Assistance of Pressure Conformer for Reconstruction of Lower Fornix
Pokpong Amornvit1, Reiyal Goveas2, Dinesh Rokaya3, Sahana Bajracharya4
1 Instructor, Maxillofacial Prosthetic Clinic, Department of Prosthodontics, Faculty of Dentistry, Mahidol University, Bangkok, Thailand.
2 Resident, Maxillofacial Prosthetic Clinic, Department of Prosthodontics, Faculty of Dentistry, Mahidol University, Bangkok, Thailand.
3 Resident, Maxillofacial Prosthetic Clinic, Department of Prosthodontics, Faculty of Dentistry, Mahidol University, Bangkok, Thailand.
4 Resident, Maxillofacial Prosthetic Clinic, Department of Prosthodontics, Faculty of Dentistry, Mahidol University, Bangkok, Thailand.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Pokpong Amornvit, Maxillofacial Prosthetic Service, Faculty of Dentistry, Mahidol University, 6 Yothi Street, Bangkok 10400, Thailand.
Phone: +66-891616260,
E-mail: pokpong_am@yahoo.com
Absence of fornix in anopthalmic socket can result in difficulty in prosthetic and cosmetic rehabilitation. A 30-year-old female was presented with absence of the lower fornix in anopthalmic socket. A stock conformer was used to create continuous downward pressure with the help of an acrylic rod, gauze and a medical adhesive tape. Eventually, a lower fornix was created and finally rehabilitated with ocular prosthesis.
Ocular prosthesis, Pressure Conformer, Shallow fornix
Case Report
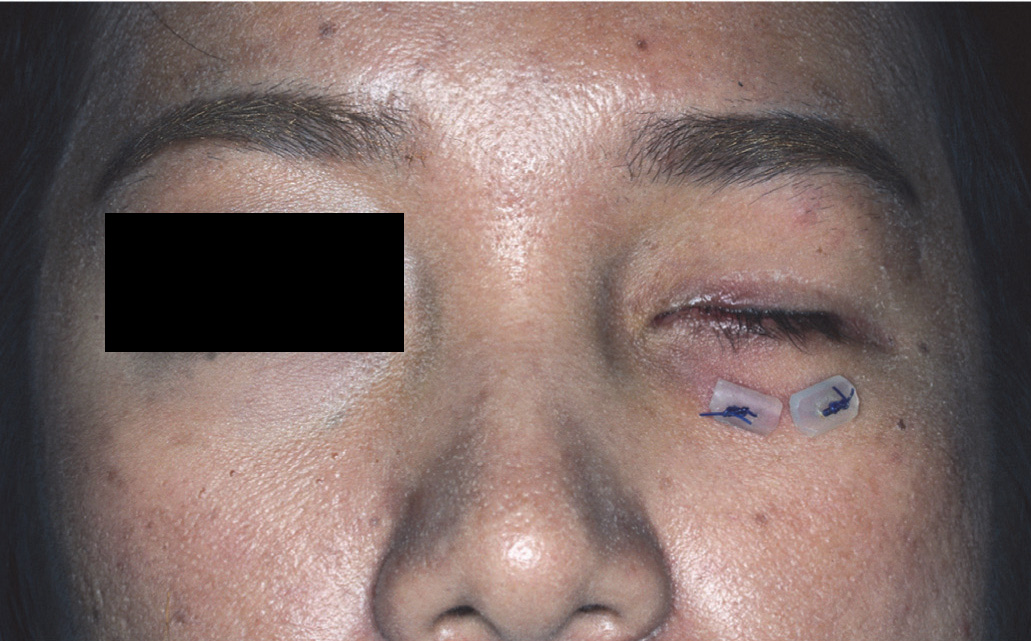
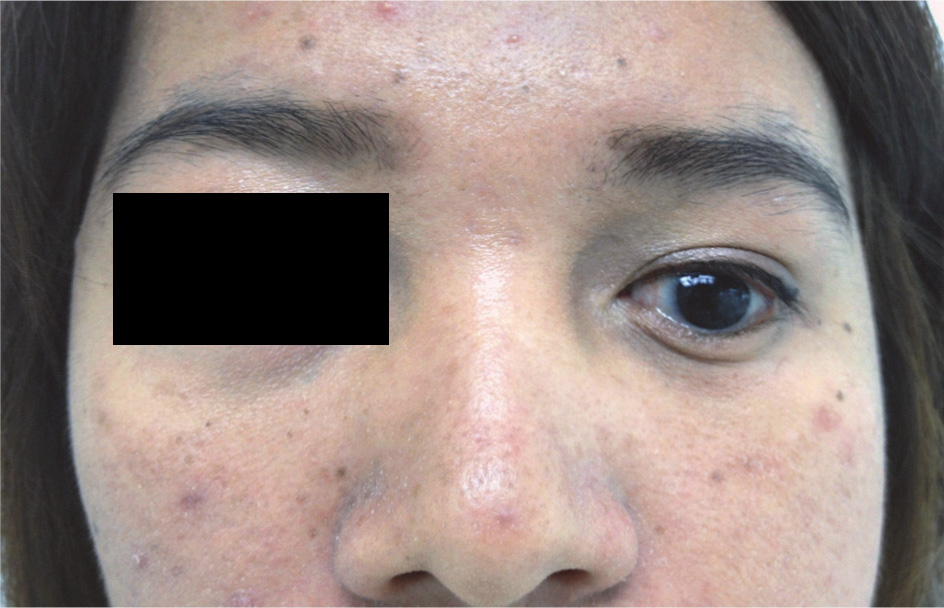
A 30-year-old female was referred to Maxillofacial Prosthetics Service for the prosthetic rehabilitation of left ocular defect. Past medical history revealed, she had congenital defect of left eye and and enucleation was performed with the placement of an intraorbital implant 2 weeks back [Table/Fig-1]. The examination of the ocular defect showed the presence of micropthalmus, facial hypoplasia and eyebrow shifted downward, upper eyelid ptosis, superior and inferior eyelid laxity, normal lacrimal secretion, adequate superior fornix depth but shallow inferior fornix depth with adequate socket volume for the prosthesis fabrication [Table/Fig-1]. She did lower fornix fixation twice but still the depth was not adequate.
Frontal view of the patient with left eye defect with sutures on lower eyelid
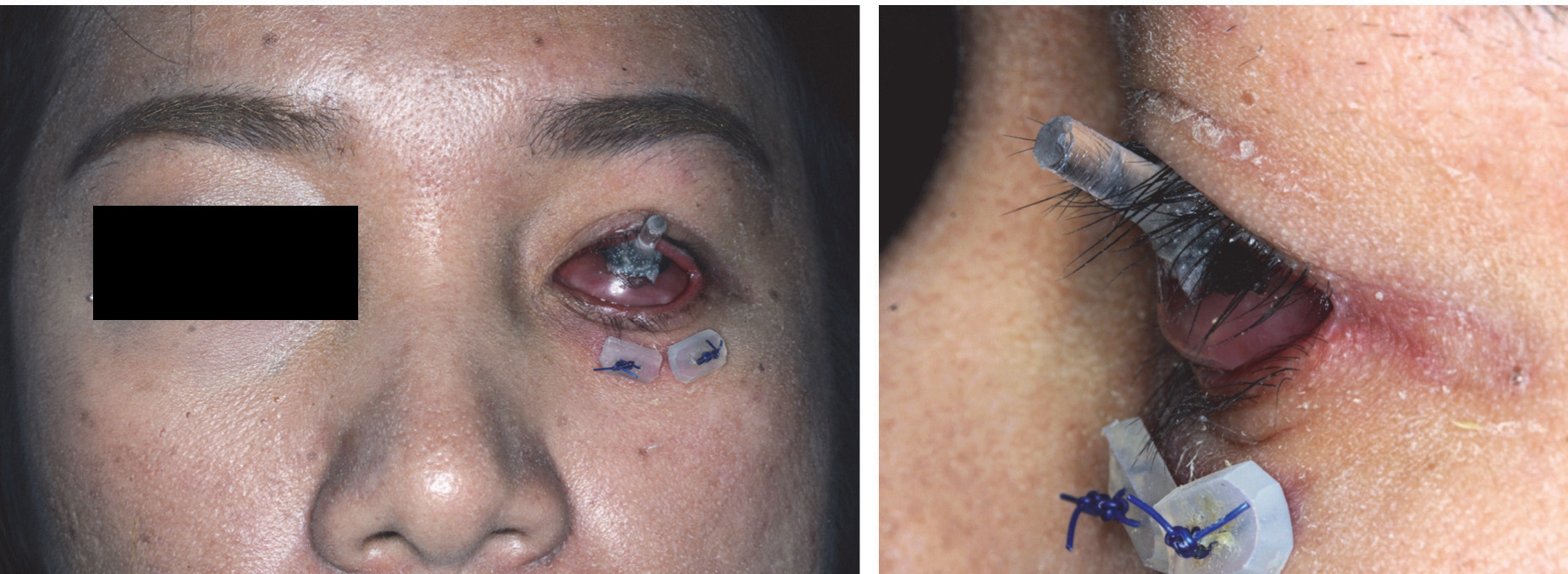
Then, a little oversized stock conformer was tried in the patient. But the conformer was pushed upward due to shallow inferior fornix [Table/Fig-2]. The mobility of the tissues and depressibility of the inferior fornix was checked with a small brush with the application of the mild pressure into the fornix. It revealed that the fornix depth could be deepned from continuous mildpressure [Table/Fig-3]. So, the treatment plan consisted of deepening the fornix with the help of the conformer and fabrication of the ocular prosthesis.
When a stock conformer was tried in, it was pushed upward ward due to the shallow inferior fornix

Examination done to check the depression of the inferior fornix with the application of the pressure with a small brush

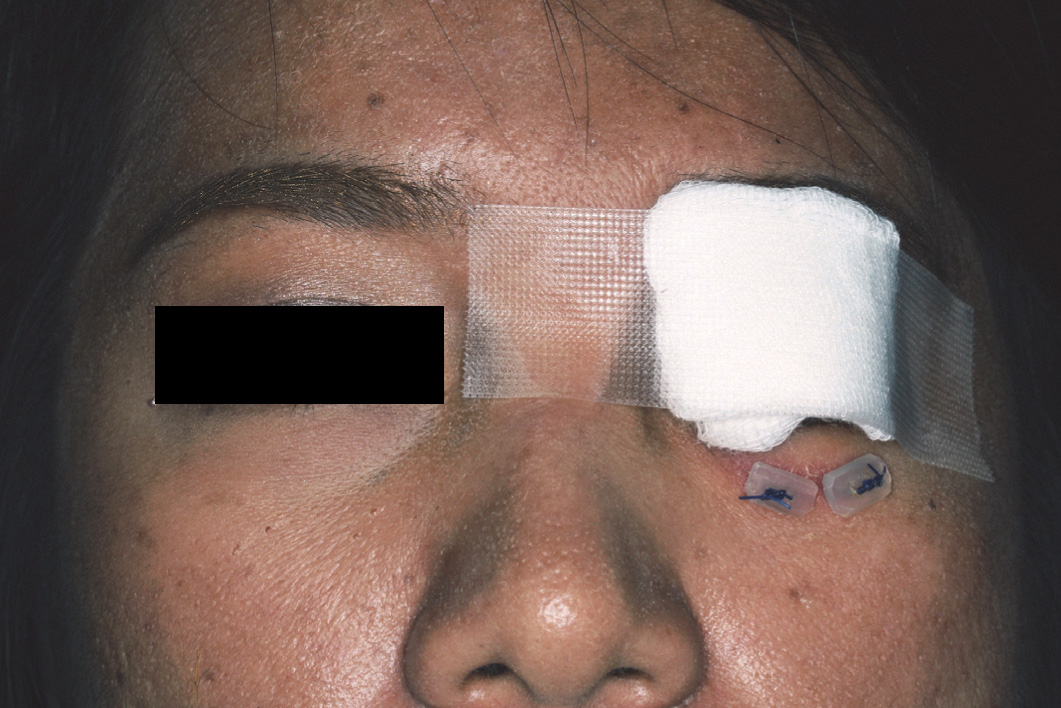
An acrylic rod (10mm length × 3mm diameter) was attached at the center of the stock conformer with autopolymerizing resin. The acrylic rod was directed superiorly when the conformer was inserted [Table/Fig-4]. Then, mild downward pressure was applied to the acrylic rod so that it is directed straight and that the inferior border of the conformer creates pressure on the lower fornix to deepen the lower fornix depth. The rod was kept in this position with the help of the gauze [Table/Fig-5].The patient felt pressure on inferior fornix but no pain. The conformer was placed in this position with the help of a medical adhesive tape [Table/Fig-6]. The patient was instructed to use the conformer with rod for 6 weeks in this position and instructed to remove and maintain hygiene every 4-5 days. The fornix depth of 3 mm was restored after 6 weeks (1-2 mm per month). The patient was advised to use the conformer to to compress the lower fornix at night only for 3-4 months after delivery [Table/Fig-7].
The rod was directed superiorly when the conformer was inserted in frontal and lateral view

(a) Application of mild downward pressure applied on the acrylic rod so that the inferior border of the conformer creates mild continuous pressure on the lower fornix to deepen the lower fornix depth (b) The rod was kept in position with the help of the gauze
Patient instructed to use the conformer with rod in this position for 2 weeks and to maintain hygiene every 4-5 days by removing the conformer
Lower fornix depth was restored (3 mm) after two weeks use of the conformer

Then, an ocular prosthesis was fabricated in this patient [Table/Fig-8]. The outcome was satisfactory after creatinglower fornix.At 3 months recall visit, the outcome of the ocular prosthesiswas satisfactory [Table/Fig-9].
Ocular prosthesis fabricated in the patient. The outcome was satisfactory after the fornix deepening in frontal and lateral view
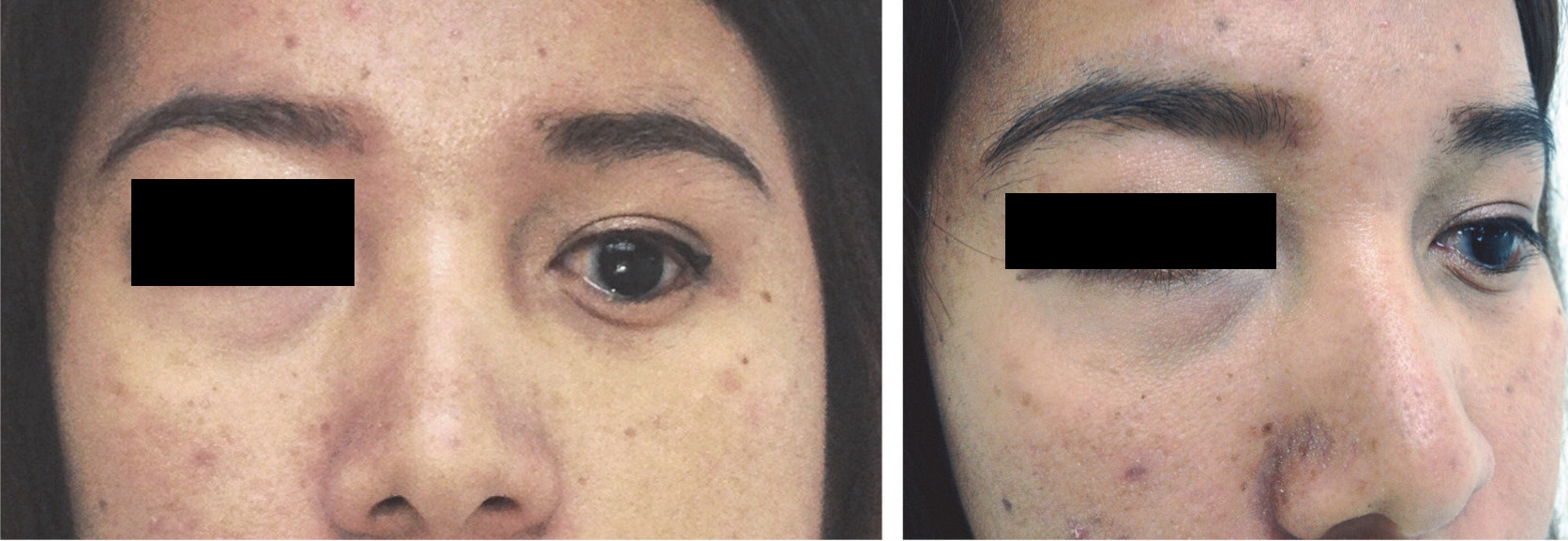
Ocular prosthesis at three months recall visit
Discussion
Ocular defects arising from an ablative surgery following trauma or tumor usually leave the patient disfigured. The most common surgeries performed are evisceration and enucleation. In evisceration, the ocular contents are removed leaving behind the sclera and muscle attachments. Enucleation surgery is more invasive with removal of the entire globe, but leaves behind the eye socket and eyelids [1]. Sometime following enucleation, shallow lower fornix is caused, apart from the congenital cause. An adequate sized surgical stent or conformer helps to maintain the socket depth. So the surgeon should use surgical stent to prevent formation of shallow fornix following enucleation. A shallow lower fornix makes prosthetic rehabilitation of the case extremely difficult and usually with poor esthetic results [2]. There are several management tools, both prosthetically and surgically, in the management of the shallow fornix in the anpthalmic sockets. Surgical correction of the shallow fornix can be performed and there are various techniques described by authors for this procedure [3–6]. Mucous membrane grafts may be attempted; nonetheless, there is an increased risk of recurrent graft failure if vascularity is decreased [2]. However, in certain cases there might be a relapse of the shallow fornix and multiple surgeries might result scar contracture [5,6]. In such cases a pressure conformer can be used. Pressure conformers are originally used to conform the ocular tissue beds following surgical reconstruction [7]. They are the most effective way to re-establish contracted sockets following infection or poorly fitting prosthesis. Taneda and Sakai highlighted the use of ready-made ocular prosthesis as the ocular conformer with a free skin graft to create fornix in contracted socket and the result was satisfactory [8]. For the prosthetic correction of the shallow fornix, the candidate should have sound socket for prosthetic correction. The muscle can be evaluated to see the possibility of tissue compression and the balance of muscle tone of lower upper eyelid. To overcome the upward force from the extraocular muscle, compression of the muscle downward is indicated using conformer which creates a continuous force to expand the socket. The depth that able to increase around 2-3 mm. Fornix depth of 3 mm is enough to maintain the prosthesis in socket.
In this case, we considered correcting the fornix depth prosthetically, as the surgery was done previously and further surgeries might lead to scar contractures [5,6]. So a stock conformer attached with acrylic rod, gauze and medical adhesive tape to deepen the lower fornix [Table/Fig-5,6]. This technique is a simple and economical. This technique created continuous pressure to deepen the lower fornix. In this case, 3 mm lower fornix was gained in six weeks and the final outcome after prosthetic rehabilitation was satisfactory [Table/Fig-8,9].
There are several other methods of application of pressure for the socket to create the fornix. Molgat et al., has mentioned a technique to create fornix using custom made conformers and fixing them in socket using sutures [9]. So once an adequate sized conformer was chosen, itis lined with the buccal mucous membrane and two superior and inferior fornix-deepening sutures of 4-0 braided polyester are passed through the lids and tied over bolsters to securely fix the conformer in position for 6-12 weeks. If fornix is not adequate, a new custom conformer may be designed for that particular socket to help maintain the fornices. Another technique for postoperative management of the fornix depth is given by Scott [10]. This utilizes a capillary traction device and the Lafuente pressure mask. The device allows proactive management of the socket by utilizing the pressure at night. This method also allows the pressure to be applied on active contraction in the socket.
Conclusion
Absence of lower fornix creates difficulty in ocular fabrication. A stock conformer can be used to create lower fornix with acrylic rod, gauze and medical adhesive tape. This technique is a simple and economical. After lower fornix fixation, prosthetic rehabilitation of ocular defect can be done with an ocular prosthesis without difficulty.
[1]. Nakra Comparing Outcomes of Enucleation and EviscerationOphthalmology 2006 113:2270-75. [Google Scholar]
[2]. Collin JRO, Enucleation, evisceration and socket surgeryIn: A manual of systematic eyelid surgery 2006 3rd edLondonElsevier-Butterworth-Heinemann:223-28. [Google Scholar]
[3]. Sterker I, Frerich B, Secondary reconstruction of the eye socket with a free radial forearm flapOphthalmologe 2007 104:978-82. [Google Scholar]
[4]. Vagefi MR, McMullan TF, Burroughs JR, Autologous dermis graft at the time of evisceration or enucleationBr J Ophthalmol 2007 91:1528-31. [Google Scholar]
[5]. Bajaj MS, Pushker N, Singh KK, Evaluation of amniotic membrane grafting in the reconstruction of contracted socketOphthal Plast Reconstr Surg 2006 22:116-20. [Google Scholar]
[6]. Kumar S, Sugandhi P, Arora R, Pandey PK, Amniotic membrane transplanta- tion versus mucous membrane grafting in anophthalmic contracted socketOrbit 2006 25:195-203. [Google Scholar]
[7]. Raizada K, Shome D, Honavar SG, Management of an irradiated anophthalmic socket following dermis-fat graft rejection: a case reportIndian J Ophthalmol 2008 56:147-48. [Google Scholar]
[8]. Taneda H, Sakai S, Effective Use of a Ready-made Ocular Prosthesis for Contracted Anophthalmic Socket Reconstruction SurgeryAnaplastology 2013 2(2):1-2. [Google Scholar]
[9]. Molgat YM, Hurwitz JJ, Webb MCF, Buccal mucous membrane-fat graft in the management of the contracted socketOphthalmic Plast Reconstr Surg 1993 9(4):267-72. [Google Scholar]
[10]. Scott R, A unique suction deviceThe Journal of the American Society of Ocularists 1986 17:11-14. [Google Scholar]