Congenital Mucous Retention Cyst of the Anterior Hard Palate! the First Case Report
Satya Ranjan Misra1, Smita Priyadarshini2, Abhishek Ranjan Pati3, Sanat Kumar Bhuyan4, Rajat G Panigrahi5
1Reader, Department of Oral Medicine & Radiology, Institute of Dental Sciences, Bhubaneswar, Orissa, India.
2Senior Lecturer, Department of Oral Medicine & Radiology, Institute of Dental Sciences, Bhubaneswar, Orissa, India.
3Senior Lecturer, Department of Oral Medicine & Radiology, Institute of Dental Sciences, Bhubaneswar, Orissa, India.
4Professor & Head, Department of Oral Medicine & Radiology, Institute of Dental Sciences, Bhubaneswar, Orissa, India.
5Senior Lecturer, Department of Oral Medicine, Institute of Dental Sciences, Bhubaneswar, Orissa, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Satya Ranjan Misra, ‘Prasanti’, Kathogola Road, Mangalabag, Cuttack-753001, Odisha, India. Phone : 9937992558,
E-mail: drsatyaranjanmds@gmail.com
Children may be born with birth defects, the most common being oro-facial clefts and fissural cysts. A well circumscribed pedunculated soft tissue growth that occurs congenitally is known as congenital epulis of the newborn or ‘Neuman’s Tumour’ as described in the literature. It is a rare lesion and the diagnosis has to be confirmed histologically. We present a rare case of a 7-year-old child with a congenital growth in the pre-maxillary region of the anterior hard palate clinically diagnosed as congenital epulis however, histologically confirmed as a mucous retention cyst. An elaborate clinical differential diagnosis is discussed. The anterior hard palate is devoid of salivary glands and the presence of a mucous retention cyst in the area is suggestive of ectopic salivary gland tissue and in a child manifesting at birth is probably the first case to be reported in the English literature.
Anterior hard palate, Congenital epulis, Ectopic salivary gland tissue, Mucous retention cyst
Case Report
A 7-year-old female child reported to the dental hospital with a complaint of a growth in the palate since birth. History revealed that the patient was born with a minute growth on the palate which has slowly grown with time. The spacing between the maxillary central incisors increased due to the growth but there was no pain or any discharge associated with the growth. The medical history was non-contributory.
On clinical examination, a single well circumscribed ovoid swelling was seen in the midline of the hard palate in the region of the incisive papilla,[Table/Fig-1] measuring 1x 0.5cm in size, of the mucosal colour, pedunculated, smooth surfaced without any secondary changes, soft in consistency and non-tender on palpation. There was no blanching or discharge associated with the swelling on palpation.
Correlating the history of the lesion being present at birth and clinical findings of an asymptomatic, pedunculated soft tissue growth in the anterior maxillary ridge a provisional diagnosis of congenital epulis was made.
The differential diagnosis of the lesion included the following:
• Irritational fibroma
• Pyogenic granuloma
• Peripheral giant cell granuloma
• Peripheral ossifying fibroma
• Peripheral odontogenic tumour
• Nasopalatine duct cyst
• Neurofibroma/Schwannoma
• Oral myofibroma
• Leiomyomatous hamartoma
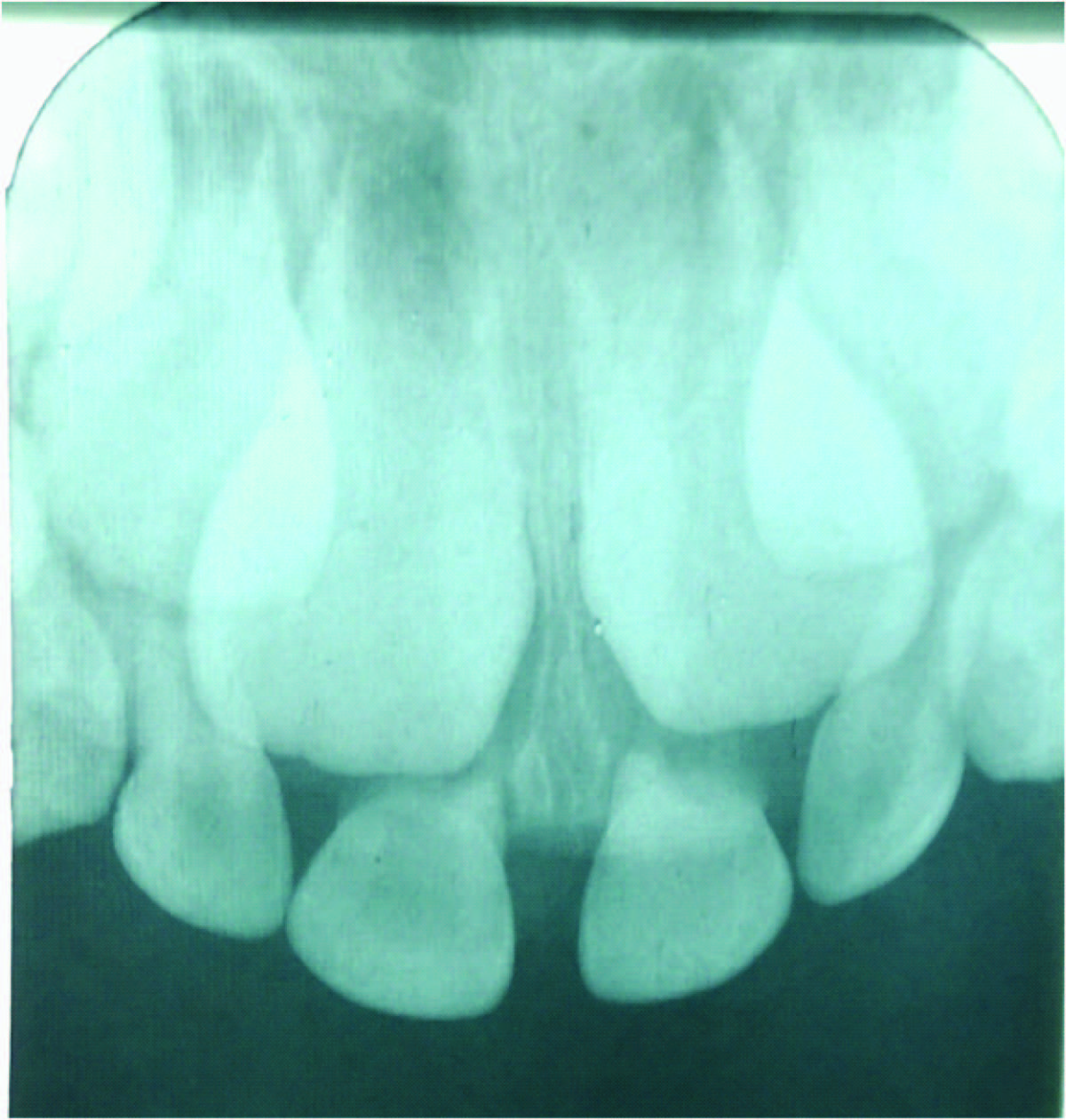
An intraoral periapical radiograph of the anterior maxilla was taken but did not reveal any bony abnormality [Table/Fig-2]. The growth was excised and sent for Histopathologic examination.
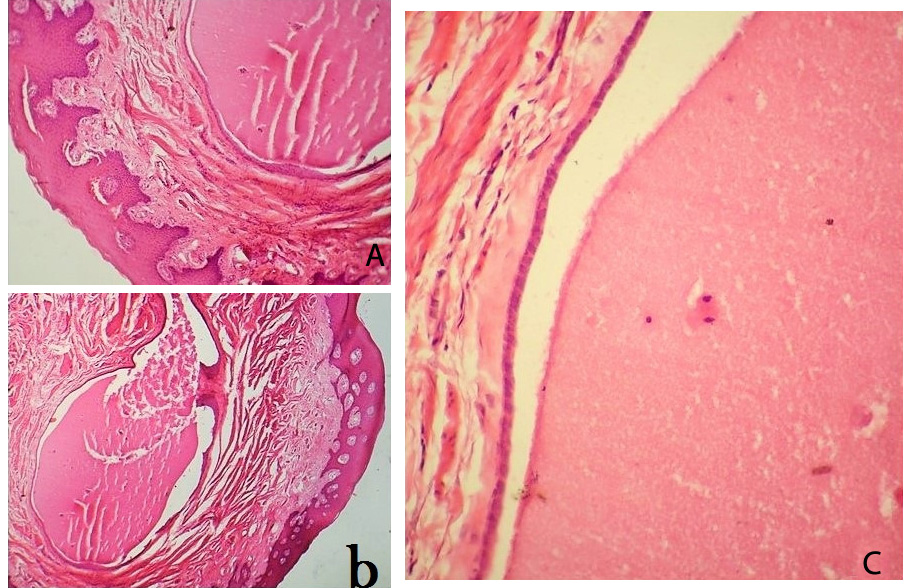
Hematoxylin-Eosin (H & E) stained section revealed parakeratinized stratified squamous eithelium with pseudoepitheliomatous like hyperplasia overlying the loosely arranged connective tissue stroma [Table/Fig-3a] magnification 4x. Submucosa is showing expanded glandular ductal (bilayered, cuboidal) epithelium enclosing mucin inside [Table/Fig-3b] magnification 10x. The ductal lining is intact throughout, inflammatory cell infiltrate is not seen [Table/Fig-3c] magnification 40x. Histopathologic findings were suggestive mucous retention cyst.
The entire growth had been excised with uneventful healing in two weeks after surgery.
Discussion
Congenital oral lesions are a cause of anxiety and apprehension to the parents even if they are asymptomatic. Though uncommon and benign few lesions can suddenly grow into bizarre size and interfere with feeding or swallowing.
Congenital epulis is a rare benign lesion, first described by Neumann in 1871. It manifests at birth predominantly in new born girls, with a female: male ratio of 10:1 [1]. It presents as a solitary, well circumscribed, smooth, pedunculated, polypoid nodular growth located on the anterior maxillary alveolar ridge as in the present case [2]. It is an intriguing lesion with uncertain aetiology and pathogenesis but the final diagnosis is dependent on histopathological evaluation.
However, a focal soft tissue growth on the palate needs to be differentiated from clinically similar lesions. A clinical differential diagnosis includes a number of lesions some of which are commonly encountered while others are quite rare. Since the maxillary anterior alveolar ridge (anterior hard palate) and gingiva are devoid of salivary glands tissue, lesions of minor salivary glands were not considered and owing to the soft consistency of the lesion bony lesions were also ruled out. The differential diagnosis is elaborately discussed in the [Table/Fig-4] [3-11].
The histopathologic diagnosis of a mucous retention cyst was contrary to all clinical assumptions and a pubmed search of the English literature did not reveal any case reported in the anterior hard palate /maxillary alveolar ridge.
A mucus retention cyst is a true non-odontogenic soft tissue cyst, lined with epithelium. It usually occurs as a result of epithelial proliferation of a partially or completely obstructed salivary duct [12]. Obstruction of salivary glands commonly occurs due to mucin plugs around which there is calcification gradually resulting in a sialolith. In the present case probably ectopic salivary gland tissue was entrapped in the mucosa following fusion of the anterior palate during development which due to epithelial proliferation formed a mucous retention cyst in such an unusual location and appeared as a congenital asymptomatic mass.
Intra-oral picture showing a well circumscribed, smooth, ovoid, pedunculated soft tissue growth in the midline of the hard palate

Maxillary anterior periapical radiograph showing mixed dentition stage without any bony abnormalities
(a) H & E stained section showing parakeratinized stratified squamous eithelium with pseudoepitheliomatous like hyperplasia overlying the loosely arranged connective tissue stroma.
(b) Submucosa is showing expanded glandular ductal epithelium enclosing mucin inside.
(C) The ductal lining is intact throughout, inflammatory cell infiltrate is not seen
Clinical differential diagnosis of focal soft tissue growth
| Lesion | Features |
| 1. | Irritational/ Traumatic Fibroma (Focal fibroepithelial hyperplasia/ Fibroepithelial Polyp) | Common reactive oral soft tissue lesion History of trauma or clinical signs of trauma present. |
| 2. | Pyogenic Granuloma | Common reactive gingival lesion which occurs due to irritation from local factors like calculus and plaque or accentuated during hormonal changes such as pregnancy. Manifests as painless, sessile gingival or mucosal growth, bleeds on provocation, soft in consistency. |
| 3. | Reactive mucosal lesion occurring exclusively on the gingiva/alveolar mucosa in adult women. Seen as a rapidly growing, sessile reddish lesion causes pressure erosion of the underlying bone. Mild bone erosion seen on radiographs. | Peripheral giant cell granuloma |
| 4. | Peripheral ossifying fibroma | Reactive soft tissue lesion that is often seen in the gingiva/ alveolar mucosa of the maxillary anterior region. Generally the lesions are paler and firm in consistency with surface ulceration secondary to trauma due to masticatory forces. Radiographs might exhibit calcifications. |
| 5. | nasopalatine duct cyst or incisive canal cyst | Most common non-odontogenic cyst of the maxilla originating from the epithelial remnants from the nasopalatine duct. It presents as a sessile swelling in the region of the incisive papilla, commonly reported in middle aged and elderly patients, either asymptomatic or the lesion is secondarily infected and painful. A well circumscribed ovoid or heart shaped radiolucency is observed in the midline on periapical radiographs of the maxillary incisors. |
| 6. | Peripheral (extra-osseous) odontogenic tumours | Peripheral (extra-osseous) odontogenic tumours though rare, can occur as a result of the remnants of the odontogenic epithelium entrapped in oral soft tissues which undergoes differentiation forming peripheral odontogenic tumours. Some of the lesions under this category can be hamartomatous and not true neoplasms they can occur at an early age however bony alterations due to the lesion or other radiographic changes may be evident. |
| 7. | Oral myofibroma | Rare soft tissue lesion reported in different intraoral sites, like the maxillary labial mucosa, tongue, gingiva and palate. |
| 8. | Neural lesions like Schwannoma, Neurofibroma and Traumatic Neuroma | Uncommonoral lesions but they may also present as solitary soft tissue asymptomatic masses. |
| 9. | Leiomyomatous hamartoma | Extremely rare oral soft tissue lesion which can occur as an asymptomatic mass in young children at birth although its occurrence in anterior palate is extremely rare. |
Conclusion
Congenital oral lesions are uncommon but such cases do report to Pediatrician/Dental surgeon and hence it is important for them to know the differential diagnosis of such entities. Common lesions sometimes pose a diagnostic dilemma and clinical diagnosis may rarely defy the accepted knowledge of the diseases surprising the clinician with an unusual manifestation. The present case of a mucous retention cyst in the anterior hard palate which is generally devoid of salivary gland tissue as a congenital, asymptomatic lesion emphasizes the utility of Histopathologic evaluation as a gold standard of diagnosis.
[1]. B Neville, DD Damm, CM Allen, J Bouquot, J. Oral and Maxillofacial Pathology 2009 3rd EditionPhiladelphiaSaunders [Google Scholar]
[2]. A Bewley, JD Bloom, S Kherani, BR Pawel, Congenital epulis.Ear Nose Throat J. 2010 89:299-300. [Google Scholar]
[3]. Ramu Sangeetha Rodrigues Charlotte, Reactive hyperplastic lesions of the gingiva: A retrospective study of 260 cases.World 2012 3(2):126-30. [Google Scholar]
[4]. JM Moffitt, RO Cooley, NH Olsen, JJ Hefferren, Nasopalatine Duct Cyst. Nelson BL, Linfesty RL.Head and Neck Pathol 2010 4:121-22. [Google Scholar]
[5]. S Azevedo R de, FR Pires, R Della Coletta, OP de Almeida, LP Kowalski, MA Lopes, Oral myofibromas: report of two cases and review of clinical and histopathologic differential diagnosis.Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008 105:35-40. [Google Scholar]
[6]. F Ide, K Obara, K Mishima, I Saito, N Horie, T Shimoyama, Peripheral odontogenic tumor: a clinicopathologic study of 30 cases. General features and hamartomatous lesions.J Oral Pathol Med. 2005 34:552-57. [Google Scholar]
[7]. P Ritwik, RB Brannon, Peripheral odontogenic fibroma: a clinicopathologic study of 151 cases and review of the literature with special emphasis on recurrence.Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010 110:357-63. [Google Scholar]
[8]. HP Philipsen, PA Reichart, JJ Sciuba, I van der Waal, Odontogenic fibroma. In: World Health Organization classification of tumors. Pathology and Genetics— Head and Neck Tumors.Lyon:IARC 2005 :315 [Google Scholar]
[9]. AR Silva, R Carlos-Bregni, PA Vargas, OP de Almeida, MA Lopes, Peripheral developing odontoma in newborn. Report of two cases and literature review.Med Oral Patol Oral Cir Bucal. 2009 14:612-15. [Google Scholar]
[10]. E Chrysomali, SI Papanicolaou, NP Dekker, JA Regezi, Benign neural tumors of the oral cavity: a comparative immunohistochemical study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997 84:381-90. [Google Scholar]
[11]. SS Napier, JC Devine, JS Rennie, PJ Lamey, Unusual leiomyomatous hamartoma of the hard palate: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996 82:305-07. [Google Scholar]
[12]. AM Hayashida, DCZ Zerbinatti, I Balducci, LAG Cabral, JD Almeida, Mucous extravasation and retention phenomena: A 24-year study.BMC Oral Health. 2010 :10-15. [Google Scholar]