Cystic Endosalpingiosis of Uterine Parametrium- A Scarcely Encountered and Sparsely Documented Entity
Hemalatha A.L1, Ashok K.P2, Anoosha K3, Indira C.S4
1Professor, Department of Pathology, Adichunchanagiri Institute of Medical Sciences, B. G. Nagar, Mandya, Karnataka, India.
2Post Graduate, Department of Pathology, Adichunchanagiri Institute of Medical Sciences, B. G. Nagar, Mandya, Karnataka, India.
3Post Graduate, Department of Pathology, Adichunchanagiri Institute of Medical Sciences, B. G. Nagar, Mandya, Karnataka, India.
4Tutor, Department of Pathology, Adichunchanagiri Institute of Medical Sciences, B. G. Nagar, Mandya, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. . Hemalatha. A.L No: 156, 12th Cross, 2nd Main, Jayanagar, Mysore- 570 014, India. Phone : 8453399335,
E-mail: halingappa@gmail.com
“Endosalpingiosis” refers to the presence of fallopian tube-like epithelium outside fallopian tubes. It merits attention both by Clinicians and Pathologists since it is a benign, non- neoplastic condition which maybe easily misjudged as carcinoma mainly due to the rarity of its occurrence and lack of awareness owing to paucity of its documentation in literature. Further, salpingiosis can undergo massive cystic change thereby mimicking a tumour when it is referred to as cystic salpingiosis. We present one such extremely rare case of cystic salpingiosis of uterine parametrium in a 40-year-old lady along with an extensive review of literature which revealed that about 10 cases have been documented till date.
Ciliated low cuboidal epithelium, Mullerianosis, Parametrium
Case Report
A 40-year-old lady (gravida 3 para 3 miscarriage) presented to Gynaecology department with mass per vagina. She was diagnosed with 2nd degree uterovaginal descent associated with cystocoele, rectocoele and enterocoele. Per-operatively, a cystic mass attached to the uterine fundus was detected. While attempting to deliver it vaginally along with the uterus and cervix, the cyst got ruptured and oozed clear serous fluid. Vaginal hysterectomy along with cystocoele repair was done. Uterus along with the cervix and the cyst attached to the uterine fundus were removed while the bilateral adnexae were retained since they were normal in appearance. The specimen was submitted for histopathological examination.
Histopathological Findings
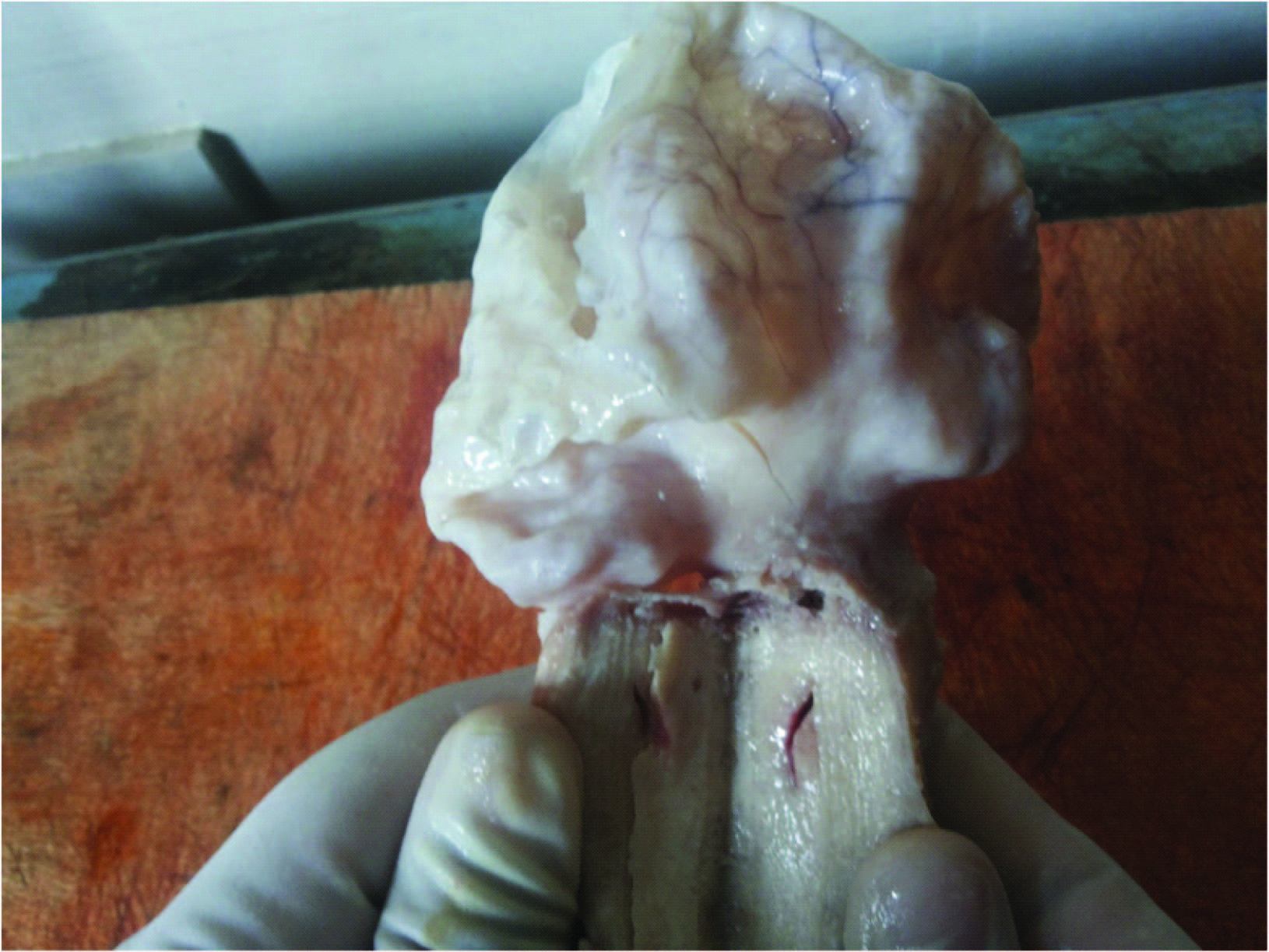
Gross Examination- Specimen consisted of uterocervix with a cyst attached to uterine fundus. Uterocervix measured 8 x 3.5 x 2 cms. The cyst measured 7.5 x 5 cms and showed prominent congested blood vessels on the serosal surface [Table/Fig-1] .
Cut Section of Uterocervix- Showed endometrial thickness of 1 mm. The uterus appeared hypoplastic.
Cut Section of the Cyst- Showed no continuity between the cyst and the endometrial cavity. The cyst wall was in continuity with the parametrium. The inner wall of the cyst showed congested blood vessels [Table/Fig-2] .
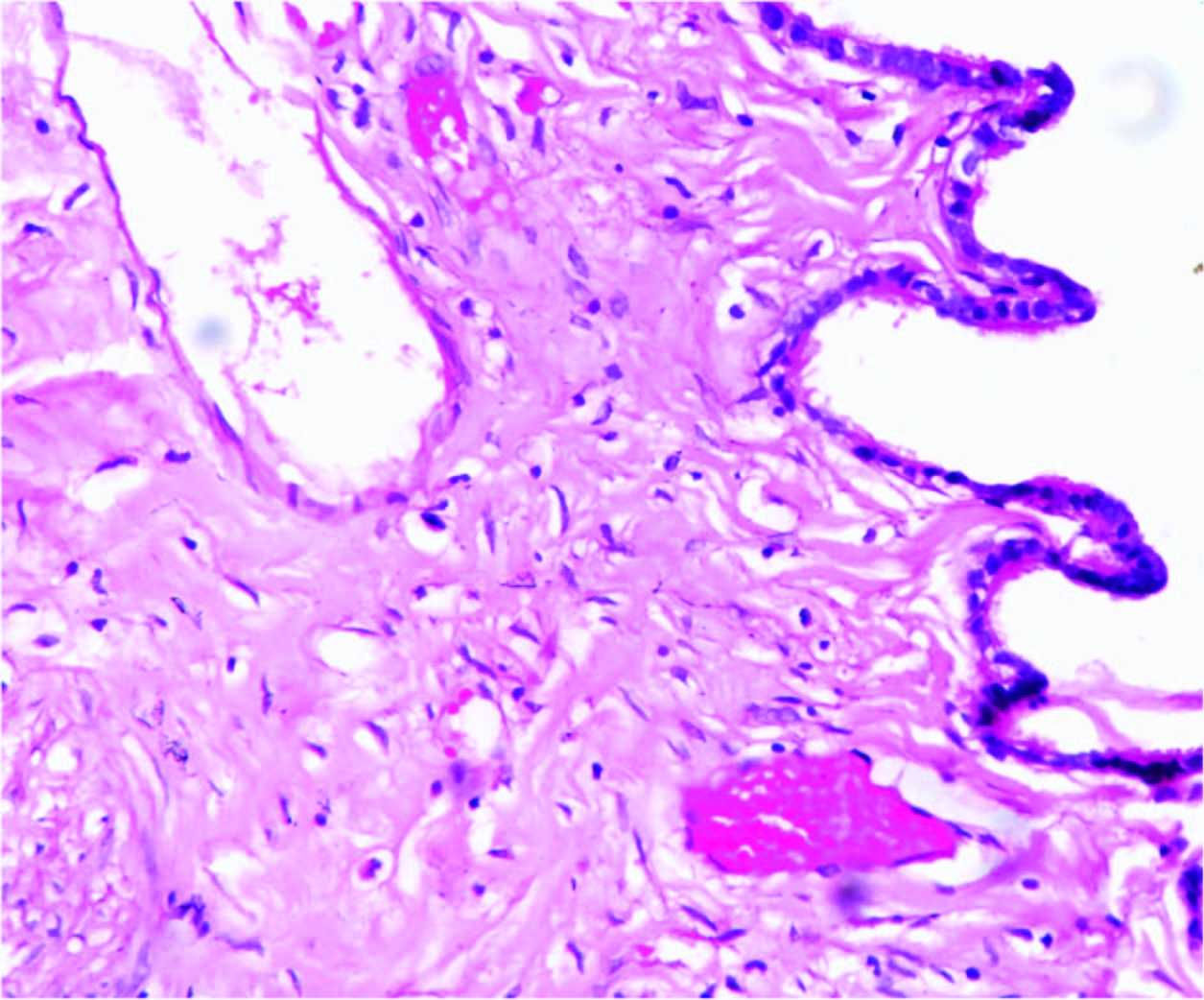
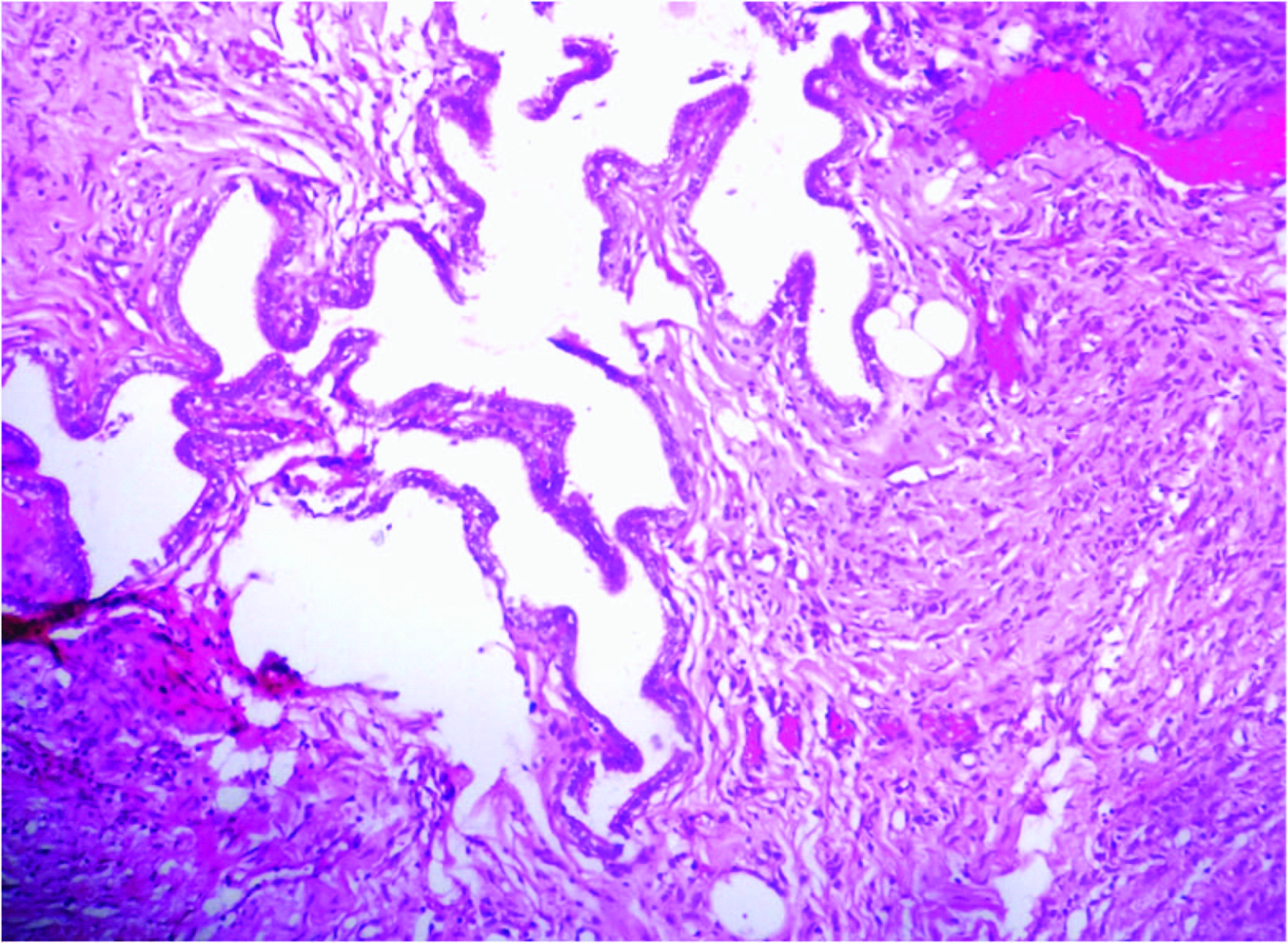
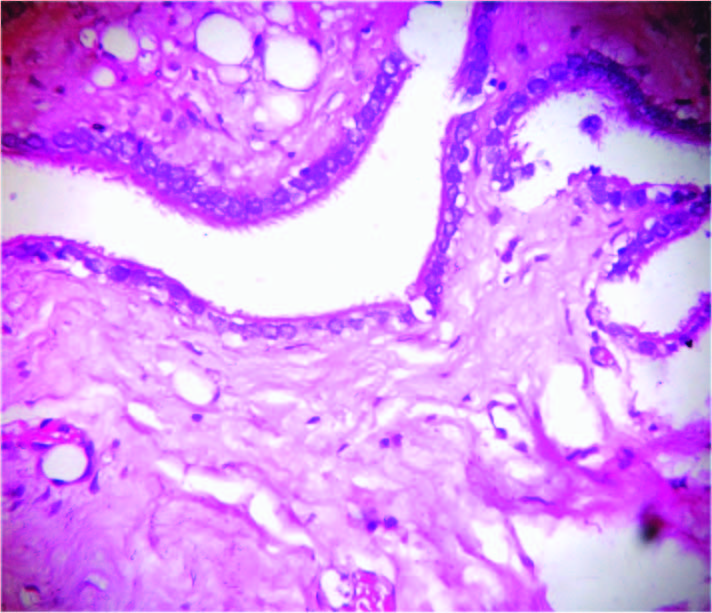
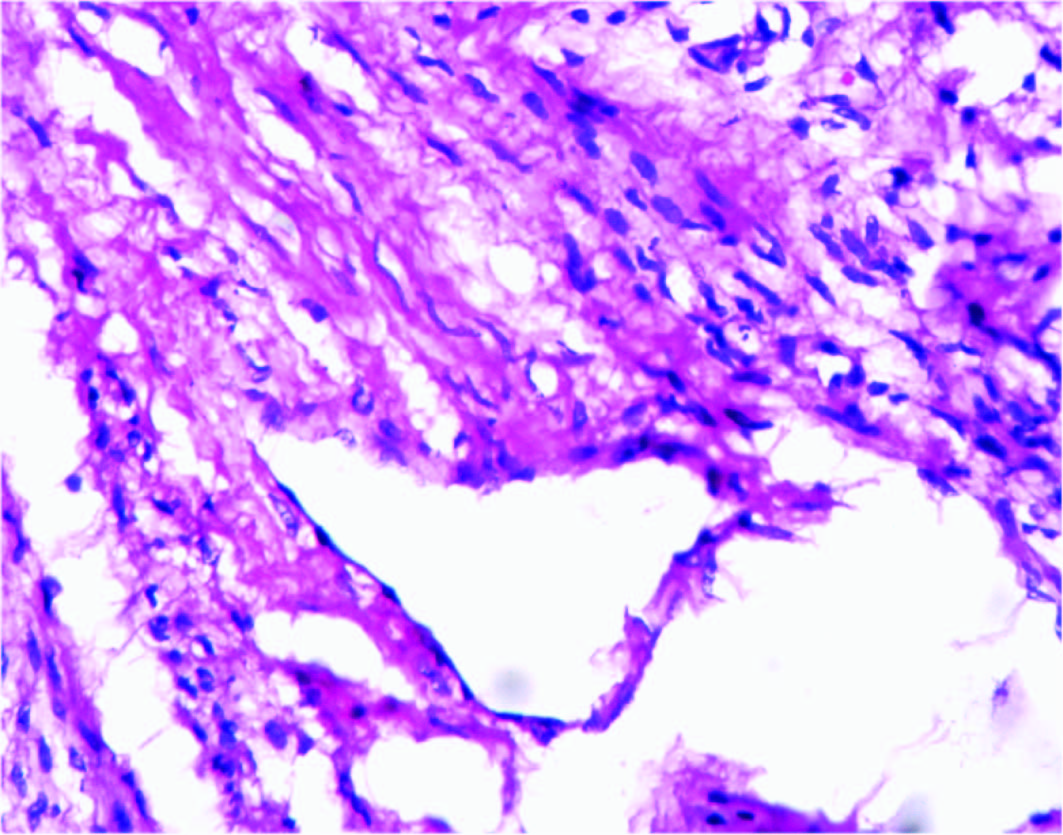
Microscopic Examination- Uterocervix showed atrophic endometrium and chronic polypoidal endocervicitis. The cyst arising from the uterine parametrium showed flattened low cuboidal epithelial lining [Table/Fig-3] . The cyst wall was continuous with the parametrium of uterine fundus. Focal areas in the wall showed embedded fallopian tubal epithelium [Table/Fig-4,5] . Multiple tiny cystic spaces and glandular structures lined by low cuboidal epithelium were seen in the cyst wall [Table/Fig-6] .
Histopathological Diagnosis- Cystic Endosalpingiosis
Discussion
The term “Endosalpingiosis” implies the presence of fallopian tubal type of ciliated low cuboidal epithelium in sites other than the fallopian tubes. It is a non- neoplastic lesion which is homologous to endometriosis and endocervicosis [1] . All these three entities are together grouped under the umbrella of “Mullerianosis” which includes epithelial proliferations of normal structures of the female genital tract involving tissues such as uterus, ovaries, fallopian tubes, urinary bladder, appendix, colon, omentum, pelvic/ retroperitoneal and para aortic lymph nodes [2,3] . The pathogenesis involves metaplasia of peritoneal pleuripotential coelomic epithelium into fallopian tube- like, ciliated, low cuboidal epithelium. The lesions which show metaplastic serous differentiation are also clubbed under this entity.
Endosalpingiosis was first described by Sampson in the year 1930 when he used it as a synonym for endometriosis [1] . Clement and Young reported four cases of florid cystic endosalpingiosis of the uterus with tumour- like manifestations in 1999. One of their four cases had transmural uterine involvement by endosalpingiosis which was the first reported case of transmural uterine endosalpingiosis [4] . Most often, endosalpingiosis is asymptomatic and is incidentally discovered on microscopic examination. AP Cil et al., have reported tumour- like cystic endoslpingiosis in the uterine myometrium hrowing light on the fact that, salpingiosis could assume huge proportions in size by undergoing cystic changes and mimic neoplasms [5] . Similarly, our patient had a cystic mass attached to the uterine fundus on the serosal surface, thus mimicking a cystic neoplasm grossly. Paradoxically, our patient had remained asymptomatic despite the large size of the cyst attached to the uterine fundus. She had presented with third degree uterine prolapse along with cystocoele, rectocoele and enterocoele for which a vaginal hysterectomy was performed. The cyst had been incidentally detected per operatively. Since the origin of the cyst was from the serosal surface of the uterine fundus and since the bilateral fallopian tubes and ovaries were separate and normal in appearance, the clinician was perplexed as to the origin and nature of the cyst. Gross examination of the specimen after sectioning revealed that the cyst originated from the serosa of the uterine fundus and that, there was no continuity between the cyst and the endometrial cavity. Microscopic examination demonstrated presence of fallopian tubelike epithelium in the parametrium and the cyst wall lined by the same type of epithelium, which resolved the issue finally and helped clinch the diagnosis of cystic endosalpingiosis.
A similar case of tumour- like multilocular cystic endosalpingiosis of the uterine serosa has been reported by SN Lee et al., [6] and also by MK Heatley et al., [7] , A case of omental endosalpingiosis has been documented by G. Santeusanio et al.,[8] . Endosalpingiosis in association with ovarian surface epithelial tumour of borderline malignancy has been reported by K Ryoko et al., [9] . Tumour- like foci of endosalpingiosis have been rarely described in the vermiform appendix and the urinary bladder [10] .
Sometimes, endosalpingiosis may present with non-specific symptoms including pelvic pain, hyper or dysmenorrhoea or infertility [5,11] . They have been found in association with endometriosis and uterine leiomyomas [8] .
Endosalpingiosis closely resembles endometriosis from which it can be differentiated by the absence of characteristic endometrial stroma and cyclical hemorrhage. The other differential diagnoses include endocervicosis (characterized by tall, columnar, mucin-secreting epithelium), florid deep glands in the uterine cervix (which show continuity with the uterine canal), multiple peritoneal inclusion cysts or benign cystic mesothelioma which are distinguished by presence of mesothelial lining.
Gross picture of uterocervix with a cyst attached to uterine fundus

Gross picture of the cyst showing congested blood vessels
Cyst wall lined by low cuboidal epithelium- fallopian tube like, (H & E, ×400)
Fallopian tubal epithelium embedded within parametrium, (H & E,×100)
Ciliated columnar epithelium of tubal type within the parametrium, (H & E, ×400)
Cystic and glandular structures within the wall, (H & E, ×400)
Conclusion
This article highlights the importance of microscopic examination in resolving the crucial diagnostic dilemma that a rare, simple, benign and seldom reported entity like cystic endosalpingiosis could create. The worrisome fact that it could be misdiagnosed as adenocarcinoma when the actual treatment options are very simple given the benign and innocent nature of this condition which is easily amenable to treatment, calls for awareness and prompt recognition of cystic endosalpingiosis.
[1]. JA Sampson, Postsalpingectomy endometriosis, (endosalpingiosis)American Journal of Obstetrics & Gynecology 1930 20:443-80. [Google Scholar]
[2]. SC Lauchlan, The secondary Mullerian systemObstetrical & Gynecological Survey. 1972 27:133-46. [Google Scholar]
[3]. P Rosenberg, NappiL A Santoro, P Bufo, P Greco, Pelvic mass-like florid cystic endosalpingiosis of the uterus:a case report and a review of literatureArchives of Gynecology and Obstetrics 2011 83:519-23. [Google Scholar]
[4]. PB Clement, RH Young, NH Olsen, JJ Hefferren, Florid cystic endosalpingiosis with tumour-like manifestations: a report of four cases including the first reported cases of transmuralendosalpingiosis of the uterusAmerican Journal of Surgical Pathology 1999 23:166-75. [Google Scholar]
[5]. AP Cil, P Atasoy, SA Kara, Myometrial involvement of tumour-like cystic endosalpingiosis: a rare entityUltrasound in Obstetrics and Gynecology 2008 32:106-10. [Google Scholar]
[6]. SN Lee, MS Cho, SC Kim, WS Han, Tumour-like multilocular cystic endosalpingiosis of the uterine serosa: possible clinical and radiologic misinterpreted,”Acta Obstetricia et Gynecologica Scandinavica 2005 84:98-98. [Google Scholar]
[7]. MK Heatley, P Russell, Florid cystic endosalpingiosis of the uterusJ clinPathol 2001 54:399-400. [Google Scholar]
[8]. G Santeusanio, L Ventura, A Partenzi, LG Spagnoli, FT Kraus, Omentalendosalpingiosis with endometrial type stroma in a woman with extensive hemorrhagic pelvic endometriosisAmerican Journal of Clinical Pathology 1999 111:248-51. [Google Scholar]
[9]. K Ryuko, H Miura, A Abu-Musa, O Iwanari, M Kitao, Endosalpingiosis in association with ovarian surface papillary tumour of borderline malignancyGynecologic Oncology 1992 46:107-10. [Google Scholar]
[10]. A Cajigas, CA Axiotis, Endosalpingiosis of the vermiform appendix.Int J Gynecol Pathol 1990 9:291-95. [Google Scholar]
[11]. J Heinig, I Gottschalk, U Cirkel, R Diallo, Endosalpingiosis—an underestimated cause of chronic pelvic pain or an accidental finding? A retrospective study of 16 casesEuropean Journal of Obstetrics Gynecology and Reproductive Biology 2002 103:75-78. [Google Scholar]