Introduction: Fine needle aspiration cytology (FNAC) is a well-established first line diagnostic tool in evaluating palpable thyroid lesions. However, the technique depends on suction and thus is at times painful, sometimes traumatic and yield haemorrhagic material for cytological study. In more recent times, a modified technique called fine needle sampling without aspiration (FNS) has come into vogue which obviates the use of suction and therefore is more patient friendly.
Aims/Objectives: To investigate whether fine needle sampling without aspiration (FNS) gives quantitatively and qualitatively superior cytologic material as compared to the conventional technique of fine needle aspiration (FNAC) in thyroid lesions.
Materials and Methods: It is a prospective study of 200 cases carried out in the Department of Pathology during two years period. Both techniques were executed on the same thyroid swelling / nodule in the same clinical session beginning with FNS followed by FNAC. The observation recorded by two pathologists were based on the scoring system proposed by Mair et al., Statistical analysis was done by Student’s paired t-test using SPSS 13 software.
Observation/Results: A total of 200 cases were studied. The non-aspiration technique yielded less diagnostically adequate but more diagnostically superior smears when compared with aspiration technique. The average score per case was 5.31 by aspiration technique and 6.35 by non-aspiration technique.
Conclusion: Both the techniques have their own merits and demerits and neither is absolutely superior to the other. A combination of both the technique gives better result.
Introduction
At the beginning of 20th century fine needle aspiration cytology (FNAC) of lymph nodes was attempted by various investigators for diagnosing diseases like trypanosomiasis, lymphoblastoma and Hodgkins disease [1,2]. During 1930s, Martin and Ellis from Memorial Hospital, New York, came up with the first large scale report on FNAC of 65 cases [3]. During the 1940s, enthusiasm for FNAC was possibly dampened by a few reports highlighting the negative aspects of FNAC [4]. S. Franzen, J.Zajicek, N. Soderstrom and others revived interest in FNAC during the 1960s and it became widespread throughout Scandinavia & later on spread to other European countries and USA.
Fine needle aspiration as a diagnostic tool in cytopathology was introduced in India, initially by M.S. Sukumaran in Madras (now Chennai) and by Subhash Kumari Gupta in PGIMER Chandigarh, in the early 1970s, after their training in Scandinavia [5]. Now a days FNAC is routinely performed in all superficial palpable mass lesions and also for deep seated lesions under ultrasonograph (USG)/computed tomography (CT) guidance.
A major criticism of FNAC, however, pertains to its use in highly vascular organs, such as thyroid and liver, or in haemorrhagic lesions where large quantities of blood compromise cytologic interpretation. In addition, suction may traumatize delicate cells, which causes distortion of appropriate cytoarchitecture, and consequently, cytologic assessment is compromised even further [6].
More recently, a modified technique called fine needle sampling without aspiration (FNS) / fine needle non aspiration cytology (FNNAC) has come into vogue. This technique also known as Cytopuncture was developed by Brifford et al., in France in 1982 [7]. This technique depends solely on capillary action of the fine needle; Therefore is less painful, less traumatic and thus much more patient friendly.
Fine needle sampling without aspiration is less commonly used but often easier to perform. Both methods have advantages and disadvantages but, as yet, there is no agreement on which method produces better specimens for cytological diagnosis.
Although fine needle sampling technique has been adopted for various organs [8,9], the high vascular nature of thyroid, leading to haemorrhagic smears and discomfort to the patient by conventional technique, made us to concentrate on this organ before embarking on a wider study including various other organs.
Aim of the Study
To investigate whether fine needle sampling (FNS) gives quantitatively and qualitatively superior cytologic material as compared to the conventional technique of fine needle aspiration (FNA) in thyroid lesions.
Objective
To perform FNS and FNA on the same thyroid lesion and to assess the smear morphology based on criteria proposed by Mair S et al., [10].
Materials and Methods
It is a prospective case control study of 200 cases carried out in the Department of Pathology over a period of two years. All the cases of palpable thyroid lesions referred to the Department of Pathology by various clinical departments including Endocrinology, General Surgery, Surgical Oncology and cases referred from outside hospitals were subjected to both FNS and FNA technique.
All the cases of palpable thyroid lesions were included in the study irrespective of consistency, size of lesions, age and sex of the patients. Cases of non-palpable thyroid lesions requiring imageological guided FNA and patients not willing to participate in the study were excluded from the study. Institutional Ethics committee approval was taken for the study. The procedure was explained to the patient and written consent was obtained prior to performing the procedure.
Examination of the thyroid was done with the patient in upright position and noticing the swelling during deglutition. Aseptic conditions were maintained by using hand gloves and cleaning the thyroid swelling with povidone-iodine solution followed by spirit. During the procedure the patient was asked to keep still and to refrain from swallowing. Both techniques were executed on the same thyroid swelling / nodule in the same clinical session beginning with FNS followed by FNAC. First a 24 gauge needle was put in the thyroid swelling. The needle held between thumb and forefinger of aspirating hand was inserted into the nodule and moved in different directions within the nodule. The material entering the hub of the needle by capillary action was then expressed onto already labelled clean glass slide after attaching an air filled syringe to it. Next a 24 gauge needle with 10ml syringe attached to it was used for aspiration from the same thyroid swelling. The material obtained was similarly spread over a glass slide. Uniform, thin, evenly spread smears were obtained by superimposing another glass slide (spreader) at right angle to the slide with the expressed cellular material sandwiched between them, exerting gentle optimal pressure for a few seconds and then rapidly pulling the slides apart horizontally, resulting in well spread smear. One glass slide each was kept for drying and others put in isopropyl alcohol for wet smear preparation. The dry smears were stained by Leishman and May-Grunwald-Giemsa (MGG) stains and wet smears with Hematoxylin & Eosin stain.
In a couple of cases there was no cellularity by either method and in such cases repeat FNAC was performed using only aspiration technique and those smears were used purely for diagnostic purposes and were not included in the study. The observation of the present study was based on the parameters of scoring system proposed by Mair S et al., [10] [Table/Fig-1]. The two sampling techniques were compared using five objective parameters.
Mair S et al., Scoring system [10]
| Sl. No | Criterion | Qualitative description | Score | Score |
|---|
| Sampling | Aspiration |
|---|
| No. | A | No. | A |
|---|
| 1. | Background blood / clot | Large amount / great compromise to diagnosis | 0 | | | | |
| Moderate / diagnosis possible | 1 | | | | |
| Minimal / diagnosis easy; specimen of textbook quality | 2 | | | | |
| 2. | Amount of cellular material | Minimal to absent / diagnosis not possible | 0 | | | | |
| Sufficient for diagnosis | 1 | | | | |
| Abundant / diagnosis simple | 2 | | | | |
| 3. | Degree of cellular degeneration | Marked / diagnosis impossible | 0 | | | | |
| Moderate / diagnosis possible | 1 | | | | |
| Minimal / good preservation; diagnosis easy | 2 | | | | |
| 4. | Degree of cellular trauma | Marked; diagnosis impossible | 0 | | | | |
| Moderate; diagnosis possible | 1 | | | | |
| Minimal; diagnosis easy | 2 | | | | |
| 5. | Retention of appropriate architecture | Minimal to absent / non diagnostic | 0 | | | | |
| Moderate / some preservation | 1 | | | | |
| Excellent architecture display, closely reflecting histology | 2 | | | | |
| 6. | Total | | 10 | | | | |
All available cytologic smears were initially handled for clinical diagnostic purposes, immediately after that they were assessed by two pathologists separately for the study purpose and scoring performed. An average score of the two pathologists was taken for each parameter as well as for each case. A cumulative score between 0 and 10 points was obtained for each specimen which was then categorized into one of the following three categories:
Category 1(Score 0–2): Unsuitable for diagnosis
Category 2(Score 3–6): Adequate for cytological diagnosis
Category 3(Score 7–10): Diagnostically superior.
Comparison between the two techniques was done by Student’s paired t-test using SPSS 13 software. All the results were analysed considering the statistical significance at a level of p<0.05.
Results
A total of 200 cases were studied. The youngest patient was 9y female and the oldest 80y female. There were 26 males and 174 females (1:6.7).
The non-aspiration technique yielded less diagnostically adequate but more diagnostically superior smears when compared with aspiration technique [Table/Fig-2].
The category wise performance of FNAC and FNS technique
| Performance | FNAC (n=200) | FNS (n=200) |
|---|
| Diagnostically superior (Score 7-10) | 43(21.5%) | 93(46.5%) |
| Diagnostically adequate (Score 3-6) | 130(65%) | 94(47%) |
| Diagnostically unsuitable (Score 0-2) | 27(13.5%) | 13(6.5%) |
The average score per case was 5.31 by aspiration technique and 6.35 by non-aspiration technique [Table/Fig-3].
Average score for each parameter
| Parameter | FNAC | FNS | p-value |
|---|
| Background blood / clot | 0.9350 | 1.0825 | 0.001 |
| Amount of cellular material | 1.230 | 1.0825 | 0.003 |
| Degree of cellular degeneration | 1.0825 | 1.4625 | <0.001 |
| Degree of cellular trauma | 1.1175 | 1.490 | <0.001 |
| Retention of appropriate architecture | 0.9475 | 1.2350 | <0.001 |
Discussion
FNAC, since its inception in 1847, has passed through two phases of initial scepticism and interim enthusiasm and has successfully reached the final stage of acceptance as identified by Orell in his analysis of steps by which the assessment of innovative diagnostic practice progresses [11].
It has been suggested that fine needle sampling technique, by eliminating the negative suction pressure employed in FNAC, decreases the dilution of cells by blood and the scientific basis of which was explained by Santos and Leiman [12]. The technique employing the insertion of fine needle into a lesion without attachment of a syringe depends on the property of capillary tension in narrow channel. The physical principle is to state that a fluid or a semisolid substance will ascend spontaneously in a narrow tube in reverse proportion to diameter of tube or capillary.
The ascent of fluid into a narrow channel is governed by the formula h=2T/pgr, where h is the height attained, T is the surface tension of the fluid, p is density of the fluid, g is the gravity and r is radius of the capillary tube [12].
Although both aspiration and non-aspiration techniques use syringe and needle, in FNS the syringe is used to expel the material after the procedure is completed, whereas in FNA it is used to create a suction force to aspirate the cells in to the needle. A fresh sterile syringe is therefore not necessary for FNS, thus reducing the cost of procedure.
The patient also would be much less apprehensive when a large syringe, a syringe holder and a needle are not seen. Thus FNS is obviously more patient friendly [13]. FNS allows greater ease of sampling with better control of the hand during the procedure and a good perception of the lesion consistency, enabling more precise entry into the mass and thus more user friendly also [8].
The disadvantage of FNS technique observed in our study was whenever there was a colloid cyst or cystic degeneration – immediately brownish colloidal fluid drained out and drenched the fingers holding the needle. This problem was handled by keeping a syringe ready, which was immediately attached to the needle and the fluid collected in the syringe – to be cyto-centrifuged for better cellularity.
Our practical experience of using FNS technique in organs other than thyroid found its limitation in yielding scant material in calcific, fibrous and hard lesions and also in very soft lesions like lipoma. In such cases one has to compulsorily go for aspiration technique.
Limitations
Diagnostic accuracy: We have not evaluated the two techniques based on the diagnosis as done in some studies by Raghuveer CV et al., [8] and Romitelli F et al., [14]. In both the studies the diagnostic accuracy was better for FNS as compared to FNAC. In addition Raghuveer CV et al., [8], also concluded that FNS was better for diagnosing malignant lesions whereas FNAC was better for benign lesions.
Order of Sampling: In our study for all the 200 cases we performed first FNS technique followed by FNA. In the study by Mair S et al., [10] and Romitelli F et al., [14] and Kamal MM et al., [15] in half cases they performed FNA technique first and vice-versa and came up with the result that there was no statistically significant difference between the scores of FNA and FNS whether performed as the first or second technique.
Blinding: Studies by Savage CA et al., [6], SA Ali Rizvi et al., [16] and L Ramchandra et al., [17] have done blinding for the technique employed but in all the said studies although observer bias for the technique was avoided but the possibility of inter-observer bias was not taken care of as the observation was made by a single pathologist.
Similar to Raghuveer CV et al., [8], in our study two experienced pathologists studied and scored the smears and an average of the two was taken as final score, thereby eliminating the inter-observer bias.
Our results when compared for background blood contamination [Table/Fig-3] supported the non-aspiration technique in the present study similar to most of the studies including those by Kamal MM et al., [15], Maurya AK et al., [18] and Mahajan P et al., [19] except one study by Mair S et al., [10] who found more blood in sampling technique. The amount of cellular yield was found to be better by aspiration technique in the present study similar to reported by Mair S et al., [10] and contrary to the result by Kamal MM et al.,[15], Maurya AK et al., [18] and Mahajan P et al., [19] who reported more cellular smears by sampling technique.
Cellular degeneration and trauma were more in aspiration technique [Table/Fig-4] in the present study similar to the studies by Mahajan P et al., [19], Maurya AK et al., [18] and whereas Mair S et al., [10] is the only study who reported more degeneration and trauma by sampling technique. Kamal MM et al., [15] had more degeneration by sampling technique whereas trauma was more in aspiration technique. In the present study the sampling smears yielded better retention of architecture [Table/Fig-5] similar to the findings reported by Mahajan P et al., [19], Kamal MM et al., [15] and Maurya AK et al., [18] whereas Mair S et al., [10] is the only study who reported better maintenance of cell architecture by aspiration technique.
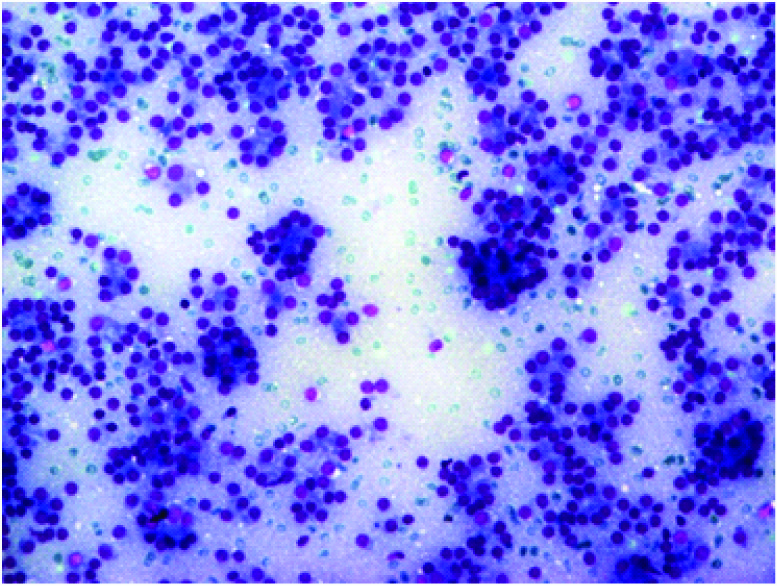
Aspiration smear from thyroid shows rich cellularity, abundant blood in the background, entangled follicular cells with ill-preserved architecture and degeneration and trauma to cells [H&E x 40]

Photomicrograph from FNS technique smear showing richly cellular smear with well-preserved microfollicular cell clusters/rosettes in a repetitive pattern with minimal blood in the background [MGG x 100]
There was statistically significant difference in favour of non-aspiration technique in our study similar to that observed by Dey and Ray [20] and SA Ali Rizvi et al., [16]. Kamal MM et al., [15] had statistically significant difference for the parameter of ‘amount of cellularity’. Romitelli F et al., [14] reported statistically significant result only in case of number of inadequate smears, which were more by aspiration technique. In studies by Mair S et al., [10] and Maurya AK et al., [18] there was no statistically significant difference in the two techniques.
Studies by Mair S et al., [10], Raghuveer CV et al., [8] and Ghosh A et al., [9] included multiple site FNACs including thyroid, lymph node, breast, salivary gland, liver and soft tissues. Raghuveer CV et al., [8] didn’t categorise the cases into diagnostically superior, adequate and unsuitable as done by others.
In the present study, more diagnostically superior and less diagnostically adequate samples were obtained by non-aspiration technique in comparison to aspiration technique [Table/Fig-6], which was similar to the results obtained by Maurya AK et al., [18] and Mahajan P et al., [19] and contrary to Santosh & Leiman [12]. Kamal MM et al., [15] reported both diagnostically superior as well as adequate samples more by sampling technique.
Comparative table with other studies
| Sl no. | Total no of cases | FNAC | FNS |
|---|
| DS | DA | U | DS | DA | U |
|---|
| Santos & Leiman [12] | 50 | 22 | 25 | 3 | 4 | 39 | 7 |
| Kamal MM et al., [15] | 200 | 88 | 46 | 66 | 99 | 54 | 47 |
| Maurya AK et al., [18] | 50 | 20 | 12 | 18 | 23 | 8 | 18 |
| Mahajan P et al., [19] | 50 | 8 | 12 | 30 | 10 | 4 | 36 |
| Present study | 200 | 43 | 130 | 27 | 93 | 94 | 13 |
DS=Diagnostically superior, DA=Diagnostically adequate, U=Unsuitable
In our study even when the aspiration technique is suggestive of higher cellular yield, the number of unsuitable cases was more in aspiration technique. This paradox may be because of the more haemorrhagic aspirate leading to entanglement of the cellular component in the blood clot and thus yielding diagnostically inadequate smears.
Conclusion
In our study we found non-aspiration technique to be better in relation to less blood in the background, less degeneration and trauma to cells and better preservation of cellular architecture. Aspiration technique yielded better cellularity as compared to non-aspiration technique.
Both the techniques have their own merits and demerits and neither is absolutely superior to the other. It thus falls upon the individual operator to select a technique of personal preference. A combination of both the technique gives better result.
We propose first fine needle sampling should be performed and only if the amount of cellular material is not adequate, repeat with aspiration technique should be performed.
DS=Diagnostically superior, DA=Diagnostically adequate, U=Unsuitable
[1]. Ward GR, In: Bedside Hematology 1914 PhiladelphiaWB Saunders Company:129 [Google Scholar]
[2]. Guthrie CG, Gland punctures as a diagnostic measureJohns Hopkins Hosp Bull 1921 32:266-69. [Google Scholar]
[3]. Martin HE, Ellis EB, Biopsy by fine needle puncture and aspirationsAnn Surg 1930 92:169-81. [Google Scholar]
[4]. Johening PW, A history of aspiration biopsy with special attention to prostate biopsyDiagn Cytopathol. 1988 4:265-68. [Google Scholar]
[5]. Das DK, Fine-needle aspiration cytology: its origin, development and present status with special reference to a developing country, IndiaDiagn Cytopathol 2003 28:345-51. [Google Scholar]
[6]. Savage CA, Hopper KD, Abendroth CS, Hartzel JS, TenHave TR, Fine-needle aspiration biopsy versus fine-needle capillary (nonaspiration) biopsy: in vivo comparisionRadiology. 1995 195:815-19. [Google Scholar]
[7]. Briffod M, Gentile A, Hebert H, Cytopuncture in the follow-up of breast carcinomaActa Cytol 1982 26:195-200. [Google Scholar]
[8]. Raghuveer CV, Leekha I, Pai MR, Adhikari P, Fine Needle Aspiration cytology versus Fine Needle Sampling without aspiration. A prospective study of 200 casesIndian J Med Sci. 2002 56:431-39. [Google Scholar]
[9]. Ghosh A, Mishra RK, Sharma SP, Singh HN, Chaturvedi AK, Aspiration vs nonaspiration technique of cytodiagnosis--a critical evaluation in 160 casesIndian J Pathol Microbiol 2000 43:107-12. [Google Scholar]
[10]. Mair S, Dunbar F, Becker PJ, Du Plessis W, Fine needle cytology--is aspiration suction necessary? A study of 100 masses in various sitesActa Cytol 1989 33:809-13. [Google Scholar]
[11]. Orell SR, Fine needle aspiration in perspectivePathology. 1982 14:113-14. [Google Scholar]
[12]. Santos JE, Leiman G, Nonaspiration fine needle cytology. Application of a new technique to nodular thyroid diseaseActa Cytol 1988 32:353-56. [Google Scholar]
[13]. Rajasekhar A, Sundaram C, Chowdhary T, Charanpal M, Ratnakar KS, Dignostic utility of fine-needle Sampling without aspiration: a prospective studyDiagn Cytopathol. 1991 7:473-76. [Google Scholar]
[14]. Romitelli F, Di Stasio E, Santoro C, Lozzino M, Orsini A, Cesareo R, A comparative study of fine needle aspiration and fine needle non-aspiration biopsy on suspected thyroid nodulesEndocr Pathol. 2009 20:108-13. [Google Scholar]
[15]. Kamal MM, Arjune DG, Kulkarni HR, Comparative study of fine needle aspiration and fine needle capillary sampling of thyroid lesionsActa Cytol. 2002 46:30-34. [Google Scholar]
[16]. Rizvi SA Ali, Husain M, Khan S, Mohsin M, A comparative study of fine needle aspiration cytology versus non-aspiration technique in thyroid lesionsSurgeon. 2005 3:273-76. [Google Scholar]
[17]. Ramachandra L, Kudva R, Rao BHA, Agrawal S, A Comparative Study of Fine Needle Aspiration Cytology (FNAC) and Fine Needle Non-aspiration Cytology (FNNAC) Technique in Lesions of Thyroid GlandIndian J Surg. 2011 73:287-90. [Google Scholar]
[18]. Maurya AK, Mehta A, Mani NS, Nijhawan VS, Batra R, Comparison of aspiration vs non-aspiration techniques in fine-needle cytology of thyroid lesionsJ Cytol. 2010 27:51-54. [Google Scholar]
[19]. Mahajan P, Sharma PR, Fine-Needle Aspiration Versus Non Aspiration Technique of Cytodiagnosis in Thyroid LesionsJK Science 2010 3:120-22. [Google Scholar]
[20]. Dey P, Ray R, Comparison of fine needle sampling by capillary action and fine needle aspirationCytopathology. 1993 4:299-303. [Google Scholar]