of all breast malignancies [1,2]. It has biphasic differentiation of cells possessing epithelial and mesenchymal characteristics and suggests myoepithelial origin or differentiation. These tumours do not express the estrogen or progesterone receptors and HER-2/neu oncogene. Due to this “triple negative” phenotype, such tumours tend to be more aggressive. Immunohistochemical features of carcinosarcoma breast shows immunoreactivity for keratin (55%), vimentin (98%), actin (77%) and S-100 protein (55%) [2,4].
Carcinosarcoma breast usually presents as large lump in breast, often painful and show no preference for any particular age group. Clinical features of metaplastic breast cancer are similar to those patients with invasive ductal carcinoma [5].
Sonographically, it shows complex echogenicity with solid and cystic components which may be related to necrosis and cystic degeneration. The cell of origin of these tumours is still being debated, but most of the research leads us to the conclusion that these tumours are of myoepithelial origin with both carcinomatous and sarcomatous features on histopathology [6].
Carcinosarcoma of the breast metastasize via lymphatics and bloodstream. The incidence of lymph nodal metastasis from metaplastic carcinoma is lower than might be anticipated for infiltrating duct carcinoma, in keeping with the sarcomatous phenotype [4].
The clinical and pathologic features of metaplastic breast carcinomas are important to distinguish from other types of uncommon breast malignancies such as spindle cell carcinoma, matrix producing carcinoma, fibrosarcoma, osteosarcoma, malignant fibrous histiocytoma, phylloides tumour and stromal sarcoma as their behavior, response to treatment and survival rates differ greatly [6,7].
In general, the recommended treatment options have followed the established guidelines for treatment of patients with invasive breast cancer. In the majority of the reported cases, mastectomy with or without axillary lymph node dissection was performed, followed by post-operative chemotherapy and radiation therapy. One study by Kim et al., reported that patients who were treated with neoadjuvant or adjuvant anthracycline based chemotherapy showed a better clinical outcome compared to those treated with CMF (cyclophosphamide, methotrexate, 5-fluorouracil) and the neoadjuvant chemotherapy for carcinosarcoma breast was less effective than for conventional adenocarcinoma [8].
Conclusion
Carcinosarcoma of the breast is a very aggressive lesion and is a diagnostic and therapeutic challenge to pathologist as well the surgeons. In the present case the patient had an enormous cystic lesion that could be mistaken with mastitis. Histopathology with immunohistochemistry confirms the diagnosis & remains a gold standard. This entity needs to be treated aggressively due to its poor prognosis.
[1]. Kristi ME, Ramona MH, Susan AB, John JL, Adam IR, Carcinosarcoma of the breast: two case reports and review of the LiteratureCases Journal 2009 2:15-20. [Google Scholar]
[2]. Muhammad AA, Humera M, Muhammad F, Khurshid AK, Javed I, Carcinasarcoma of the BreastJournal of the College of Physicians and Surgeons Pakistan 2012 22(5):333-34. [Google Scholar]
[3]. Roberta L, Ana C, Luis O, Rosemar R, Ruffo F-Jr, Régis P, Carcinosarcoma of the Breast Presenting as a Giant Cystic LesionJournal of sonologic international society 2010 1(3):504-07. [Google Scholar]
[4]. Hennessy BT, Giordano S, Broglio K, Duan Z, Trent J, Buchholz TA, Biphasic metaplastic sarcomatoid carcinoma of the breastAnn Oncol 2006 17:605-13. [Google Scholar]
[5]. Patrikar A, Maimoon S, Mahore S, Akhtar MA, Wilkinson A, Metaplastic carcinoma of the breast (carcinosarcoma variant)Indian J Pathol Microbiol 2007 50:396-98. [Google Scholar]
[6]. Gutman H, Pollock RE, Janjan NA, Johnson DA, Biologic distinctions and therapeutic implications of sarcomatoid metaplasia of epithelial carcinoma of the breastJ Am Coll Surg 1995 180(2):193-99. [Google Scholar]
[7]. Foschini MP, Dina RE, Eusebi V, Sarcomatoid neoplasms of the breast: Proposed definitions for biphasic and monophasic sarcomatoid mammary carcinomasSemin Diagn Pathol 1993 10(2):128-36. [Google Scholar]
[8]. Rosai J, Special techniques in surgical pathologyRosai and Ackerman’s Surgical Pathology. Mosby Ninth Edition 2004 :1810-12. [Google Scholar]