A Very Rare Presentation of Synovial Cell Sarcoma Arising from the Tendon Sheath of Flexor Hallucislongus Tendon and Causing Secondary Erosion of Calcaneum
C J Mani Kumar1, B.S.S.S. Venkateswarlu2
1 Assistant Professor, Department of Orthopaedics, Government General Hospital, Rangaraya Medical College, Kakinada, India.
2 Professor, Department of Orthopaedics, Government General Hospital, Rangaraya Medical College, Kakinada, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. C.J Mani Kumar, Assistant Professor, II unit, Department of Orthopaedics, GGH, RMC , Kakinada - 533001, India. Phone : 9848198594, E-mail : manikumarcj@gmail.com
Synovial cell sarcoma is a rare variety of soft tissue tumour. Very few cases of this tumour affecting the tendon sheath have been reported so far. We report a rare presentation of synovial cell sarcoma of the flexor hallucislongus tendon in a 35-year-old female. She presented with a painful lump (tumour) arising from postero medial aspect of the right ankle. The mass produced erosion of the overlying calcaneum over the time of one year. She was managed surgically by enucleation of the tumour followed by augmentation of calcaneum with bone cement.
Enucleation, Flexor hallucislongus, Spindle cell tumour
Case Report
A 35-year-old female from yanam (Pondicherry) presented to our OPD with the chief complaint of a painful lump over the inner aspect of her right ankle, which initially appeared for the first time about one year ago. The lesion since then gradually progressed in size before being finally excised by a general surgeon after six months from onset on the assumption of a diagnosis of nodular tenosynovitis. However the swelling recurred four months after surgery, and then she made her first visit to our OPD with the complaint of a painful lump over the inner aspect of right heel and ankle [Table/Fig-1a&b]. She was able to move around with much difficulty due to the presence of the mass. Walking uphill or climbing stairs was problematic. Clinical examination of the mass revealed a tender mass of soft tissue origin extending over the region posterior to the calcaneal bone. Excision biopsy of the tumour was planned based on the earlier histological report of nodular tenosynovitis with spindle cell predominance.
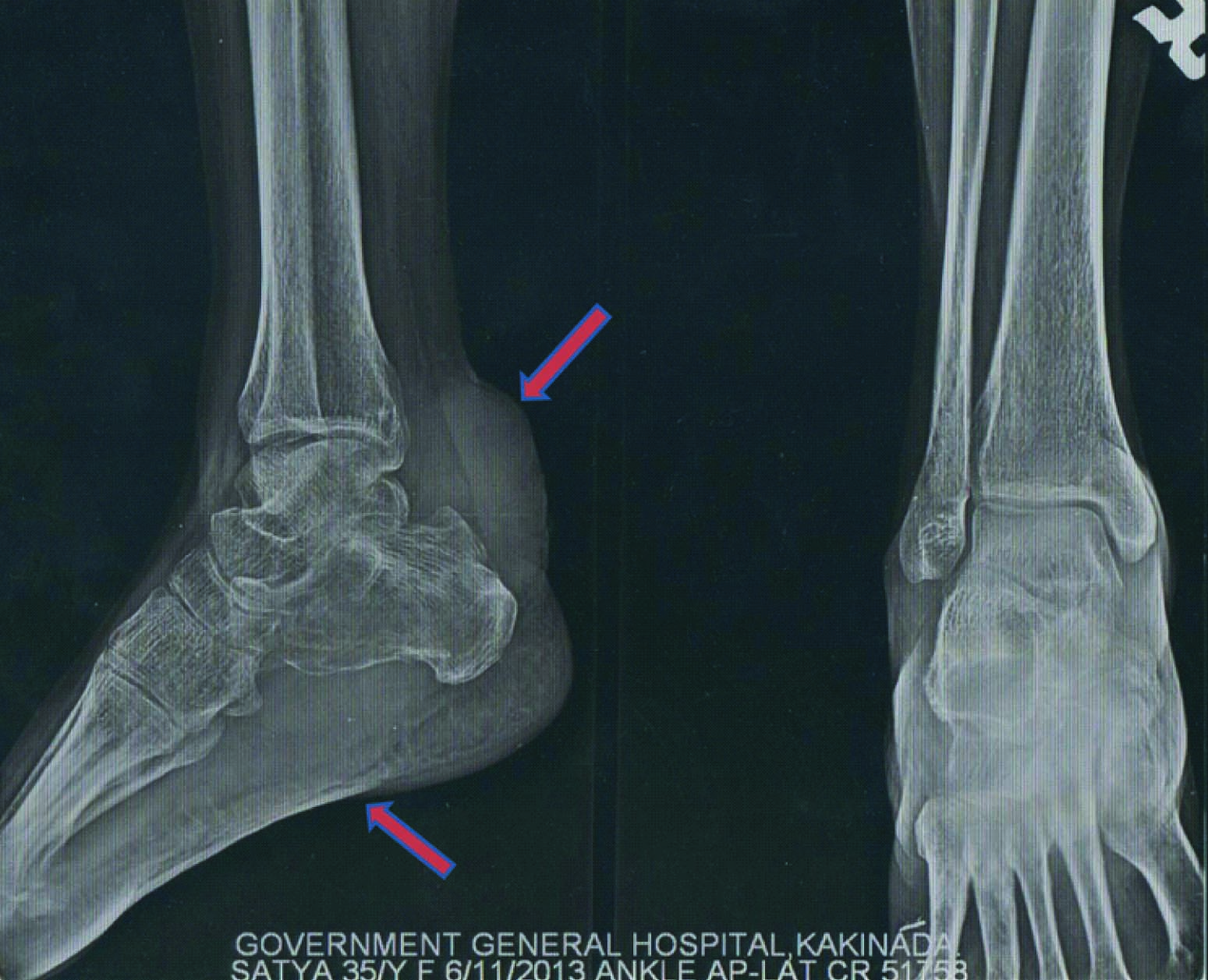
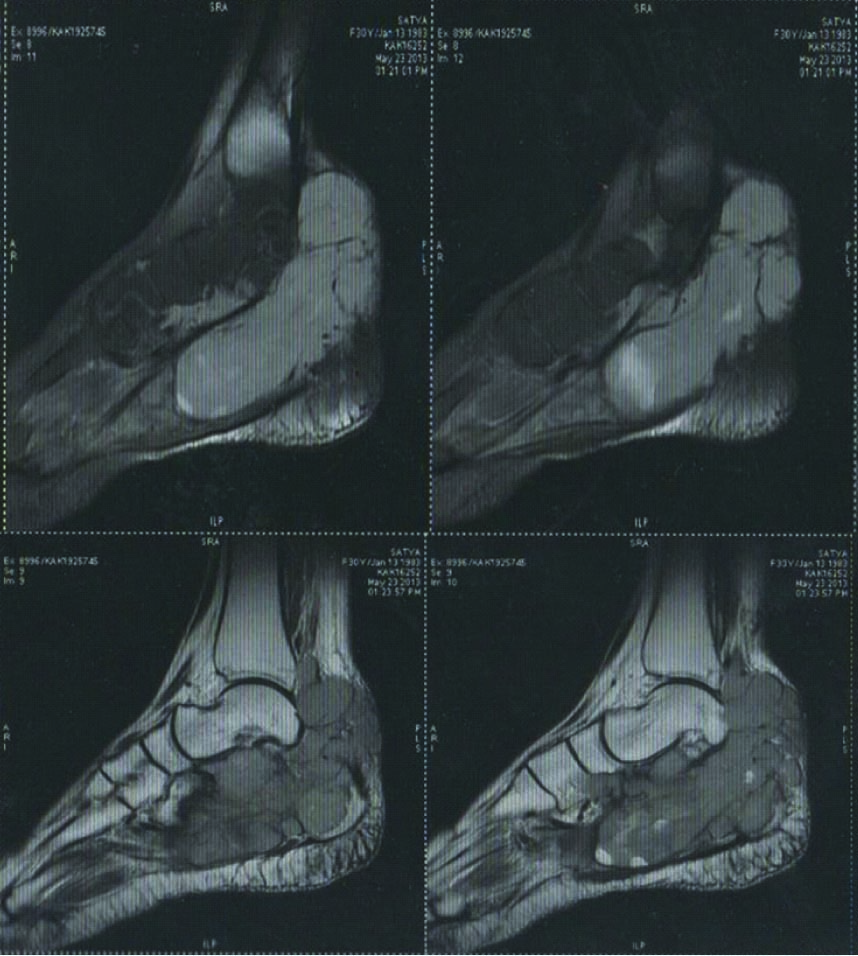
X-ray showed a soft tissue mass posterior to the calcaneum producing erosion of the bone [Table/Fig-2]. MR imaging of the right leg and foot recognized a soft tissue mass involving right flexor hallucislongus extending into the calcaneum [Table/Fig-3]. Routine blood investigations and all other laboratory parameters assessed were within the normal limits.
Pre operative clinical picture of the patient showing a lump around the inner aspect of the right ankle

Pre operative radiograph of the right ankle , antero posterior and lateral views showing the tumour mass causing erosion of calcaneum (indicated by red arrows)
MR images of the ankle and foot showing the extent of the tumour
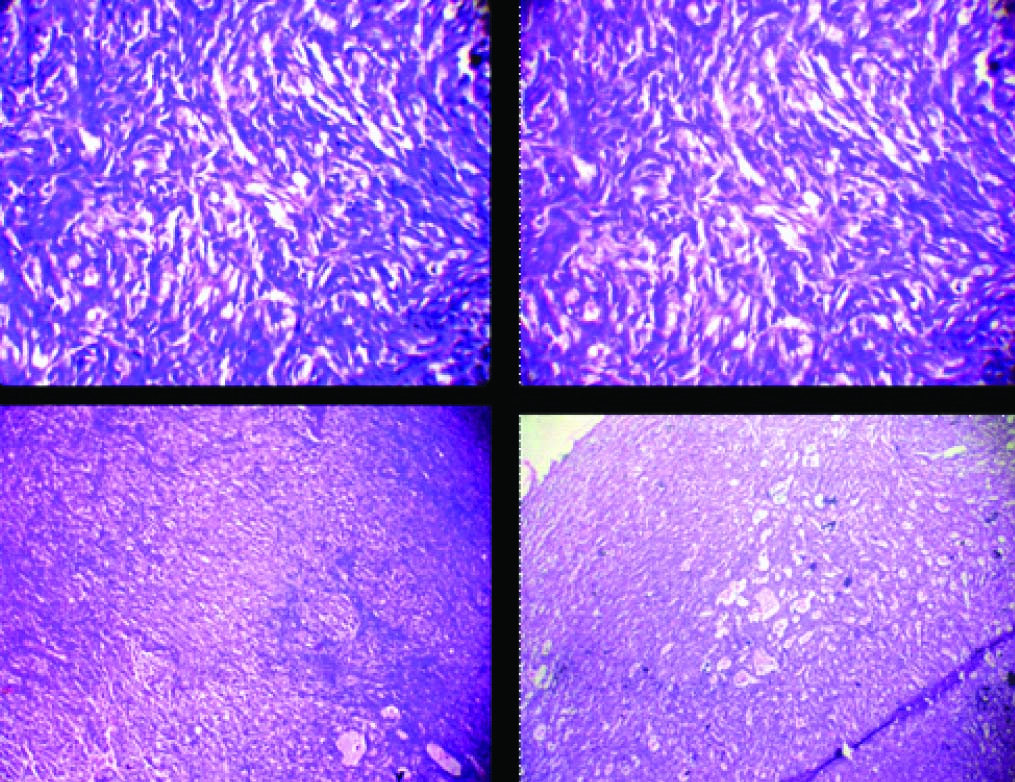
Excisonal biopsy, enucleation, curettage and bone cement augmentation of the right calcaneum was performed under spinal anaesthesia [Table/Fig-4]. The excised mass was sent for histopathological examination. Based on histopathological examination [Table/Fig-5] a diagnosis of spindle cell sarcoma (monophasic). Synovial sarcoma/ low grade fibrosarcoma was made and recommended for immunohistochemical and cytogenetic studies.
Intra Operative images demonstrating pre operative marking of the tumour margins and key steps in surgery

Histological photomicrograph showing cells sheets of spindle cells with oval elongated nuclei and few cells with vesicular nuclei (H & E stained slides examined under high and low resolution)
She was referred to a higher centre for assessment of tissue slides. Her tumour was staged as T2b N0 M0Gx. A final diagnosis of synovial cell sarcoma monophasic variant (spindle cells) with immunohistochemical study strongly positive for CK Ema Bcle2, vimentin and focally positive for s100 was made. Serial follow up of MRI was advised to the patient as resection yielded no residual primary tumour except for two plantaris nodules with no metastasis. At five months postoperative period patient was pain free and there were no signs of tumour recurrence locally [Table/Fig-6]. She is ambulant and is able to bear her weight completely. She is able to carry her daily activities without any hindrance.
Follow up clinical images taken at five months following surgery, showing well healed scar with no signs suggestive of local recurrence

Discussion
“I have not seen synovial cell sarcoma, but has it seen me?” words of late Francesca Thompson, M.D still hold true. She first expressed her view in a paper presentation made at AO foot and ankle society meeting. She reported seven cases [1] of synovial cell sarcoma in that conference.Synovial cell sarcoma is the fourth most common of soft tissue sarcomas. The term synovial cell sarcoma is a misnomer as it does not arise from synovial structure [2] (suggested by Miettinen and Virtanen). Distal extremities are more commonly associated with this tumour. It is seen to affect mostly tendon sheath, bursa and joint capsule.
The tumour can occur over a wide age range but usually is seen in adolescent and young adults of about 15 to 40 yrs age. Tumour has an indolent course and patients usually present late as the mass remains painless for years [3]. Usual duration for development of symptoms is around 2 to 4 yrs [4]. These tumours are commonly misdiagnosed and are wrongly interpreted and treated for arthritis, synovitis or bursitis. Knee is the most commonly affected large joint. There are few other reports of synovial sarcoma affecting the foot and ankle [5,6].
The Cleveland Clinic Foundation reported 34 synovial sarcomas of the extremities, and of these, five were in the foot and one was in the ankle. Four of these patients were treated with amputation, and one patient died of pulmonary metastases. Seale et al., in his retrospective study of seven patients with malignant soft tissue tumours of foot and ankle reported four synovial sarcomas [7].
Most of the publications on synovial sarcomas show that these tumours were commonly misdiagnosed as ganglia, plantar fasciitis, synovitis and fibroma. These tumours are generally regarded as benign tumours. Chou and Mala reported 33 patients with tumours of the foot and ankle treated at one institution over a 14 y period. X-rays sometimes show underlying bone reaction or multiple small radio opacities due to focal calcification [8]. MRI is the modality of choice in the evaluation of soft-tissue tumours of the foot and ankle [9], allowing examination of a mass in the axial, sagittal, and coronal planes. Although the image does not provide a histologic diagnosis, it shows features that allow differentiation between benign and malignant lesions.The treatment for synovial sarcoma is wide or radical excision with adjunctive radiation therapy and possibly chemotherapy. The most common form of this disease is the biphasic type, with epithelial cells and fibroblast-like spindle cells [10].
The prognosis for five year survival rate ranges from 36% to 76%, and the 10 y survival rate is less (20% to 63%), because of late metastases. Favourable prognostic factors include age of the patient (15 y or younger), less than 5 cm in size, distal extremity involvement, and low tumour stage.
Conclusion
Synovial cell sarcoma though a common soft tissue tumour of the foot is very rare to originate from the tendon sheath and even rare to invade regional bone. It has been described as a slow growing tumour with a benign nature. The immunohistochemical characteristics of synovial cell sarcoma typically present a strong positivity with S100 study.
[1]. Lahr DD, Harrelson JA, Synovial sarcoma of the foot and ankle: Presented atThe Annual American Orthopaedic Foot and Ankle Society Meeting 1995July Vail, CO [Google Scholar]
[2]. Miettinen M, Virtanen I, Synovial sarcoma - a misnomerAm J Pathol 1984 117:18-25. [Google Scholar]
[3]. Bos GD, Esther RJ, WolI TS, Foot tumors: diagnosis and treatmentJ Amer Acad Orthop Surg 2002 10:259-70. [Google Scholar]
[4]. Weiss SW, Goldblum JR, Malignant Soft Tissue Tumors of Uncertain Type. In Weiss SW, Goldblum JRSoft Tissue Tumors 2001 4th edSt. LouisMosby [Google Scholar]
[5]. Chou LB, Malawer MM, Analysis of surgical treatment of 33 foot and ankle tumorsFoot Ankle Int 1994 15:175-81. [Google Scholar]
[6]. Machen SK, Easley KA, Goldblum JR, Synovial sarcoma of the extremities: a clinicopathologic study of 34 cases, including semi-quantitative analysis of spindled, epithelial, and poorly differentiated areasAm J Surg Pathol 1999 23:268-75. [Google Scholar]
[7]. Seale KS, Lange TA, Monson D, Hackbarth DA, Soft tissue tumours of the foot and ankleFoot Ankle 1988 9:19-27. [Google Scholar]
[8]. Weiss SW, Goldblum JR, Malignant Soft Tissue Tumours of Uncertain Type. In Weiss SW, Goldblum JRSoft Tissue Tumors 2001 4th edSt. LouisMosby [Google Scholar]
[9]. Damron TA, Beauchamp CP, Rougraff BT, Ward WG, Soft-tissue lumps and bumpsJ Bone Joint Surg 2003 85A:1142-55. [Google Scholar]
[10]. Fisher C, Synovial sarcomaAnn Diagn Pathol 1998 2:401-21. [Google Scholar]