Introduction
In some cases of the completely edentulous patients, implant supported prosthesis treatment is almost impossible without complex techniques such as nerve transposition and grafting in the posterior maxilla and mandible. A solution for such situations is the All-on-4® concept. This method advocates tilting distal implants in edentulous arches which enables us in the placement of longer implants, improved prosthetic support with shorter cantilever arm, improved inter implant distance and improved anchorage in the bone [Table/Fig-1]. The “All-on-4® “treatment concept was developed by Paulo Malo with straight and angled multi-unit abutments, to provide edentulous patients with an immediately loaded full arch restoration with only four implants.
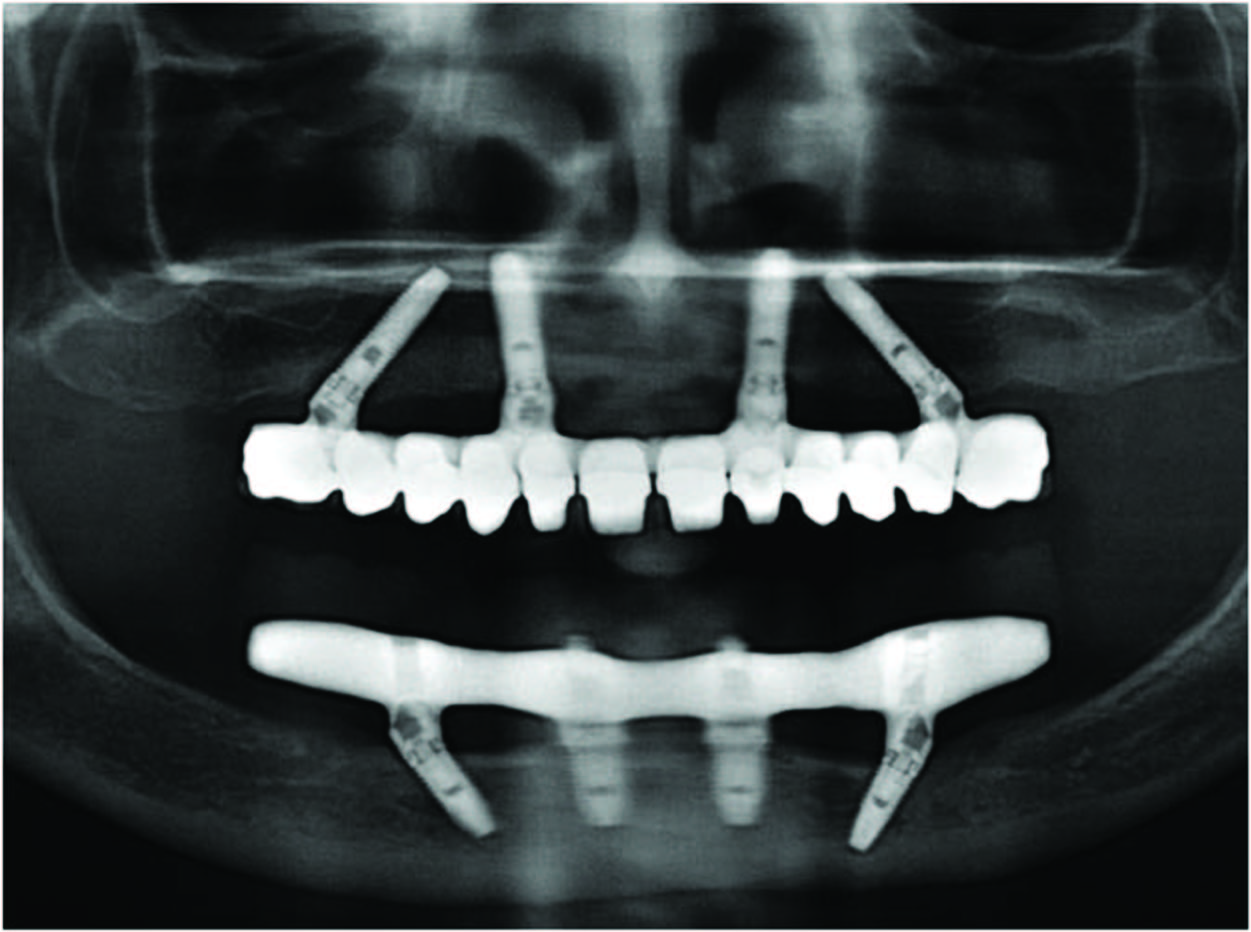
–Two placed vertically in the anterior region and two placed upto an angle of 45o in the posterior region.
When used in the mandible, tilting of posterior implants makes it possible to achieve good bone anchorage without interfering with mental foramina in severely resorbed maxillae, tilted implants are an alternative to sinus floor augmentation [1].
General considerations
To achieve primary implant stability (35 to 45 Ncm insertion torque).
Indicated with a minimum bone width of 5mm and minimum bone height of 10mm from canine to canine in maxilla and 8mm in mandible.
If angulation is 30o or more, the tilted implants can be splinted.
For tilted posterior implants, the distal screw access holes should be located at the occlusal face of the first molar, the second premolar, or the first premolar [2].
| Step 1 | Selection Of Case Satisfying The Inclusion Criteria |
| Step 2 | Planning Implant Placement Using All-On-4® Guide(Prefered) |
| Step 3 | Location Of Maxillary Antrum And Mental Foramen With All-On-4® Guide |
| Step 4 | Implant Placement Done Following The Protocols |
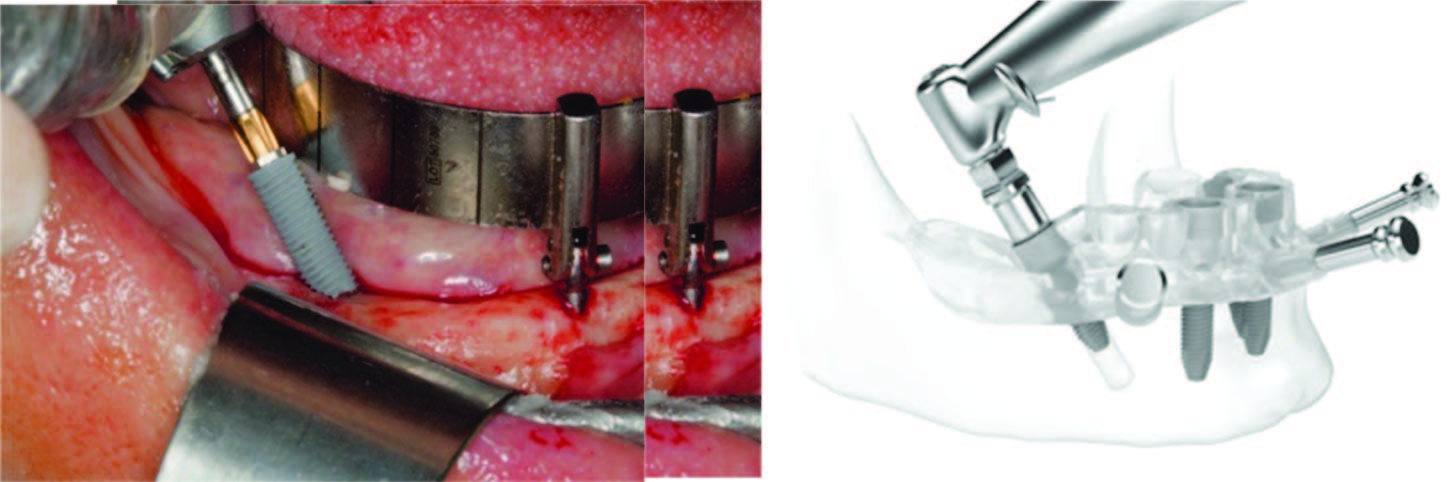
Implants in the maxilla are placed with two distal implants in the posterior region which are tilted anterior to the maxillary antrum while in the mandible implants are positioned anterior to the mental foramen. They should be inserted at an angulation of 30o-45o. The use of the All-on-4® surgical guide assists in ensuring the placement of the implants with correct positioning, angulation and emergence. The guide is placed into a 2mm osteotomy that is made in the midline position of the maxilla or mandible and the titanium band is contoured to follow the arc of the opposing arch. The guide also assists in retracting the tongue in mandibular cases. The vertical lines on the guide are used as a reference for drilling at the correct angulation, which should not be greater than 45o. The other guides that can be used for implant placement are Template, Angulated pins and Denture [Table/Fig-3a,b].
Guides for implant placement., a-guide., b-Template
Straight, 17o multiunit abutments and 30o angulated abutments with different collar heights are placed onto the implants. These are used to achieve the correct access allowing relative parallelism and so that the rigid prosthesis can be seated passively.
Success rate in edentulous maxillae
A retrospective clinical study including 242 patients with 968 immediately loaded implants supporting fixed complete arch maxillary all-acrylic prosthesis demonstrated a high survival rate 93% at patient level and 98% at implant level after 5 y of follow up . Recent studies encouraged the use of All-on-4® concept emphasizing that when planning a fixed rehabilitation in an edentulous maxillae using four implants, the quality of bone, the length of implants, the patient’s habits and the length of expected cantilever should be considered [3].
Comparison of tilted v/s non tilted implants
If an implant is part of a multi implant supported prosthesis, the spread of implants and stiffness of the prosthesis will reduce bending of the implant [4]. The more distal position of the posterior implant and the resulting shorter cantilever may have a role in reduction of stress values in the implant [5]. Strain gauge measurements performed by Krekmanov showed no significant differences in forces and bending moments between titled and non tilted implants [6]. Theoretical models show that an increased prosthetic base, due to the inclination of implants can reduce the force acting over the implants. Therefore, from biological point of view, the position of the neck of the implant can be more important than the inclination of the implants themselves. Bevilacqua et al., demonstrated that tilting of the distal implant by 30o in a FFP decreased the level of stress by 52% and 47.6% in compact bone and cancellous bone respectively, when compared to vertical implants supporting FFP with longer cantilevers [7].
Loading of the cantilever on prosthesis can cause a hinging effect that induces considerable stresses on the implants closest to the load application [8]. When the distal cantilevers of FFP are excessive in length, deformation of the framework can result in fracture of the prosthetic screw, the acrylic resin teeth or even the framework itself [9].
The splinted tilted implants showed lower stresses than the axial implant with cantilever and the reduction of the stresses generated with the prosthesis might help reduce maintenance problems of FFPs v/s those that employ a conventional implant configuration [10]. When a vertical load was applied to the first premolar of the tilted implant, the two neighboring implants mostly shared the load, as the prosthesis was loaded between the mesial and distal implants load was distributed to both supporting implants through the prosthesis, the tilted implant configuration did not show over loading or bending [11].
Stress patterns on implants in prosthesis supported by four or six implants
A long term study found no significant differences in implant survival in a comparison of complete maxillary prosthesis supported by four or six implants. The stress location and distribution patterns were very similar in both four and six implant models. The cantilever should be minimized as its presence greatly increases stress on the distal implant, regardless of whether or not the prosthesis is supported by four or six implants [12].
Stress patterns around distal angled implants in the All-on-4® concept configuration
A study analysed the photo elastic strain patterns surrounding distal implants placed at 0o, 15o, 30o and 45o. There was no remarkable difference in strain magnitude between models of implants placed at 0, 15, 30. But increase in strain pattern for 45o angled implants [13].
Angled Abutments
In general, the magnitude of stress and strain for angled abutments was within or slightly above the physiologic limits. The use of angled abutments on two tilted implants placed in a curved arch and with cross-arch splinting might help decrease the stresses around the distal implants [13].
Loading on the healing bone
Overloading and fracturing happen more readily in healing bone than in normal bone [14]. Occlusal loading in the period immediately after placement may be sufficient to cause micro damage in the bone surrounding the implant, even though the same load will not do so after healing and adaptation of the bone to the implant. The All-on-4® concept advocates immediate loading. A slight load on healing bone shortens healing time rather than prolonging [15]. Immediately loaded implants osseointegrate provided that forces and implant micromotion are controlled.
Immediate extraction socket placement
The connection of implants may provide a safer transfer of load on each implant and so the placement in healed or fresh extraction bone sights may not influence implant survival when rehabilitating totally edentulous mandibles [16].
From a surgical perspective, the most notable are careful implant site preparation (including tapping), use of relatively low – torque producing implants, the preparation of an osseous shelf to level the alveolar ridge and establish optimum implant sites and the provision of adequate interocclusal space.
From a prosthetic perspective, the high success rate obtained with this protocol, including minimal bone loss even with multiple extractions and bone reduction followed by immediate function is believed to be as a result of –
Stable splinting of all four implants with the provisional immediately after surgery,
Careful occulsal adjustment to provide bilateral occulsion in the canine and first premolar areas,
Avoid occlusal contact toward the distal of the prosthesis and maximizing the anteroposterior spread [17].
An Anteroposterior spread that minimizes the distal cantilevers and establishes well distributed four-point stability was probably contributary to both implant and prosthetic success. The immediate implant loading and function in the dental extraction setting can be performed with a high degree of confidence.
| Rangert | 10 mm for a cantilever of 20 mm (2xA-P-spread)for mandibular ISFPs |
| English | ISFPs should be 1.5 times A-P-spread for mandible maxillary ISFP posterior cantilever should be reduced to 6-8mm due low bone density |
Rangert provides simple guidelines for controlling occlusal loads on implants and prosthetic reconstruction- an A-P-spread(distribution distance between the most anterior and most posterior implants) of 10 mm was proposed for a cantilever of 20 mm (2xA-P-spread)for mandibular ISFPs English proposed Anecdotally that a very reasonable rule of thumb for determining posterior cantilever in mandibular ISFPs should be 1.5 times A-P-spread. According to English, this would allow a 10-12 mm posterior cantilever for the mandible, whereas maxillary ISFP posterior cantilever should be reduced to 6-8mm due low bone density [18].
Open tray multi-unit impression copings are placed onto the multi-unit abutments, which are then splinted with a low shrinkage autopolymerising resin (GC pattern resin) and wire bars [Table/Fig-5,6a]. This ensures an accurate transfer without accidental displacement of the impression copings. An open tray impression is made with a rigid polyvinyl siloxane material (3M ESPE Imprint Putty) to capture the positions of the implants and the soft tissues.
| Step 1 | Open tray impression made with wire and GC resin splinting for improved accuracy |
| Step 2 | Final impressions after integration is verified, being splinted with GC resin and metal. |
| Step 3 | All ceramic Zirconia bridge being designed with CAD/CAM technology |
| Step 4 | Use of CAD/CAM zirconia bridge or Titanium framework milled for crown cementation |
| Step 5 | Crowns luted to zirconia framework |
| Step 6 | Implant-supported zirconia bridge framework with individual crowns luted |
Prosthetic phase a resin splinting., b-final prosthesis

Provisional all-acrylic resin prosthesis is then constructed and issued to the patient within a few hours or overnight. The provisional prosthesis is torqued to 15Ncm. The patient is reviewed after one week, at three weeks, three months and then annually.
At the three month appointment, fabrication of the definitive bridge may be started. The final restorative solution can be a:
CAD/CAM designed fixed prosthesis with Zirconia or Titanium framework. Individual crowns are cemented to the final bridge framework.
Fixed prosthesis with CAD/CAM designed Titanium or Zirconia framework with acrylic veneering [Table/Fig-6b].
Fixed prosthesis with cast metal and veneering porcelain.
Removable final prosthesis: e.g. milled bar overdenture, MK1 attachment overdenture.
Comparision of superstructure framework
The first patient with fixed complete dentures were provided with Cr-Co alloy frameworks with resin teeth. This protocol was modified over time and gold alloy casting was introduced to provide a more stable occlusion in metal and to allow porcelain veneering of the framework, however in case like severe bone resorption, large amt of gold alloy had to be cast. To avoid problems with casting few non casting approaches such as premachined gold-alloy cylinders /bars and laser – welded titanium frameworks were introduced. More recently a new protocol based on using computer numeric-controlled milling of a solid block of titanium was developed and is free of the technical challenges involved in previous approaches [19].
Occlusal aspect
Many implant failures can be attributed to improper occlusal design which can concentrate stresses in the bone and lead to rapid bone resorption. The goal of any prosthetic procedure must include the establishment of a functional occlusion [20].
Occlusal Schemes
Occlusal scheme of implant-prosthetic superstructure basic requirements are
Establishment of stable jaw relationships with maximum intercuspal contacts that are bilaterally identical
Establishment of “ freedom in centric” within the overall occlusal scheme
Elimination of any interference between the maximum intercuspal and retruded contact positions
Provision of harmonic, free mandibular movements with light tooth contacts during both lateral and protrusive maneuvers.
Occlusal scheme for immediate loading for All-on-Four concept
Avoid or minimize length of cantilever .Simultaneous bilateral point contacts on all teeth, excluding teeth distal to implant emergence. In lateral movements, group function or guidance with flat linear pathways and minimal vertical super impositon excluding teeth in cantilever. In protrusive movements, guidance distributed on all anterior teeth including canines, with flat linear pathways and minimal verical super imposition. Even if the implant supported prosthesis is opposed to a removable full denture, in excursive movements avoid balancing contacts.
Occlusal scheme for All-on-Four definitive prosthesis [
Table/Fig-7]
Simultaneous bilateral point contacts on canine and posterior teeth and grazing contacts on incisors
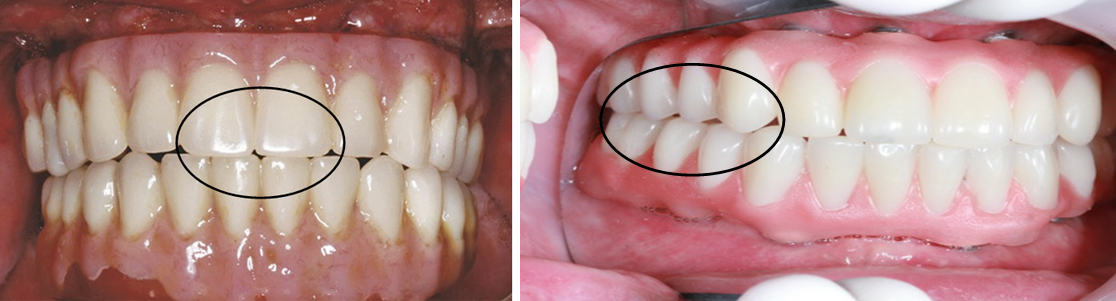
Simultaneous bilateral point contacts on canine and posterior teeth and grazing contacts on incisors. In lateral movements, canine guidance opposing natural dentition, group function opposing posterior implant supported bridge with flat linear pathways and minimum vertical super imposition [Table/Fig-7a,b]. If the implant supported prosthesis is opposed to removal, complete denture or implant supported over denture or a distal extension cast partial denture leave the most distal tooth slightly out of occlusion and in excursive movements seek one or more balancing contacts, planning greater anteroposterior space at the anterior teeth. The occlusal pattern should have relatively flat cusps i.e. the inclination of the cuspal planes should be less than the inclinations of the condylar path.
Complete denture opposing All-on-4® concept
Over denture opposing All-on-4® concept
Precision attachment opposing All-on-4® concept
Cast partial denture opposing All-on-4® concept
Distal tooth out of occlusion
Balancing contacts
planning greater anteroposterior space at the anterior teeth
Since the teeth of the distal cantilever are less heavily loaded, the guiding surfaces of the incisors and canines can be expected to undergo increasing abrasions with time, therefore eliminate premature or non working side contacts on the distal cantilever [21].
Discussion
Advantages of the All-on-4® concept
Angled posterior implants avoid anatomical structures
Angled posterior implants allow longer implants anchored in better quality bone
Reduces posterior cantilever
Eliminates bone grafts in the endentulous maxilla and mandible in majority of cases
High success rates
Implants well-spaced, good biomechanics, easier to clean
Immediate function and aesthetics
Final restoration can be fixed or removable
Reduced cost due to less number of implants and avoidance of grafting in the majority of cases.
Limitations
Good general health and acceptable oral hygiene;
Sufficient bone for 4 implants of at least 10mm in length; and
Implants attain sufficient stability for immediate function.
Disadvantages
Free hand arbitrary surgical placement of implant is not always possible as implant placement is completely prosthetically driven.
Length of cantilever in the prosthesis cannot be extended beyond the limit.
It is very technique sensitive and requires elaborate pre-surgical preparation such as CAD/CAM, surgical splint.
Length of cantilever in the prosthesis cannot be extended beyond the limit.
Conclusion
Various researches done on the concept and practice of the rehabilitation has advanced the All-on-4® treatment option from the skeptical to the predictable with commendable success rates. The long term results of this technique and the numerous advantages of immediate loading, the reduced morbidity, the high patient satisfaction and relatively low costs should be taken into account when a decision among the alternative treatment options for an edentulous jaw has to be made.
[1]. Christopher , Implant rehabilitation in the edentulous jaw: The “All-on-4® concept” immediate functionAustralian dental practice 2012 :138-48. [Google Scholar]
[2]. Singh Pankaj P, A Norman CraninAtlas of oral implantology:275-81. [Google Scholar]
[3]. Paulo Malo, All-on-4® immediate function concept for completely edentulous maxillae. A clinical report on the medium and long term 5 years outcomeJournal of Oral ImplantologyXXXVII/No. Four/2011 [Google Scholar]
[4]. Dallenback K, Biomechanics of in-line vs offset implants supporting a partial prosthesisJ Dent Res 1996 75:183 [Google Scholar]
[5]. Bellini Chiara M, Comparison of tilted versus non-tilted Implant –supported prosthetic designs for the restoration of the edentulous mandible. A biomechanical studyInt J oral Maxillofacial implants 2009 24:511-12. [Google Scholar]
[6]. Krekmanov L, Tilting of posterior mandibular and maxillary implants of prosthesis supportInt J Oral maxillofacial implants 2000 15:405-14. [Google Scholar]
[7]. Bevilacqua H, Three dimensional finite element analysis of load transmission using different implant inclinations and cantilever lengthsInt J Prosthodont 2008 21:539-42. [Google Scholar]
[8]. White SN, Effect of cantilever length on stress transfer by implant – supported prosthesisJ Prosthet Dent 1994 7:493-99. [Google Scholar]
[9]. Captuto AA, Biomechanics in clinical dentistryChicago Quintessance 1195 :64 [Google Scholar]
[10]. Kim KS, Kum YL, Bae JM, Chohw Biomechanical comparison of axial and tilted implants for mandibular full arch fixed prosthesisInt J Oral Maxillofacial Implants 2011 26:976-84. [Google Scholar]
[11]. Duyck J, Van Oostcrwyck H, Vander Sloten J, Magnitude and distribution of occlusal forces on oral implants supporting fixed prosthesis – An in vivo studyClin Oral implants Res 2000 111:465-75. [Google Scholar]
[12]. Guilherme Carvalho Silva, Stress patterns on implants in prostheses supported by four or six implants. A three dimensional finite element analysisInt J Oral Maxillofac Implants 2010 25:239-46. [Google Scholar]
[13]. Tasneem Begg, Stress patterns around distal angled implants in the All-on-4® concept configurationInt J Oral Maxillofacial implants 2009 24:663-71. [Google Scholar]
[14]. Frost HM, Perspectives: Bone’s mechanical usage windowsBone miner 1992 9:257-71. [Google Scholar]
[15]. Isodro F, Influence of forces on peri, implant boneClin Oral Implants Res 2006 17:8-18. [Google Scholar]
[16]. Tommaso Grandi, Immediate Loading of four All-on-4® Post-extractive implants supporting mandibular cross arch fixed prosthesis – 18 month follow up from a multi centre prospective cohortEur J Oral Implantol 2012 5(3):277-85. [Google Scholar]
[17]. Daniel F Galindo, Immediately loaded Mandibular fixed implant prosthesis using the All-on-4® protocol. A report of 183 consecutively treated patients with 1 year of function in definitive prosthesisInt J Oral Maxillofac Implants 2012 27:628-33. [Google Scholar]
[18]. Bo Rangert, All-on-4® Immediate-Function Concept with Brånemark System Implants for Completely Edentulous Maxillae: A 1-Year Retrospective Clinical StudyClinical Implant Dentistry and Related Research 2005 7(1):S88-94. [Google Scholar]
[19]. Khatami Amir H, “All-on-4®” Immediate function concept and clinical report of treatment of an edentulous mandible with a fixed complete denture and milled titanium frameworkJournal of Prosthodontics 2008 17:47-51. [Google Scholar]
[20]. Schemes of occlusion – Color atlas of dental medicineImplantology:299-304. [Google Scholar]
[21]. Immediate loading – A new era in oral implantology – chap – 14 –pg 234.Occlusion in implant supported prosthesis under immediate loading and delayed loading [Google Scholar]