A Comparative Study on the Efficacy of Glucose and Sucrose on the Vaccination Pain: A Randomized Controlled Clinical Trial
Zainab Suhrabi1, Hamid Taghinejad2, Kobra Valian3, Kourosh Sayehmiri4, Safoura Taheri5
1 Lecturer, Department of Midwifery, Ilam University of Medical Sciences, Ilam, IR Iran.
2 Assistant Professor, Department of Nursing, Ilam University of Medical Sciences, Ilam, IR Iran.
3 Lecturer, Shahid Mostafa Khomieni (PBUH) Hospital, Ilam University of Medical Sciences, Ilam, IR Iran.
4 Associate Professor, Prevention of psychosocial injuries research center, Ilam University of Medical Sciences, Ilam, IR Iran.
5 Lecturer, Department of Midwifery, Ilam University of Medical Sciences, Ilam, IR Iran.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Hamid Taghinejad, Assistant Professor, Department of Nursing, Ilam University of Medical Sciences, Ilam- Iran. Phone : 00 98 841 2227123 P.O.Box : 69315138, Fax : 00988412227123, E-mail : hamid2005mordad@yahoo.com
Objectives: This study was performed to compare the effectiveness of two analgesics for the management of vaccination pain.
Materials and Methods: A total of 90 neonates to be vaccinated against Hepatitis B were assigned to Glucose, Sucrose and control groups at Shahid Mostafa Khomini hospital. 2cc oral Glucose 25% and 2cc oral Sucrose 25% with Syringe were given for 30 sec then 2 min later Hepatitis-B vaccine injected by vaccinator and pain intensity measured by Neonatal Infant Pain Scale (NIPS) during 1-2 min. The third group (control) no intervention was performed. The collected data were analysed by SPSS18 Software and ANOVA and LSD tests were used.
Results: Research results showed that there were no significant differences between groups in term of Apgar score, delivery type, sex, head circumstance, weight and height. By comparison of pain severity in two groups, mean and Standard deviation of pain, group that received Glucose solution had more intensity than Sucrose group (3 ± 1.66 vs. 2.90 ± 1.44), but this difference was not significant statistically (p=0.78). Comparison of pain intensity in control and intervention groups showed that the pain intensity in control group is higher than intervention groups (p<0.001).
Conclusion: Patients who received Glucose or Sucrose had lower pain intensity in comparison with the other. The pain intensity in patients who received sucrose was less than the glucose group, but this difference was not significant statistically.
Glucose, Pain, Sucrose, Vaccination
Introduction
Pain is a worldwide problem that often originates from disease process, diagnostic, treatment and may be preventive interventions such as vaccination [1,2]. Extensive literature review shows that preterm and full term infants are capable of responding to pain and noxious stimuli by midgestation. Considering these evidences health care providers need to identify safe and efficacious interventions to effects of procedural pain [3]. Relieving of pain in the newborn is essential; firstly, for ethical reasons and, secondly, because pain can lead to decreased oxygenation, hemodynamic instability, or increased intracranial pressure [2]. Recent research has shown that even short term pain can have lasting negative effects [4], while in health care settings Analgesia is not provided routinely to infants who undergo painful procedures [5] such as vaccination.
The pain associated with vaccination is a source of anxiety and distress for the children receiving the vaccination, their parents, and the providers who must administer them [6].
Nowadays various methods are used to reduce procedural pain in the newborn —such as oral sugar solutions (One of the most frequently studied), milk, or sucking a pacifier. Sucrose, Glucose and non-sucrose sweet tasting solutions have also been found to have analgesic effects on pain reactions during blood sampling, by heel stick or venipuncture in term and preterm newborn infants [4,7,8].
The pain-relieving effect of oral sugar solutions such as glucose and sucrose is believed to be mediated by two mechanisms: orotactile stimulation by the intraoral fluid gives an initial effect and orogustatory stimulation prolongs the effect through release of endogenous opioids. In some studies, oral sucrose or glucose has been used to alleviate pain reactions during blood sampling, by heel stick or venipuncture [8].
Sucrose is a disaccharide consisting of fructose and glucose, the administration of it has been most frequently examined non-pharmacological intervention for the relieving of pain in newborns [3]. The calming and pain-relieving effects of sucrose are thought to be mediated by endogenous opioid pathways activated by sweet taste [9]. Sucrose also has an immediate short-term attention-gaining response due to its strong taste which results in instant calming and cessation of crying [5]. Compared with sucrose, the sweetener glucose is 0.75 time as sweet [3]. Several psychometric tools are available to assess pain in the neonate. Although, clinically tested, most of these tools have not been integrated into the assessment of the well newborn. Information is lacking regarding the implementation of such tools and their effects in clinical practice [10], Considering pain has a multidimensional nature, a multidimensional measurement, has been found to be superior to other ones and Neonatal Infant Pain Scale (NIPS) as a multidimensional measure fulfils this need [8].
In summary, although there are many evidences to support the efficacy of sucrose and glucose for management of pain in infants, the comparative efficacy of them on vaccination have not been clearly delineated. In the present study, researchers assess and compare the analgesic effects of orally administered glucose, sucrose and control.
Materials and Methods
This study is a controlled clinical trial for which the researchers, after receiving a written verification with the issue No:22/52/999/18 January 2012 by Ilam(western Iran) Medical University Ethics Committee, as well as a written permission signed by Head of Research, Deputy of Ilam University of Medical Sciences, referred to Shahid Mostafa Khomeini (Peace Be Upon Him) Hospital of Ilam (governmental and referral) and, besides observing Helsinki & Belmont statements, studied 90 neonates who had undergone vaccination for hepatitis-B between May 2013 and June 2013. The research has registered in Iranian Randomized Clinical Trials (IRCT 201304096790N3). It should be noted that researchers calculated the sample size based on the following formula:
The parents of studied cases signed informed consent for the trial instead of their infants. The inclusion criteria were: full term neonate, no receiving of analgesics, dryness of neonates diaper, awakeness of neonate, no receiving of nutrition during 30 minutes before vaccination, maximum of pain intensity 3 before intervention absences of diarrhea and common cold.
We excluded infant neonates that have history of anomality and preterm neonates. The cases were randomly (simple randomization method) divided into three groups of 30 neonates and received oral sucrose (2cc, 25%) or oral glucose (2cc, 25%) or no solutions (control group). The mentioned above solutions have given orally by syringe to neonate in 30 seconds, and 2 minutes later hepatitis-B vaccine injected by vaccinator, then, the pain level was measured using NIPS.
The Neonatal Infant Pain Scale provides a measure of the intensity of an infant's response to pain. On the basis of the literature review and the consideration of multiple tools, it was determined that the NIPS (Lawrence et al.,) would suit the hospital’s needs for assessing pain in well newborns. The NIPS assess six behavioural indicators in response to painful procedures in preterm and full-term newborns. This nonintrusive assessment includes facial expression, cry, breathing patterns, motor activity, and state of arousal. The calculated score measures the infants’ response to pain and allows the nurse to intervene accordingly. Scoring ranges from 0 to 1 in each category, with the exception of cry, which ranges from 0 to 2. A total score can range from 0 to 7. During the clinical trials and testing of the tool with an invasive procedure, newborns displayed a score of 1 before the procedure, a 5 during the procedure, and a 2 after the procedure. Extensive testing of the NIPS in clinical settings has demonstrated high inter rater reliability (Pearson correlations ranging from .92 to .97) and internal consistency (Cronbach’s alphas of .95, .87, and .88). In addition, construct and concurrent validity (Pearson correlations ranging from .53 to .84) were established (Lawrence et al.,) [10]. Checklists and questionnaires were used as the investigation means. The questionnaires contained demographic specifications of the studied cases, while the checklists included the data extracted from the pain level records. The observed data were analyzed using version 16 of SPSS Software as well as ANOVA and LSD tests. It is notable that we checked normal assumption and K.S test demonstrated that variables have normal distribution.
Results
Based on the obtained findings through ANOVA test, it showed that all of three groups of sucrose, glucose and control have no significant differences with each other in term of apgar score, delivery type, sex, head circumstance size , weight, height and gestational age (p-value were 0.376, 0.245, 0.444, 0.283, .0634, 0.883 and 0.40 respectively).
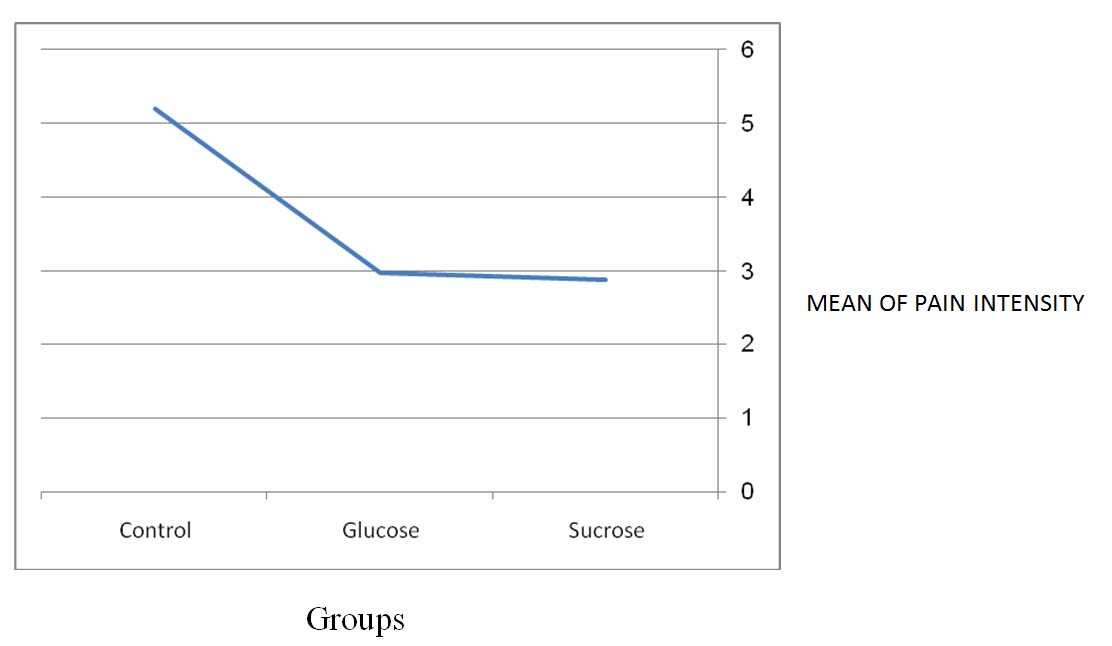
According to [Table/Fig-1,2] that demonstrate a comparison of average pain levels between the three groups, the average pain levels in sucrose, glucose receivers and control group were respectively as follow: 2.90±1.44, 3±1.66 and 5.20±1.03. ANOVA-test showed that, there were significant differences between the mean pain levels of the three groups, statistically (p<0.001), then paired comparisons of means were performed in term of findings that which of means is differ, we use LSD test, statistically significant differences were seen between the mean pain levels of the sucrose/glucose and control groups (p<0.001), but there was no significant difference between sucrose and glucose groups(p=0.78) [Table/Fig-3].
Comparison of pain intensity between the three groups
| Group | Frequency | Mean ±SD | p-value |
|---|
| Sucrose | 30 | 2.90±1.44 | <0.001 |
| Glucose | 30 | 3±1.66 |
| Control | 30 | 5.20± 1.03 |
Comparison of pain intensity between three groups
Pair comparison of means ± SD of pain intensity in three groups
| Groups | Pairs | Difference between Means in tow Groups | Difference between SDs in tow Groups | P-Value |
|---|
| Sucrose | Glucose | 0.10 | 0.36 | 0.78 |
| Control | 2.30 | 0.36 | <0.001 |
| Glucose | Sucrose | 0.10 | 0.36 | 0.78 |
| Control | 2.20 | 0.36 | <0.001 |
| Control | Sucrose | 2.30 | 0.36 | <0.001 |
| Glucose | 2.20 | 0.36 | <0.001 |
Discussion
Intervention by oral consumption of glucose or sucrose decreased the pain caused by vaccination. Considering the results, sucrose was more effective than glucose, but the difference was not statistically significant (p > 0.05).One systematic review in title of The Use of Oral Sucrose for Procedural Pain Relief in Infants Up to Six Months of Age: A Randomized Controlled Trial in 2010 has also demonstrated that Of the 695 studies 14 RCTs with 1674 injections showed that Sucrose or glucose, compared to water or no treatment decreased crying during or following vaccination in 13 of the 14 studies. Infants receiving 30% glucose (three trials, 243 infants) had a decreased RR in crying incidence following vaccination (typical RR 0.80, 95% CI 0.69 to 0.93; RD–0.17, 95% CI –0.29 to –0.05; NNTB 6, 95% CI 3 to20). With sucrose or glucose, there was a 10% WMD reduction in proportion of crying time (95% CI –18 to –2) and a 12 s reduction in crying duration (95% CI –23 to –0.7 s). The authors concluded that Sucrose and glucose also reduce pain during vaccination in infants up to 12 months of age [11].
Another study in 2007revealed that Sweet solution can be used as a simple and safe method to reduce the distress following vaccination in infants [12]. An older study in 1999 had concluded that the analgesic effects of concentrated sucrose and glucose and pacifiers are clinically apparent in newborns, pacifiers being more effective than sweet solutions. The association of sucrose and pacifier showed a trend towards lower scores compared with pacifiers alone. These simple and safe interventions should be widely used for minor procedures in neonates [4].
Considering in health care settings Analgesia is not provided routinely to infants who undergo vaccination, so we suggest (based on literature review and our study) the using of oral sucrose or glucose for relieving of pain caused by vaccination.
[1]. Suhrabi Z, Taghinejad H, A Comparative Study on the Efficacy of Ibuprofen and Celecoxib on the Intensity of Perineal Pain Following Episiotomy: A Randomized Clinical TrialIran Red Cres Med J 2013 15(12):e9980 [Google Scholar]
[2]. Taghinejad H, Delpisheh A, Suhrabi Z, Comparison between massage and music therapies to relieve the severity of labor painWomen’s Health 2010 6(3):377-81. [Google Scholar]
[3]. Gibbins S, Stevens B, Mechanisms of sucrose and non-nutritive sucking in procedural pain management in infantsPain research & management 2001 6(1):21-28. [Google Scholar]
[4]. Carbajal R, Chauvet X, Couderc S, Olivier-Martin M, Randomised trial of analgesic effects of sucrose, glucose, and pacifiers in term neonatesBmj 1999 319(7222):1393-97. [Google Scholar]
[5]. Wilson S, Bremner AP, Mathews J, Pearson D, The Use of Oral Sucrose for Procedural Pain Relief in Infants Up to Six Months of Age: A Randomized Controlled TrialPain Management Nursing 2013 14(4):e95-105. [Google Scholar]
[6]. Schechter NL, Zempsky WT, Cohen LL, McGrath PJ, McMurtry CM, Bright NS, Pain reduction during pediatric immunizations: evidence-based review and recommendationsPediatrics 2007 119(5):e1184-98. [Google Scholar]
[7]. Gradin M, Schollin J, The role of endogenous opioids in mediating pain reduction by orally administered glucose among newbornsPediatrics 2005 115(4):1004-07. [Google Scholar]
[8]. Gradin M, Finnström O, Schollin J, Feeding and oral glucose—additive effects on pain reduction in newbornsEarly human development 2004 77(1):57-65. [Google Scholar]
[9]. Olson TL, Downey VW, Infant physiological responses to noxious stimuli of circumcision with anesthesia and analgesiaPediatric nursing 1998 24(4):385 [Google Scholar]
[10]. Gallo AM, The fifth vital sign: implementation of the Neonatal Infant Pain ScaleJournal of Obstetric, Gynecologic, & Neonatal Nursing 2003 32(2):199-206. [Google Scholar]
[11]. Harrison D, Stevens B, Bueno M, Yamada J, Adams-Webber T, Beyene J, Efficacy of sweet solutions for analgesia in infants between 1 and 12 months of age: a systematic reviewArchives of disease in childhood 2010 95(6):406-13. [Google Scholar]
[12]. Thyr M, Sundholm A, Teeland L, Rahm VA, Oral glucose as an analgesic to reduce infant distress following immunization at the age of 3, 5 and 12 monthsActa Paediatrica 2007 96(2):233-36. [Google Scholar]