Angiomyolipomas, Renal Cell Carcinomas and Pulmonary Lymphangioleiomyomatosis
Panagiotis J Vlachostergios1, Bahareh Soroori Rad2, Kamran Karimi3, George Apergis4
1 Faculty, Department of Internal Medicine, Lutheran Medical Center, Brooklyn, New York, USA.
2 Faculty, Department of Internal Medicine, Lutheran Medical Center, Brooklyn, New York, USA.
3 Faculty, Department of Internal Medicine, Lutheran Medical Center, Brooklyn, New York, USA.
4 Faculty, Division of Pulmonary and Critical Care Medicine, Lutheran Medical Center, Brooklyn, New York, USA.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Panagiotis J Vlachostergios, 150 55th Street, Brooklyn, New York-11220, USA. E-mail : pvlachostergios@lmcmc.com
Angiomyolipoma, Lymphangioleiomyomatosis, Renal cell carcinoma, Tuberous sclerosis
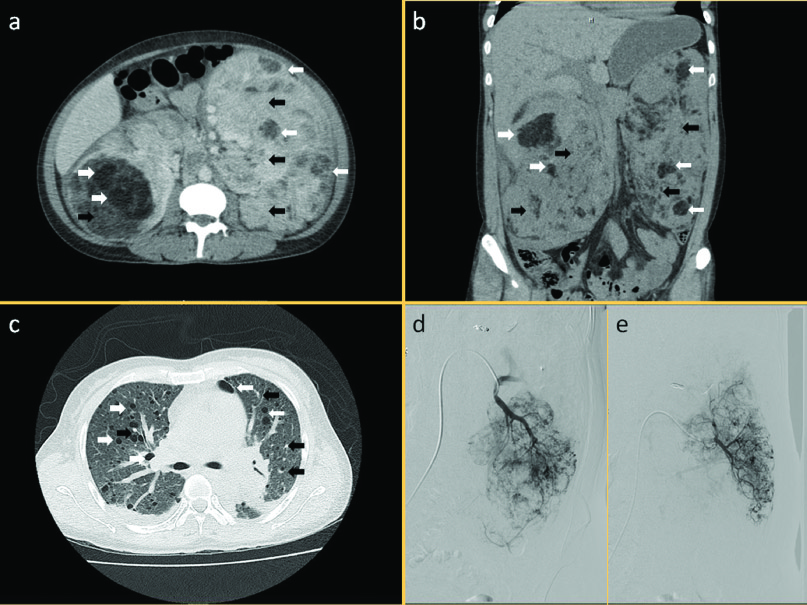
A 46-year-old female presented with worsening bilateral flank and abdominal pain. Abdominal CT revealed bilateral enlarged kidneys containing lesions suggestive of multiple angiomyolipomas (AML) and bilateral enhancing solid renal masses suggestive of multifocal renal cell carcinoma (RCC) [Table/Fig-1a–b]. A chest CT disclosed multiple random pulmonary cysts and small nodules in both lungs compatible with lymphangioleiomyomatosis (LAM) and multiple micronodular pneumatosis hyperplasia [Table/Fig-1c]. Overall findings were consistent with tuberous sclerosis (TS). The patient underwent bilateral renal artery branches embolization [Table/Fig-1d,e] with resolution of symptoms. Patient had another two admissions with same symptoms and signs, during which she underwent repeat embolizations for renal artery aneurysms. Patient was lost to follow up before initiation of any further therapy.
Axial (a) and coronal (b) views of contrast-enhanced CT scan of abdomen showing bilateral enlarged kidneys with multiple fat-containing lesions suggestive of angiomyolipomas (white arrows) and multiple enhancing solid renal lesions suspicious of multifocal renal cell carcinoma (black arrows).
Axial view of CT scan of chest without contrast (c) showing multiple random pulmonary cysts in both lungs (white arrows) and bilateral innumerable scattered pulmonary nodules (black arrows), suggestive of lymphangioleiomyomatosis and multiple micronodular pneumatosis hyperplasia
Selective left renal arteriogram (d,e). After interrogation of multiple artery branches, an aneurysm was identified in the central aspect of interpolar region. A microcatheter was used to selectively, distally catheterize the supplying branch. Following microcoil embolization, good angiographic results were noted with no visualization of the aneurysm on the final left renal angiogram
TS should be suspected when common manifestations are found, including renal AML (55-75%) and LAM (26-39%) [1]. AML is one of the leading causes of death in TS patients. Patients are at risk of serious complications such as life-threatening hemorrhage (25%–50%). As the disease progresses, end-stage renal disease leading to dialysis develops secondary to encroachment of AML on normal renal parenchyma [2].
Historically, treatment of TS has focused on watchful waiting and surgical procedures to reduce tumor burden. Embolization is preferred in the setting of recent or active hemorrhage, or when large or multiple aneurysms are present. At the molecular level, loss of the TS complex 1 (TSC1) or TSC2 gene has been associated with increased production of vascular endothelial growth factor (VEGF), and inhibitors of mTOR have been shown to have an inhibitory effect on production of VEGF, tumor growth, and angiogenesis, both in vitro and in vivo. Everolimus is such an mTOR inhibitor approved for the treatment of adults with renal AML and TSC not requiring immediate surgery, based on favorable results from multicenter, international, randomized, double-blind, placebo-controlled trials EXIST-1 and EXIST-2 [2].
In 2–5% of patients with TS, RCC may develop within dysplastic epithelial cysts. Intriguingly, the course of RCC in TS differs from that in the general population. The mean age of TS-associated RCC is 25 years lower than in those without TSC mutations. In addition, TS-related RCC is usually bilateral and is more often found in women. However, RCC may be over-diagnosed in this patient population given the difficulty in differentiating from fat-poor AML with imaging studies alone. Immunostaining is helpful in such cases, with human melanoma black 45 (HMB-45) stain being characteristic for TSC-associated AML and lymphangioleiomyomatosis (LAM), while cytokeratin immunopositivity is typical for RCC [3].
LAM is characterized by cystic destruction of the lung caused by infiltration of smooth muscle cells and affects predominantly women, occurring more rarely in patients without TS (sporadic LAM). Symptomatic relief of air flow obstruction with bronchodilators and oxygen support can be used, as effective treatment options for this condition are lacking [2]. However, clinical evidence suggests that mTOR targeting can benefit other TSC-associated disease manifestations, including pulmonary LAM, thus rendering it a potential systemic treatment option for this genetic multifaceted disorder [4].
[1]. Umeoka S, Koyama T, Miki Y, Akai M, Tsutsui K, Togashi K, Pictorial review of tuberous sclerosis in various organsRadiographics 2008 e32:28 [Google Scholar]
[2]. Franz DN, Everolimus in the treatment of subependymal giant cell astrocytomas, angiomyolipomas, and pulmonary and skin lesions associated with tuberous sclerosis complexBiologics 2013 7:211-21. [Google Scholar]
[3]. Borkowska J, Schwartz RA, Kotulska K, Jozwiak S, Tuberous sclerosis complex: tumors and tumorigenesisInt J Dermatol 2011 50:13-20. [Google Scholar]
[4]. Moavero R, Coniglio A, Garaci F, Curatolo P, Is mTOR inhibition a systemic treatment for tuberous sclerosis?Ital J Pediatr 2013 39:57 [Google Scholar]