Ethylenediaminetetraacetic Acid (EDTA) – Dependent Pseudothrombocytopenia: A Case Report
Izhar Shabnam1, Chuphal D S2, Joshi B C3
1Chief of Lab, Dr Lal path Labs, Haldwani, Nainital, India.
2Senior Technician, Department of Hematology, Dr Lal path Labs, Haldwani, Nainital, India.
3Lab Supervisor, Dr Lal path Labs, Haldwani, Nainital, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shabnam Izhar, Akashpuram Colony, Lalabegum, Jagatpur, Bareilly, UP, India. Phone : 91-9410658003,
E-mail: drshabnamizhar@gmail.com
Pseudo-thrombocytopenia, Peripheral blood smear, Thrombocytopenia
We present a case of 26-year-old female patient who was presented as a case of Isolated Thrombocytopenia and found to have EDTA induced Pseudo-Thrombocytopenia with no associated pathologies.
Pseudo-thrombocytopenia (PTP) is defined by falsely low platelet counts on automated analysers and is caused by in vitro phenomena including large platelet aggregates in blood samples. Platelet aggregates on account of their large size are frequently not included in the platelet window of auto-analysers, but are counted as leukocytes, leading to misleadingly low platelet counts and high leukocyte counts [1]. The phenomenon can be suspected on examining the platelet histogram and review of the smear should confirm the presence of aggregates.
Ethylenediaminetetraacetic acid (EDTA) is a well-known anticoagulant since early 1950s and it has certain advantages over other anticoagulants [2]. It inhibits clotting by removing or chelating calcium from the blood. EDTA most important advantage is that it does not distort blood cells, making it ideal for the most hematological tests. It is known to cause erroneous results of platelet counts by automated hematological analysers yielding low platelets counts. This relatively rare phenomenon has been found in the normal population as well as being associated with some disease entities. It occurs with an incidence of approximately 0.1% of the normal population [3]. it has never been reported to be associated with bleeding tendency or dysfunction of platelets. Far from being a harmless curiosity, undiagnosed PTP is a pitfall leading to unwarranted investigations, platelet transfusions, and treatment with glucocorticoids and may lead to surgical procedures being cancelled.
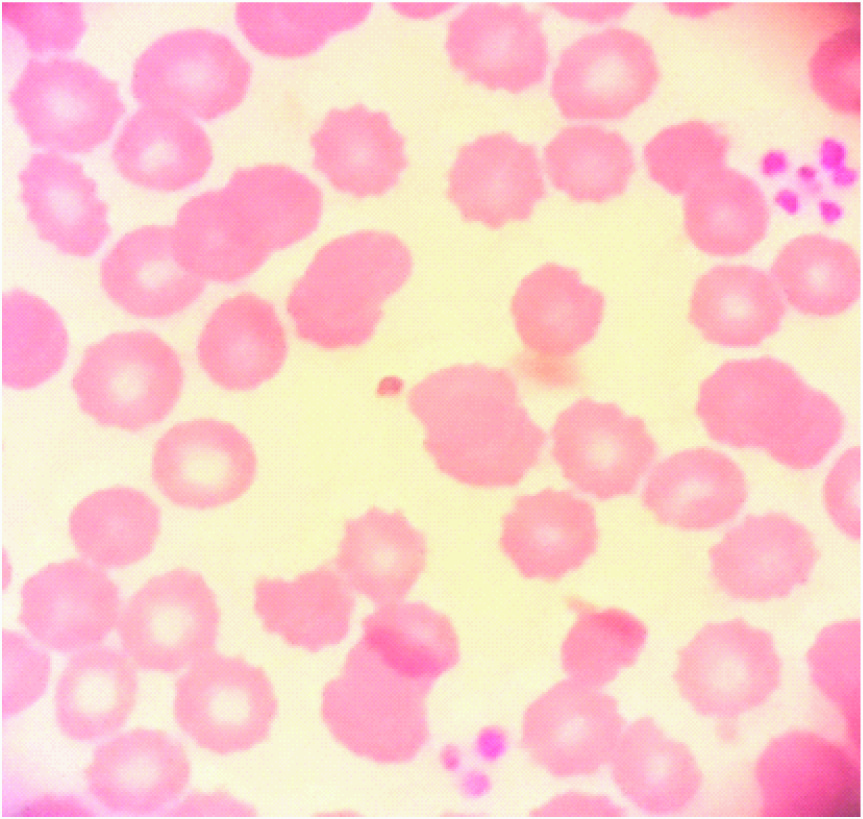
A 26-year-old female patient was referred to our lab for investigations as a case of newly diagnosed thrombocytopenia. She presented to a local physician with fever and Upper Respiratory Tract Infection (URTI). The CBC revealed normal parameters apart from a low platelet count; 10 x10^9/L. A blood film [Table/Fig-1] was ordered and it revealed platelet aggregations. History, physical and systemic examination was unremarkable. Other laboratory investigations were normal as well as brain CT scan and abdominal ultrasound. The lab asked for CBC to be drawn in a citrate tube as well as a Heparin tube to diagnose if this could be an EDTA induced platelet clumping. The CBC and the blood film results were the same in both tubes and similar to the EDTA tube results except that the count was higher with the Heparin tube; 72x10^9/L.
EDTA induced PTP was first reported by Gowland et al., (1969). It is attributed to EDTA induced alteration of surface glycoproteins (GP) and anionic phospholipids, which enables binding of antiplatelet antibodies, which in turn cause agglutination. Antibodies against the platelet GPIIb/IIIa have been reported in this context [4]. Platelet agglutinins generally belong to the immunoglobulin M class. However, immunoglobulin G and immunoglobulin A are also described. Around 20% of cases with EDTA induced PTP show the phenomenon in citrate anticoagulant as well [5]. Oxalate and heparin have also been implicated in PTP. Normal platelet function seems to be a criterion for platelet aggregation. Some resources state that clumping of platelets in patients with EDTA- induced Pseudo-Thrombocytopenia can be prevented by the use of other anticoagulants such as Sodium Citrate or Heparin. Other resources have found that even these agents can induce platelet clumping as well. This is comparable to the results in our case.
We drew blood of the pateint in three tubes containing three different types of anticoagulants; EDTA, Sodium Citrate and Heparin. The three blood samples were run in fully automated Hematology analyser. The platelet count with the EDTA tube was 11.0 x10^9/L, with the Sodium Citrate tube was 22.0 x10^9/L and with the Heparin tube was 72 x10^9/L. The peripheral blood morphology of the three blood samples revealed platelets aggregations.
A prospective study of 20,761 routine clinical blood specimens was conducted to evaluate the incidence and causes of thrombocytopenia [6]. It revealed that the incidence was 0.15% and 72% of which had EDTA induced platelet clumping, 28% had spuriously low platelet counts due to large platelets. Another study states that when Theophylline was used as an anticoagulant in blood samples showing aggregation with EDTA, blood film examination revealed no platelet clumping [6]. Kamath et al., [1] reported resolution of Pseudothrombocytopenia using 37°C incubation and Kanamycin.
Unrecognized Pseudo-Thrombocytopenia may result in unnecessary laboratory testing and unwarranted interventions. Examination of a well prepared peripheral blood smear is mandatory for every case of thrombocytopenia to rule out platelet clumping (Pseudo-Thrombocytopenia). For a definitive diagnosis of EDTA Induced Thrombocytopenia, the simultaneous collection of blood into EDTA citrate and Heparin containing or other anticoagulant containing tubes may provide a simple, rapid mean of identifying the presence of EDTA- Induced Pseudo-Thrombocytopenia.
Blood film revealing platelet aggregations
[1]. V Kamath, P Sarda, MP Chacko, U Sitaram, Pseudothrombocytopenia observed with ethylene diamine tetra acetate and citrate anticoagulants, resolved using 37°C incubation and Kanamycin. Indian J Pathol Microbiol 2013 56:306-08. [Google Scholar]
[2]. HG Gordan, NL Larson, Use of sequestrene as an anticoagulantAm J Clin Pathol 1955 23:613-18. [Google Scholar]
[3]. S Rod, DO Hangerman, Ethylenediaminetetraacetic acid dependent Peudo- Thrombocytopenia: A case report of an incidental but important findingMedicine on-line 2000 12:120-23. [Google Scholar]
[4]. NJ Wilkes, NA Smith, SV Mallett, Anticoagulant-induced pseudothrombocytopenia in a patient presenting for coronary artery bypass graftingBr J Anaesth 2000 84:640-42. [Google Scholar]
[5]. N Bizzaro, HO Heymann, EDTA-dependent pseudothrombocytopenia: A clinical and epidemiological study of 112 cases, with 10-year follow-upAm J Hematol 1995 50:103-09. [Google Scholar]
[6]. O Ohnuma, Y Shirata, K Miyazawa, Use of theophylline in the investigation of Pseudo-Thrombocytopenia induced by EDTAJ Clin Pathol 1988 41(8):915-17. [Google Scholar]