Introduction
Dentistry, over the past few years has undergone and seen a lot of advancements in its daily practice [1]. Latest diagnostic imaging techniques like Ultrasonography, Cone beam computed tomography and procedures like Microsurgery, Implants, Lasers and Nanotechnology have made dentistry, as one of the front runners in medical fraternity [2]. With the above mentioned inventions, we have already entered a world of painless dentistry.
The success of any treatment modality in dentistry depends upon the tools by which the treatment is being carried out [3]. Tools as in hard tissue cutting tools such as micromotor handpiece, aerotor which remove enamel, dentin, cementum as well as bone. The amount and quality of hard tissue removal determines the post- operative outcome of any dental surgical procedure,be it implantology or Periodontology [4].
Traditional dental therapeutics involved hand cutting instruments such as Mallet, chisel followed by rotary instruments consisting of different burs.These instruments produced a lot of heat during bone cutting and required high amount of external copious irrigation.These instruments also exerted considerable pressure in osseous surgeries and hence endangered treatment of fractured and brittle bones [3].
To overcome the limitations of traditional tools, researchers have come up with advanced therapeutic devices which use the principle of ultrasonic microvibrations to make precise and selective cut on the bone in harmony with the surrounding tissues [4,5]. One of the novel methods to incorporate these properties of ultrasonic’s is, Piezosurgery. This is a relatively new alternative for bone-related procedures introduced in the field of dentistry. It has a wide potential for usage with the devices running according to the piezoelectric principles and capable of cutting by way of ultrasonic vibration [5,6]. These vibrations are low frequency modulated vibrations at 25 to 30 khz which selectively cut the bone without damaging adjacent soft tissues in particular with delicate structures such as schneiderian membrane or a nerve [6].
The piezoelectric devices are called in practice as piezosurgery with reference to the name of first device in the market [5].
Historical Background
The instruments used for ultrasonic cutting of bone create microvibrations which are the result of a piezoelectric effect, was first described by French physicists Jean and Marie Curie, in 1880 [7]. Catuna in 1953, Volkov and Shepeleva [8] in 1974 described cutting of hard tissue with ultransonic vibrations as piezoelectric effect. In 1981, its application was described by Aro et al., [9] in orthopaedic surgery, and Horton et al., [10] in oral and maxillofacial surgery.
Tomaso vercellotti an italian oral surgeon modified conventional ultrasonic technology [6].
In 1997 Mectron and Tomaso Vercellotti developed the idea of piezoelectric bone surgery. The main technological advancement was the adaptation of ultrasound movement for bone cutting. Mectron produced the first prototype device for piezoelectric bone surgery with which the first extraction treatments were performed. In 1999 Tomaso Vercellotti introduced the name PIEZOSURGERY® for the new method. Mectron also developed 2nd generation of the piezosurgery device in 2004 which was more powerful than the previous device. In the year 2009 3rd generation piezosurgery device was introduced [Table/Fig- 1]. Currently piezosurgery is very commonly and successfully used in implant dentistry.
The Equipment (Courtesy: Mectron Dental- India Pvt Ltd)

Mechanism of Action [
4–
6]
‘Piezo’ the term is derived from ‘piezein’ meaning pressure in Greek language.Piezosurgery works on the principle of ‘Pressure Electrification’, meaning when electric tension is applied across certain materials, the material in question expands and contracts, thus producing ultrasonic vibrations [5]. Materials used here are piezoelectrical crystals which generally include quartz, Rochelle salt and certain types of ceramic. When these crystals are subjected to an electrical charge, they expand and contract alternately to produce ultrasonic waves. Since these ultrasonic waves are mechanical in nature, they can induce disorganization and fragmentation of different bodies. The ultrasonic waves can allow segmentation of interfaces from solid to solid by means of distinct vibration, and solid-liquid by means of cavitation. In dentistry these two phenomena are used [5,6].
A variety of Piezoelectric oscillating tips can be chosen for particular applications. For example, a disc shape provides a plane ultrasonic wave, while curving the radiating surface in a slightly concave or bowl shape, further creating an ultrasonic wave that focusses at a specific point [5].
The microvibrations produced by piezoelectric unit are at a frequency of 25 to 29 khz modulated with a low frequency of 10 to 60 Hz and highest upto 30 KHz [4]. The linear vibrations of the tips range between 60 and 200 micro meter horizontally and a 20-60 micro meter in a vertical motion [11]. The ultrasonic tip vibrates at a controlled speed of 60-200mm/sec which is targeted to cut only mineralized tissue without damaging adjacent soft tissues [12].Frequency above 50khz is only capable of cutting neurovascular tissues and other soft tissues [13]. The vibration amplitude is also adjustable in the range of 30-60 micro meter.This allows constant and instantaneous adaptation of the power required depending on the resistance encountered by the tip.The power of the device is adjusted at 5W. Power and precision are indirectly proportional to each other. So, as the power increases, it requires thicker tips which produce imprecise cuts.Therefore 5W is the ideal compromise between power and precision [4]. The oscillating tip simultaneously drives coolant which produces cavitation effect [14].
The term cavitation describes the process of vaporisation, bubble formation and subsequent implosion into many fractions of its original size that occurs due to decrease in pressure as a result of ultrasonic vibration.When pressure increases, the voids implode and can generate an intense shockwave [5,14]. The cavitation effect necessitates low vapour pressure of the oscillating tip.This effect maintains bone temperature, washes away debris,regulates haemostasis and clears the field by the bursting of water bubbles under high pressure.This causes erosion and cleaning of the osseous crest.Henceforth increases visibility and ease of operation [5,15].
In addition cavitation also illustrates an anti bacterial property which helps in obtaining high predictability and low morbidity in bone surgery.The antibacterial property is attributed to the fragmentation of bacterial cell wall [14].
The action of piezoelectric device can be summarized by the following points:
Micrometric Cutting: Precise bone cutting accompanied by high tactile sensitivity.
Selective Cutting: Bone cutting without the risk of damaging adjacent soft tissues.
Asepsis: Sterile water [4].
Cavitation Effect: For maximum intra operative visibility and high predictability.
Minimum surgical stress: Excellent tissue healing [6,9].
Equipment
The first model of piezoelectric devices was developed by Vercellotti et al., [6] and is generally called as ‘Piezosurgery’ in reference to the first model. Piezoelectric devices typically consist of a handheld device [handpiece], a base unit and a foot pedal/switch which are connected to main power unit [Table/Fig-1]. There are different-shaped inserts that correspond to different applications that can be screwed into the handpiece. The handpiece is controlled by a foot pedal with settings that can be adjusted on the base unit. The device has a holder for the hand piece, and contains irrigation fluids that create an adjustable jet of 0–60 ml/minute through a peristaltic pump. It removes debris from the cutting area and ensures precise cutting. It also maintains a blood-free operating area because of cavitation of the irrigation solution [5], and gives greater visibility particularly in complex anatomical areas. The control panel of the device consists of only 4 buttons which makes it easy and economical. The speed and the irrigation can be controlled by (-) and (+) buttons present on the control panel [Table/Fig-1]. Throughout the procedure there is continuous irrigation flow ensured by internal safety control [6,15].
While using the piezosurgical handpiece care should be taken not to apply too much load or pressure. Pressure exhibited by handpiece is inversely related to bone temperature and therefore, Inserts should be moved continuously backward and forward at a high speed with minimum pressure [5]. To achieve maximum depth, 150gms of load is needed [16]. Excessive pressure decreases oscillations and hence the cutting ability.
The cutting characteristics of piezosurgery are dependent upon the degree of bone mineralization, its density, the design of the insert and the pressure applied on the handpiece [17]. The frequency of ultrasonic vibrations(Hz), the level of power(W) and the water spray are three adjustable settings that should be set in accordance with the intended procedure [5].
Osteotomy insert tips (Courtesy: Mectron Dental- India Pvt Ltd)
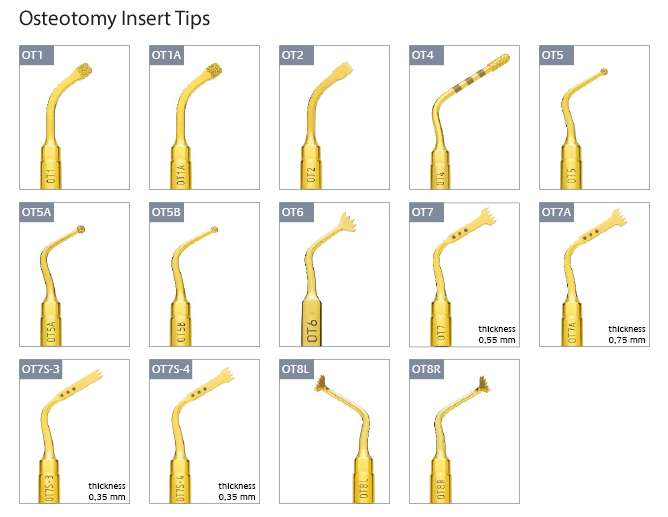
The grades of precision, predictability and treatment outcome of any surgical procedure depend upon the armamentarium design and the technique used [5,18]. Depending upon the need and type of surgery, different insert designs can be used.The size and shape of the inserts as well as the purpose of the same determine the level of power required.For eg: saw shaped insert used to cut highly mineralized bone, uses high level of power [5,18] .
Sharp Inserts: The sharp edge of the instruments enable gentle and effective cut on the mineralised tissue. They are useful in osteotomy procedures like implant site preparation, osteoplasty and other surgical techniques which require fine and well defined cut.
Eg:Design No: OT-7, EX1,OP-3,IM2A and IM3P
Smoothening Inserts: They have diamond surface coating which enables precise and controlled work on bony structures to obtain the final bone shape. These inserts are specifically useful to prepare difficult and delicate structures such as sinus window or access to nerve [18].
Eg: Design no: OT5,OT-1, OT-4 and OP-4
Blunt Inserts: They have blunt, dull and rounded non cutting tip. These tips play wonders in atraumatic elevation of the sinus membrane for grafting procedures [5].
Insert Tip Color: Insert tips are color coded by either Gold or steel. Gold insert tips are used to treat bone.It is obtained by applying titanium nitride coating to improve the surface hardness which further increases longevity of the insert tip.Steel is used to treat soft tissue or delicate structures such as roots of teeth [4].
Applications of piezosurgery
The application of piezosurgery in medical fraternity has already been established. It has been used in number of surgical procedures like rhinoplasty, orthopaedic and wrist surgery, mastoidectomy, facial, neurosurgery, traumatology, opthalmology, head and neck surgery as well as plastic and reconstructive surgery [6,17,19,20].
The dental applications of piezosurgery can be categorised owing to different specialities:
Oral and Maxillofacial Surgery: Piezosurgery has a wide role in oral and maxillofacial surgical procedures. Piezosurgery can be very easily and successfully used in cases which require meticulous handling of delicate structures like soft tissues, piece of a tooth; impacted teeth which is close to anatomical structures [5].
Piezosurgery has been effectively used in atraumatic tooth extraction, enucleation of cyst and tumour, sinus lift procedure,alveolar ridge expansion, ridge augmentation, bone harvesting (Chips and blocks), dentoalveolar surgery, atraumatic dissection of sinus mucosa, alveolar distraction osteogenesis, jaw resection, TMJ ankylosis/resection [6,11,18,21].
During tooth extraction vigorous movements produced by traditional forceps causes forceful tearing of Sharpey’s fibres away from the bundle bone surrounding the socket. This causes disruption of blood supply and trauma to the extraction socket which in turn delays healing [21]. Piezosurgery has been used in this regard to obtain atraumatic extraction which results in faster healing and better recovery. Ultrasonic vibrating ‘Syndesmotomes’ are recently developed tips for tooth and root extraction [21]. The tip is inserted through gingival sulcus between the space occupied by periodontal ligament between the root and the socket. The periodontal fibres are cut upto or greater than 10mm. Thus when the most apical fibres are severed, the coronal portion is not submitted to a violent ‘rip’.Therefore, in this way nearly atraumatic extraction can be achieved [21].
Implantology: In implantology, piezosurgery can be used in implant socket preparation, recontouring of alveolar crest, mental nerve repositioning, mobilisation of inferior alveolar nerve and simultaneous implant placement and, immediate implant placement after extraction [22].
The role of Piezosurgery is symbolic, delicately helps in critical procedures like alveolar ridge expansion which involves separation of palatal and vestibular bone flaps and subsequent implant placement [23].
Sinus elevation with traditional burs is often associated with complications such as membrane perforation, intra operative bleeding and surgical trauma. To avoid such mishap, piezosurgical insert with blunt tip is useful in atraumatic elevation of the membrane, followed by successful grafting procedure [5,6].
Endodontics: Hemisection, root amputation, apical resection and endodontic treatment can be easily performed with the help of piezosurgery [24].
Periodontics: Apart from routine scaling and root planning piezosurgery can be used in periodontal surgical procedures such as osteoplasty and osteotomy, crown lengthening procedure, Resective and regenerative surgery [4,24].
Orthodontics: Osteotomy, corticotomy and orthodontic micro- surgery can be successfully done with the help of piezosurgery [5].
Biological effects on bone and osseous response to piezosurgery
In any type of osseous surgery the effects of mechanical instruments on the structure of bone and the viability of cells is important. Any alteration in temperature are injurious to cells and may cause necrosis of bone [25].
Erikson et al., [26], showed that local bone necrosis would occur in cases where the temperature exceeds 470C for 1 minute due to the contact of rotating tools.
Piezosurgery not only selectively cuts the hard tissue but also produces the haemostatic effect on the surrounding tissue [14,27,28]. Because this technique preserves the surrounding soft tissues, it can be applied in areas where bone is in close proximity to vital and delicate structures such as nerves, blood vessels or the sinus mucosa [6].
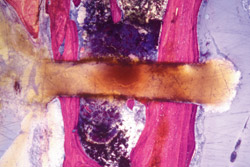
Microtopographic and histomorphometric studies have shown that piezosurgery is preferred over other tools for harvesting vital bone [25,26]. ‘Perfect integrity of the Osteotomized surfaces with a cut which is clean, regular and without imperfections or pigmentation’. The bone surface which was cut using the piezoelectric device showed no sign of lesions to the mineralized tissues and presented live osteocytes with no sign of cellular suffering [29].
[Table/Fig-3,4,5] Recently, Stubinger et al., [27] showed that autologous bone from the zygomatico-maxillary region that had been harvested with a piezoelectric device, could be used in augmentation for stable and aesthetic placement of oral implant after a five months healing.
Osteotomy by bone saw: limited surgical control and lack of precision resulting in trauma to the adjacent tissues as well as osteonecrosis
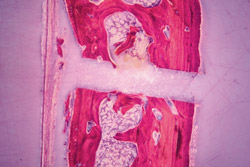
Osteotomy by bone bur: macrovibrations produced by the bur also limit the access to surgical field and produce damage to the adjacent tissues

Osteotomy by piezosurgery: easy and precise cut, with reduced trauma and complications to the adjacent tissues (Courtesy: Mectron Dental- India Pvt Ltd)
Another histomorphological study reveals that the piezoelectric surgery increases the concentration of Bone Morphogenic Protein (BMP-4), TGF beta-2, Tumor Necrosis Factor and Interleukin-1, 10 and decreases some of the pro inflammatory cytokines in the bone [4,5,25]. Thus, neo osteogenesis was proven to be consistently more active in cases where piezosurgery is used [5]. Harder et al., [30] observed that the critical temperature rises only when the irrigation volume is as low as 20 ml per minute.Piezosurgery, therefore has a potential role in osseous surgery [6,25].
Advantages
Precise and selective bone cutting.
Effective and faster healing.
Less invasive and so reduced post operative pain.
Favourable osseous response.
Protects vital structures such as Schneiderian membrane and nerves.
Maintains asepsis due to sterile water environment.
Better tactile sensitivity.
Owing to the effect of cavitation, surgery is performed in bloodless field and ensuring optimal visibility.
Does not produce noise during the procedure.
No risk of emphysema [31].
Reduce traumatic stress.
Can be applied in paediatric and medically compromised patients.
All of the above factors increase patient’s compliance.
Disadvantages
The largest disadvantage of piezosurgical unit is increased operating time required for bone preparation [32].
Contraindications
There are no absolute contraindications, but one such is electrical pacemakers, in either the patient or the operator, which is a contraindication for piezosurgery. Age factor is a relative contraindication for any surgery [4,33].
Conclusion
This review emphasizes on the clinical importance of piezosurgery pertaining to its use in dental sciences.Piezosurgery ensures the 3 ‘P’s, that is Predictability, less post operative pain and increased patient’s compliance. Need not say, the use of piezosurgical device, a novel invention is not only limited to the field of dental surgery, but far beyond the horizon, in more complex cases and in all interdisciplinary problems pertaining in the effect of medical and dental sciences.
[1]. Manton DJ, Diagnosis of the early carious lesionAusDent J 2013 58(suppl):135-39. [Google Scholar]
[2]. Filo K, Sehneider T, Locher MC, Kruse AL, Lubbers HT, The inferior nerve’s loop at the mental foramen and its implications for surgeryJ Am Dent Ass 2014 145(3):260-69. [Google Scholar]
[3]. Rashad A, Kaiser A, Prochnow N, Schmitz I, Hoffmann E, Haurer P, Heat Production during different Ultrasonic and conventional osteotomy preparation for dental ImplantsClin Oral Implant Res 2011 22(12):1361-65. [Google Scholar]
[4]. Chopra P, Chopra P, Piezosurgery and its applications in Periodontology and ImplantologyInternational Journal of Contemporary Dentistry 2011 2(4):16-24.(http://edentj.com/index.php/ijcd/article/view/404/251) [Google Scholar]
[5]. Yaman Z, Suer BT, Piezoelectric surgery in oral and maxillofacial surgeryAnnals of Oral and Maxillofacial Surgery 2013 1(5):1-9. [Google Scholar]
[6]. Vercellotti T, Paoli SD, Nevins M, The Piezoelectric Bony Window Osteotomy and Sinus Membrane Elevation: Introduction of a New Technique for Simplification of the Sinus Augmentation ProcedureInt J Perio Rest Dent 2001 21:561-67. [Google Scholar]
[7]. Hoigne DJ, Stubinger S, Kaenel OV, Shamdasani S, HHasenboehler P, piezoelectric osteotomy in hand surgery: first experiences with a new techniqueBMC Musculoskeletal Disorders 2006 7(36):1-4. [Google Scholar]
[8]. Volkov MV, Shepeleva IS, The use of ultrasonic instrumentation for the transection and uniting of bone tissue in orthopaedic surgeryReconstr Surg Traumatol 1974 14(0):147-52. [Google Scholar]
[9]. Aro H, Kallioniemi H, Aho AJ, Kellokumpu-Lehtinen P, Ultrasonic device in bone cutting. A histological and scanning electron microscopical studyActa Orthop Scand 1981 52(1):5-10. [Google Scholar]
[10]. Horton JE, Tarpley TM Jr, Jacoway JR, Clinical applications of ultrasonic instrumentation in the surgical removal of boneOral Surg Oral Med Oral Pathol 1981 51(3):236-42. [Google Scholar]
[11]. Garcia AC, Frcitas MD, Martin MS, Garcia AG, Piezoelectric and conventional osteotomy in Alveolar Distraction Osteogenesis in a series of 17 patientsInt J-Oral Maxillofac Implants 2008 23(5):891-96. [Google Scholar]
[12]. Seshan H, Konuganti K, Zope S, Piezosurgery in periodontology and oral implantologyJounIndSocPeriodontol 2009 13(3):155-56. [Google Scholar]
[13]. Schlee M, Steigmann M, Bratu E, Garg AK, Piezosurgery: basics and possibilitiesImplant Dent 2006 15(4):334-40. [Google Scholar]
[14]. Nalbandian S, Piezosurgery techniques in Implant DentistryAustralasian Dental Practice 2011 :116-26. [Google Scholar]
[15]. Sohn DS, Ahn MR, Lee WH, Yeo DS, Lim SY, Piezoelectric Osteotomy for Intraoral Harvesting of Bone BlocksInt J Periodontics Restorative Dent 2007 27(2):127-31. [Google Scholar]
[16]. Claire S, Lea SC, Walmsley AD, Characterisation of bone following ultrasonic cuttingClin Oral Investig 2013 17(3):905-12. [Google Scholar]
[17]. Vercelotti T, Technological characteristics and clinical indications of piezoelectric bone surgeryMinerva Stomatol 2004 53(5):207-14. [Google Scholar]
[18]. Wallace SS, Stuart J, Forum,Schneiderian. Membrane Perforation Rate During Sinus Elevation Using Piezosurgery; Clinical Results of 100 Consecutive CasesInt J Perio Resto Dent 2007 27:413-19. [Google Scholar]
[19]. Salami A, Vercellotti T, Mora R, Dellepiane M, Piezoelectric bone surgery in otologic surgeryOtolaryngol Head Neck Surg 2007 136(3):484-85. [Google Scholar]
[20]. Kotrikova B, Wirtz R, Krempien R, Piezosurgery: a new safe technique in cranial osteoplasty?Int J Oral Maxillofac Surg 2006 35(5):461-65. [Google Scholar]
[21]. Blus C, Moncler S, Atraumatic tooth extraction and immediate implant placement with piezosurgery: evaluation of 40 sites after at least one year of loadingInt J Perio Rest Dent 2010 30(4):355-63. [Google Scholar]
[22]. Lazzara RJ, Immediate implant placement into extraction sites: Surgical and restorative advantagesInt J Perio Rest Dent 1989 9(5):332-43. [Google Scholar]
[23]. Vercellotti T, Piezoelectric surgery in Implantology; a case report- a new piezoelectric ridge expansion techniqueInt J Perio Rest Dent 2000 20(4):358-65. [Google Scholar]
[24]. Walmsley AD, Laird WR, Lumley PJ, Ultrasound in dentistry. Part 2- Periodontology and endodonticsJ Dent 1992 20(1):11-17. [Google Scholar]
[25]. Vercelotti T, Nevins ML, Kim DM, Wada K, Schenk RK, Florellini JP, Osseous response following resective therapy with piezosurgeryInt J Perio Rest Dent 2005 25(6):543-49. [Google Scholar]
[26]. Eriksson AR, Albrektsson T, Albrektsson B, Heat caused by drilling cortical bone. Temperature measured in vivo in patients and animalsActa Orthop Scand 1984 55(6):629-31. [Google Scholar]
[27]. Stubingers Ultrasonic bone cutting in oral surgery: a review of 60 casesUltraschallMed 2008 29(1):66-71. [Google Scholar]
[28]. Troiani C, Piezoelectric surgery: a new reality to cut and manage bone in maxilla-odonto-stomatologyInt J Maxillo odontostomatology 2005 4:23-8. [Google Scholar]
[29]. Vercelotti T, Crovace A, Palermo A, Molfetta A, The piezoelectric osteotomy in orthopaedics: clinical and histological evaluations (pilot study in animals)Mediterranean Journal of Surg Med 2001 9:89-95. [Google Scholar]
[30]. Harder S, Wolfart S, Mehl C, Kern M, Performance of Ultrasonic Devices for Bone Surgery and Associated Intraosseous Temperature DevelopmentInt J Oral Maxillofac Implants 2009 24:484-90. [Google Scholar]
[31]. Vercellotti T, Technological characteristics and clinical indications of piezoelectric bone surgeryMinervastomatol 2004 53:207-14. [Google Scholar]
[32]. Labanca M, Azzola F, Vinci R, Rodella L, Piezoelectric surgery: twenty years of useBr J Oral MaxillofacSurg 2008 46(4):265-69. [Google Scholar]
[33]. Walsh L J, Piezosurgery : an increasing role in dental hard tissue surgeryAustralasian Dental Practice 2007 :52-56. [Google Scholar]