The correct identification of living or deceased persons using the morphology of hard and soft tissues of oral cavity is an important element in forensic odontolgy. Investigators often gain information and evidence through the use of odontology, anthropometry, fingerprints and lip prints. DNA profiling is the most accurate method of forensic identification but fingerprints and lip prints can also be used as an additional tool. The groove patterns present on the human lips are unique to each individual and analogous to finger prints. The study of these grooves or furrows present on the red part of lips is known as cheiloscopy [1]. Lip prints are similar to finger prints, palm prints and footprints where individual characteristics of grooves and furrows are used for identification. Lip prints are unique and do not change during the life of a person [2]. It has been verified that they recover after undergoing alterations like trauma, inflammation and diseases like herpes and that the disposition and form of the furrows does not vary with environmental factors [3–5].
Cheiloscopy studies conducted in Tamil Nadu, Maharashtra and Kerala population of India have shown that there is a predominance of different lip print patterns in different populations [2,6,7]. Variations of the lip patterns in different populations will help in forensic odontology. Previous studies have shown the relationship of finger print patterns and the predominance of different lip print patterns in different ABO blood groups [8–10].
Studies also reveal that lip prints show differences according to the race and ethnic origin of a person [11]. In this light, the present study was designed to determine and compare the predominant lip print pattern in Kerala and Maharashtra population, correlate them in ABO blood groups.
Materials and Methods
The present study was conducted at School of Dental Sciences, Karad, India. The study subjects were selected from Krishna Institute of Nursing Sciences, Karad, India. During the period of the study there were 270 students present. By purposive sampling technique, we enrolled all the students in our study. Subjects birth by origin of Kerala and Maharashtra were only included in the study. Subjects with any inflammation, trauma, congenital deformity or any other disease of the lips and with any known hypersensitivity to the lipstick were excluded from the study. After considering the inclusion and exclusion criteria, 100 subjects from Maharashtra (69 females and 31 males) and 100 from Kerala (100 females) were selected for the study. The research protocol was initially submitted to the institutional ethical committee and review board of Krishna Institute of Medical Sciences Deemed University (KIMSDU). The ethical clearance was obtained from KIMSDU before commencing the study. The study was conducted during the period from December 2013 to February 2014.
All the participants were briefed about the purpose of the study and their lip prints were recorded with their due consent. The materials used in the study were non glossy lipstick of a dark color (Lakme enrich, Hindustan Lever Ltd., India), scissors, white bond paper, transparent cellophane tape and magnifying lens.
The data was collected by utilizing pre tested structured questionnaire that included demographic, hematological parameters and lip print patterns. The data was collected by personal interview and examination techniques by the investigator. The observer bias was minimized by cross-examination by an expert senior researcher. The blood group of subjects was identified by qualitative test with anti sera using the slide method.
Lip print recording procedure: Subject’s lips were cleaned with sterile gauze before application of lipstick. The subject was asked to open the mouth and lipstick was applied in a single motion on both the lips. The subjects were asked to gently rub his/her lips together to spread the lipstick evenly on the both lips. A square strip of white bond paper (10cm×10cm) was folded and kept between the lips, the subject was asked to close his/her lips for few seconds. The subjects were asked to slowly open the mouth and the bond paper was removed carefully. A cellophane tape was stuck over the lip print marking obtained on the white bond paper to avoid distortion. The lip prints were studied carefully using a magnifying glass in bright light to identify and classify. The middle part of the lower lip was considered for classification, as this fragment is usually visible in any trace and most frequently found at the crime scene. The classification scheme proposed by Tsuchihashi [3] was used to analyze the lip prints [Table/Fig-1, 2].
Tsuchihashi classification of lip print patterns

Different lip print patterns observed in the present study
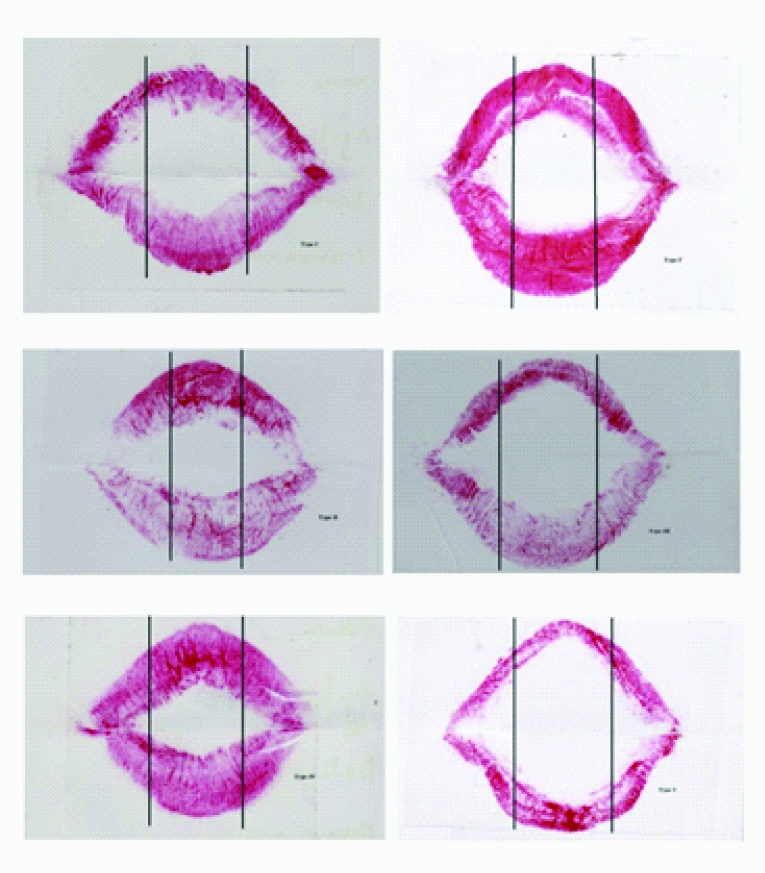
Type I: Clear-cut vertical grooves that run across the entire lips
Type I’: Similar to type 1, but do not cover the entire lip
Type II: Branched grooves
Type III: Intersected grooves
Type IV: Reticular grooves
Type V: Grooves do not fall into any of the above categories and cannot be differentiated morphologically (undetermined).
Statistical Analysis
The raw data was entered in MS Excel and analyzed into descriptive statistics. Chi-square test was applied to see the significant differences in lip print patterns and demographic parameters and p-value less than 0.05 was considered significant. Statistical calculations were performed using Statistical Package for the Social Sciences (SPSS) software version 19 (Armonk, New York: IBM. Corporation).
Results
The analysis of lip print patterns revealed that no two lip prints matched with each other, thus establishing the uniqueness of the lip prints in each individual. The most common lip print pattern observed in our study group was Type IV (32.5%) followed by Type II (28.5%), Type III (17.5%), Type I (7.5%), Type V and Type I’ (7% both).
Distribution of lip print patterns in gender [Table/Fig-3]: The most predominant lip print pattern in males was Type II followed Type IV, Type III, Type I and Type V. The most predominant pattern in females was type IV, followed type II, type III, type I’, type V and type I.
Distribution of lip print patterns in gender
| Lip Print Patterns | Male | Female | Total |
|---|
| Type I | 4 | 11 | 15 |
| Type II | 11 | 46 | 57 |
| Type III | 7 | 28 | 35 |
| Type IV | 8 | 57 | 65 |
| Type V | 1 | 13 | 14 |
| Type I’ | 0 | 14 | 14 |
| Total | 31 | 169 | 200 |
Distribution of lip print patterns in populations [Table/Fig-4]: The most predominant lip print pattern in Kerala population was Type IV (53%) followed by Type III (19%), Type II (15%), Type V (6%), Type I (4%) and Type I’ (3%). The most predominant lip print pattern in Maharashtra population was Type II (42%) followed by Type III (16%), Type IV (12%), Type I (11%), Type I’ (11%) and Type V (8%). Comparison of lip print pattern between Kerala and Maharashtra population showed statistical significance difference (Chi-square value, X2 = 47.032, p<0.001).
Distribution of lip print patterns in populations
| Lip Print Patterns | Population | Total Frequency (%) |
|---|
| Kerala Frequency (%) | Maharashtra Frequency (%) |
|---|
| Type I | 4 (4%) | 11 (11%) | 15 (7.5%) |
| Type II | 15 (15%) | 42 (42%) | 57 (28.5%) |
| Type III | 19 (19%) | 16 (16%) | 35 (17.5%) |
| Type IV | 53 (53%) | 12 (12%) | 65 (32.5%) |
| Type V | 6 (6%) | 8 (8%) | 14 (7%) |
| Type I’ | 3 (3%) | 11 (11%) | 14 (7%) |
| Total | 100 (100%) | 100 (100%) | 200 (100%) |
†X2 = 47.03, p<0.001
†X2 = p-value is significant at 95% confidence interval.
Distribution of lip print patterns in females of two populations [Table/Fig-5]: The most predominant lip print pattern in Kerala females was type IV and Maharashtra females was type II.
Distribution of lip print patterns in females of two populations
| Lip Print Patterns | Kerala females Frequency (%) | Maharashtra females Frequency (%) |
|---|
| Type I | 4 (4%) | 7 (10.1%) |
| Type II | 15 (15%) | 31 (44.9%) |
| Type III | 19 (19%) | 9 (13%) |
| Type IV | 53 (53%) | 4 (5.7%) |
| Type V | 6 (6%) | 7 (10.1%) |
| Type I’ | 3 (3%) | 11 (15.9%) |
| Total | 100 | 69 |
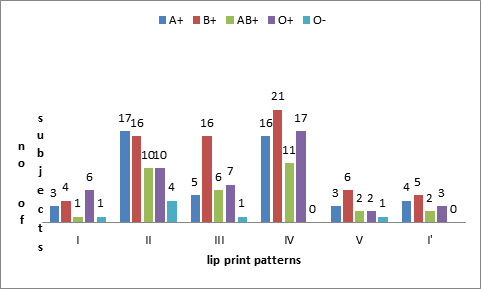
Correlation of lip print patterns in ABO blood groups [Table/Fig-6]: Type II lip print pattern was predominant in A+ blood group followed by type IV, type III, type I’, type I and type V. Type IV lip print pattern was predominant in B+, AB+ and O+ blood groups, followed by type II and type III. Type II lip print pattern was predominant in O- blood group followed by type I and type III. The lip print patterns does not show any correlation between ABO blood groups. Blood groups A-, B- and AB- were not taken into correlation, as there were no subjects with these blood groups in our study.
Distribution lip print patterns in different ABO blood groups
† Not even single subject with A-, B- and AB- blood groups
Discussion
Lip prints have been used for identification of a person since 19th century, Fischer was the first to describe it in 1902 [12]. The use of lip prints in personal identification and criminal investigation was first recommended in France by Locard [13]. In 1950, Synder also suggested the idea of using lip prints for identification of an individual [14]. Lip prints can be found on surfaces such as glass, paper, clothing, cutlery or cigarette butts. Even the invisible lip prints can be used and can be lifted using aluminium and magnetic powder [15,16]. The edges of the lips have sebaceous glands with sweat glands in between therefore, secretions of oil and moisture enable development of ‘latent’ or persistent lip prints, analogous to finger prints [17]. Lip prints found at criminal investigation site can help in identifying the individual and solving the cases.
Sivapathasundharam et al., stated that the lip pattern recording depended on the way the lip muscles are relaxed to produce a particular pattern [2]. Lip print pattern recorded depends on whether the mouth is open or close. In closed mouth position, the lip exhibits well-defined grooves, where as in the open position the grooves are relatively ill defined and difficult to interpret [6]. In the present study the lip prints were recorded in closed lip position.
Different opinions exist between different studies, as the authors have divided the lips in to quadrants and considered different quadrants of lips for the study. We have considered middle third of the lower lip for the classification, since it is the part most frequently found at the crime scene.
The most predominant pattern in our study group was Type IV (32.5%) which is in accordance with Verghese AJ et al., [7] study, followed by type II (28.5%),Type III (17.5%), type I (7.5%) and type V (7%) and contradictory to Suzuki and Tsuchihashi study conducted in Japanese individuals [3]. They found type III to be the most common, followed in order by type I, type II, type IV and type V. Studies on Indian subjects have also yielded varying results, Vahanwala and Parekh [18] in their study in Mumbai found that Type I was the most frequent and Sivapathasundharam et al., study in Indo-Dravidian population noted that Type III was predominant [2]. The differences in the results of our study may be because of different genetic and ethnic background of the study population.
In our study the most predominant lip print pattern seen in Kerala population was Type IV (53%), which was in accordance with Verghese AJ study [7] conducted in Kerala population, followed by type III (19%),type II (15%), type V(6%), type I and I’ (4%). Whereas lip print patterns in Maharashtra population showed type II (42%) predominance followed by type III(16%), type IV (12%), type I, I’ (11%) and type V (7%) which was contradictory to results of Gondivkar et al., [6] and Augustine J studies [19], as they studied lip pattern in different quadrants of the lip.
The most common lip print pattern among males in our study was type II which was in accordance with Verma P et al., study [10] and contradictory to Gondivkar et al., study [6]. Bias here is that these male population are from maharashtra only. The most common lip print pattern in Kerala females was type IV which was in accordance with Verghese AJ study [7] conducted in Kerala population. Maharashtra females showed type II pattern predominance which was in accordance with Gondivkar et al., study [6] conducted in Maharashtra population.
The lip print pattern correlated with blood groups showed type II predominance in A+ and O- blood groups, which was in accordance with Patel S et al., study [9]. Blood groups B+, O+ and AB + had type IV predominance. The correlation of blood groups with the lip print patterns was not statistically significant which was similar to Patel S and Verma P et al., studies [9,10]. The results also matched with previous studies conducted by Telagi et al., in south India and Sandhu et al., in Punjabi population [20, 21].
Conclusion
Cheiloscopy is a simple and less expensive technique, which can be used as an additional tool in forensic investigations. In our study different population showed different lip print pattern predominance, with no correlation in ABO blood groups. Chelioscopy has to be carried out in depth on larger samples and in different populations of the world. A database on different lip prints in different population has to be created, to be used as an effective tool. Along with forensic medicine specialist, role of dentist in forensic investigation is important since hard and soft tissues of oral and perioral structures helps to identify a person.
†X2 = 47.03, p<0.001
†X2 = p-value is significant at 95% confidence interval.