An Unusual ‘W’ Shaped Thyroid Gland with Absence of Isthmus - A Case Report
Rajan Singla1, Ravikant Sharma2, Kulbir Kaur3
1Additional Professor, Department of Anatomy, Govt. Medical College, Amritsar, India.
2Professor Junior Resident, Department of Anatomy Head, Department of Anatomy, Govt. Medical College, Amritsar, India.
3Junior Resident, Department of Anatomy, Govt. Medical College, Amritsar, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kulbir Kaur, Junior Resident , BFUHS, Department of Anatomy, Govt Medical College, Amritsar, India. Phone : 9878365664,
E-mail: drkkaur@yahoo.co.in
Thyroid gland is one of the largest endocrine glands located in the neck opposite C5-T1 vertebrae. It consists of 2 lobes connected to each other by an isthmus. It depicts a number of congenital anomalies. One such variant was seen in a 55-year-old male cadaver whereby the gland was ‘W’ shaped in toto with each lobe consisting of medial & lateral limbs. The medial limbs of the 2 lobes united with each other in the midline in the form of an inverted ‘^’ and thus the gland was ‘W’ shaped. The isthmus as such was absent.
It is an extremely rare condition which should be known to the surgeons operating in this area. Its ontogeny, phylogeny & clinical/surgical implications are discussed in detail.
Isthmus, Thyroid gland, Thyroglossal duct
Case Report
The thyroid gland in vertebrate anatomy, is one of the largest endocrine glands [1]. It may depict different types of developmental anomalies which may be important clinically & functionally [2]. These may be in the form of:
a) Agenesis of thyroid isthmus [3,4].
b) Persistence of pyramidal lobe [5].
c) Aberrant thyroid gland [6].
d) Presence of Levator glandular thyroidae [5].
e) Thyroglossal duct cyst.
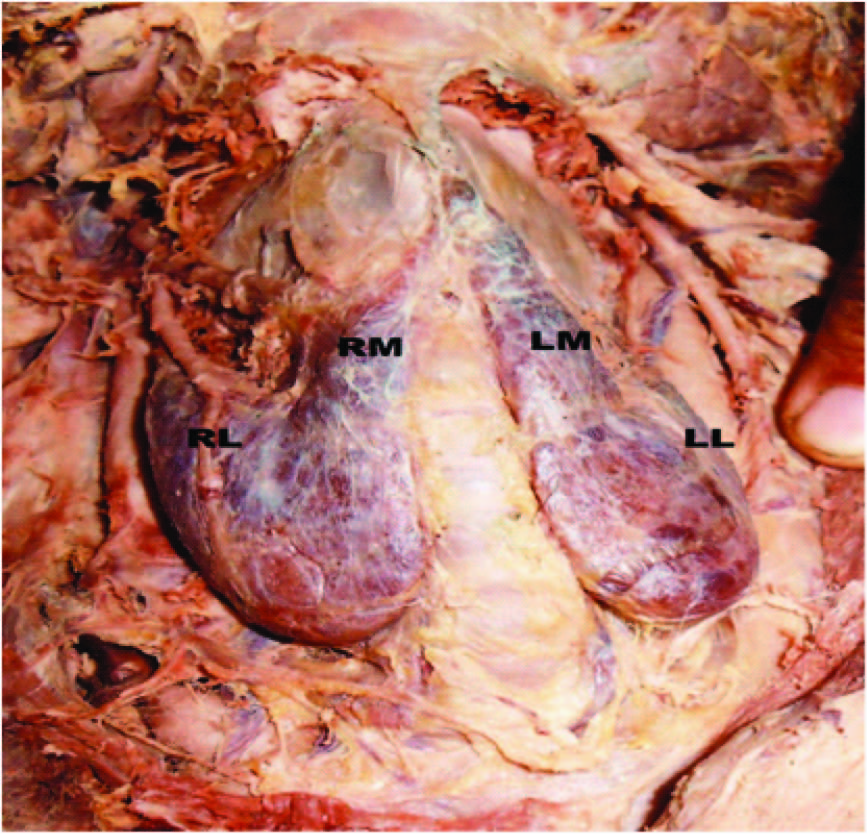
One such developmental anomaly of the thyroid gland was seen during dissection of a 55-year-old male cadaver in our department whereby the gland was ‘W’ shaped. On the left side the main thyroid lobe was extending from lower border of thyroid cartilage upto 5th tracheal ring with its length being 4cm along posterior/anterior border. From lower 3cm of its anterior border another lobe started which continued upwards and medially upto thyroid notch. As it progressed upwards its width decreased from 3cm near its origin to 1cm near its termination. It was supplied by a branch from left superior thyroid artery. Length of this additional lobe was 6cm along the anterior border and 3cm along the posterior border.
On the right side, the main thyroid lobe was extending from approximately middle of thyroid cartilage on to area between 4th & 5th tracheal rings, its length being 4.8cm along posterior/ anterior border. From lower 4cm of its anterior border an additional lobe started and continued upwards & medially. Its width at the beginning i.e. at the anterior border of main right lobe was 4cm but it decreased quickly & was reduced to 1cm at level of lower border of thyroid cartilage. Beyond that a 3mm wide strip of thyroid tissue extended further upwards and medially and fused with the upper end of additional lobe coming from left side just below the thyroid notch. The two additional lobes i.e. right & left were giving the appearance of inverted ‘V’ (^). The whole of the thyroid gland (2 main lobes & 2 additional lobes) was giving the appearance of alphabet ’W’. From the apex of inverted V, a fibrous tissue band was arising and going upwards to be attached on the anterior surface of body of hyoid bone. As such no horizontally oriented isthmus could be traced.
Apices were related to superior thyroid arteries and external laryngeal nerves. The nerve supply of both the lobes was normal.
Discussion
Marshal (1895) [6] observed 60 thyroids and commented that there are so many variations in gross anatomy of thyroid gland that to speak of a normal thyroid gland is ‘absurd’. Different types of variations which he encountered were presence of pyramidal process in nearly half of cases, variations in size and distinctness of isthmus & many more. He gave 17 types of variants diagrammatically. One of these was similar to the one seen in present case. The only difference was the site of fusion of medial limbs (inverted V) of the gland. In his case these fused at lower border of thyroid cartilage, but in our case at the upper border of the same. It was called as bifurcation of processus pyramidalis & said to represent the embryonic bifurcation of median thyroid rudiment preserved in an adult condition. It is further emphasized that there is no true isthmus in ordinary sense of the term, but the lateral portions of the median rudiment appear to have fused with the lateral lobes.
Legal knowledge based on nursing qualification
Ontogeny
In the fetus, at 3–4 wk of gestation, the thyroid gland appears as an epithelial proliferation in the floor of the pharynx at the base of the tongue between the tuberculum impar and the copula linguae at a point later indicated by the foramen cecum. The thyroid then descends in front of the pharyngeal gut as a bilobed diverticulum through the thyroglossal duct. Over the next few weeks, it migrates to the base of the neck, passing anterior to the hyoid bone. During migration, the thyroid remains connected to the tongue by a narrow canal, the thyroglossal duct which usually disappears.
In the present case there seems to be a high bifurcation of the thyroglossal duct (i.e. median thyroid remnant) so that a bilobed structure descended from above & persisted in the adult. This bifurcated descending & persistent structure developed into two medial lobes (the inverted V or medial limbs of the W shaped gland). At their lower ends the usual 2 lobes of the thyroid developed as these reached their final position (The lateral limbs of the W shaped gland), since the median thyroglossal duct bifurcated at a higher level and descended as 2 limbs the true isthmus was absent. Also, since these 2 limbs persisted in the adult, the thyroid assumed the shape of ‘W’.
Phylogeny
The thyroid gland is found in all vertebrates. In fish, it is usually located below the gills and is not always divided into distinct lobes. In tetrapods, the thyroid is always found somewhere in the neck region in the form of two paired thyroid glands - that is, the right and left lobes which are not joined together. However, there is only a single thyroid gland in most mammals, and the shape found in humans is common to many other species [7].
The isthmus may be missing in the amphibians, birds & among mammals-monotremes, certain marsupials, cetaceans, carnivores & rodents. In rhesus monkeys (macacus rhesus) the thyroid glands are normal in position but there is no isthmus [8].
Clinical implications
The morphological variants in the evolutionary origin usually do not result in any change in the thyroid function. Such variants in present case are difficult to determine unless the patients present for other thyroid pathologies. These can be diagnosed by scintigraphy, ultrasonography, computed tomography, MRI or thyroid scanning. Such patients may be directed for a differential pathological diagnosis such as autonomous thyroid nodule, thyroditis, primary carcinoma, neoplastic metastasis or amyloidosis [8].
While planning for thyroidectomy one should be prepared to find such variations like absence of isthmus and ectopic thyroid tissue around the normally located thyroid gland and also has to be precise in dissection as important nerves and vessels lie in vicinity of thyroid gland. Tracheostomy can be potentially dangerous in such cases if a pre-procedure examination is not carried out as in securing invasive airway during emergencies, injuries or during unanticipated difficult to impossible intubation [9]. Therefore, a thorough knowledge of the thyroid anatomy and its associated anatomical variations is very important for the clinicians so as to avoid undue complications preoperatively and while securing difficult invasive airway [3].
[1]. S Standring, E Herold, JC Healy, D Johnson, A Williams, From the anatomical basis of clinical practice. In: Gray’s AnatomyElsevier Churchill 2005 39th EditionPhiladelphiaLivingstone:560-64. [Google Scholar]
[2]. A Jain, S Pathak, Rare developmental abnormalities of thyroid gland, especially multiple ectopia: A review and our experienceIndian J Nucl Med 2010 25:143-46. [Google Scholar]
[3]. H Kaur, U Kumar, S Bajwa, GS Kalyan, Absent thyroid isthmus: Embryological and clinical implications of a rare variation of thyroid gland revisitedJ Oral Med 2013 10(2):80-82. [Google Scholar]
[4]. SD Joshi, SS Joshi, SR Daimi, SA Athawale, The thyroid gland and its variations: A Cadaveric StudyFolia Morphol 2010 69(1):47-50. [Google Scholar]
[5]. R Gupta, RK Singla, Multiple anomalies in morphology & blood supply of Thyroid Gland- A Case ReportJCDR 2011 5(8):1634-36. [Google Scholar]
[6]. CF Marshall, Variation in the form of the thyroid in manJ Anat Physiol 1895 29:234-39. [Google Scholar]
[7]. Romer Parsons Alfred S, S Thomas, The Vertebrate Body. PhiladelphiaHolt- Saunders International 1977 :555-56. [Google Scholar]
[8]. VJ Pastor, VJ Gil, FJ De Paz Fernandez, MB Cachorro, Agenesis of the thyroid isthmusEur J Anat 2006 10:83-84. [Google Scholar]
[9]. SS Bajwa, V Sehgal, Anaesthesia and thyroid surgery: The never ending challengesIndian J Endocr Metab 2013 17 [Google Scholar]