Management of Ruptured Occult Left Hydronephrotic Kidney in 7-Year - old Boy: A Case Report
Rajendra K Ghritlaharey1, Santosh More2
1 Associate Professor, Department of Paediatric Surgery, Gandhi Medical College and Associated Kamla Nehru and Hamidia HospitalsBhopal, Madhya Pradesh, India.
2 Student, Department of Paediatric Surgery, Gandhi Medical College and Associated Kamla Nehru and Hamidia HospitalsBhopal, Madhya Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rajendra K Ghritlaharey, Associate Professor, Department of Paediatric Surgery, Gandhi Medical College and Associated Kamla Nehru and Hamidia Hospitals Bhopal, Madhya Pradesh 462 001, India. Phone : 0-9425009272, E-mail : drrajendrak1@rediffmail.com
Pre-existing, occult, congenital renal anomalies are often discovered during evaluation of children for blunt injury of the kidney and abdomen, presenting with or without haematuria. This is a report of 7-year-old boy; who presented with blunt injury abdomen with haematuria following fall from motorcycle. He had pallor, and features of hypovolumic shock and peritonitis. Skiagram of the abdomen showed haziness of the abdomen, without free gas under diaphragm. Ultrasonography (USG) of the abdomen revealed significant hemoperitoneum and gross hydronephrosis of the left kidney, which was undiagnosed previously. Exploratory laparotomy was done for peritonitis and the findings were hemoperitoneum, hematoma at the left mesocolon and left retroperitoneum. Postoperative computed tomography (CT) scan of the abdomen reported left hydronephrosis due to pelvi-ureteric junction (PUJ) obstruction with rupture of the renal pelvis. The ruptured hydronephrotic kidney was successfully managed by nephrostomy followed by delayed open dismembered Anderson-Hynes pyeloplasty. His postoperative recovery following pyeloplasty was uneventful and he was doing well at follow-up after a month of pyeloplasty.
Abdominal trauma, Nephrostomy, PUJ obstruction
Case Report
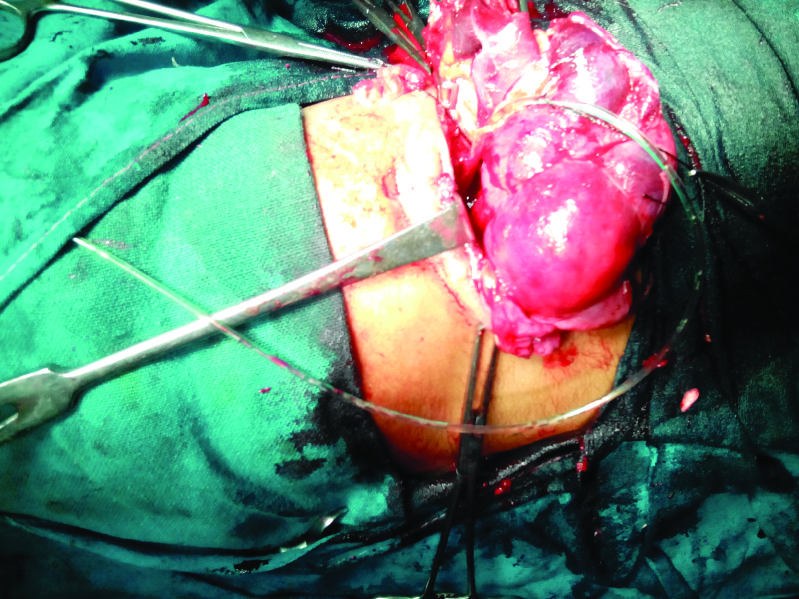
A 7-year-old boy was admitted with history of haematuria and blunt injury abdomen, following fall from motorcycle. He had pallor, and signs of hypovolumic shock. His abdomen was mildly distended, tense, and tender with absent bowel sounds. Standing skiagram of the abdomen showed haziness without free gas under diaphragm. USG examination of the abdomen revealed gross hydronephrosis of the left kidney due to PUJ obstruction and significant hemoperitoneum. The left kidney also showed hematoma at mid and lower pole. Right kidney, spleen and liver were normal. His Hb% was 7.2gm and needed blood transfusion during stabilization. Exploratory laparotomy was done for peritonitis and revealed about 300 ml of collected blood, haematoma at descending mesocolon [Table/Fig-1a] and hematoma at left retroperitoneum [Table/Fig-1b]. Left kidney could not be palpated well due to left retroperitoneal hematoma, although appeared grossly enlarged. Rest of the abdominal organs were normal and there were no active bleeding. Intra peritoneal drain was inserted and abdomen was closed. His postoperative course was normal except that the peritoneal drain started draining urine.
Operative photograph showing hematoma in descending mesocolon

Operative photograph showing hematoma in left retroperitoneum

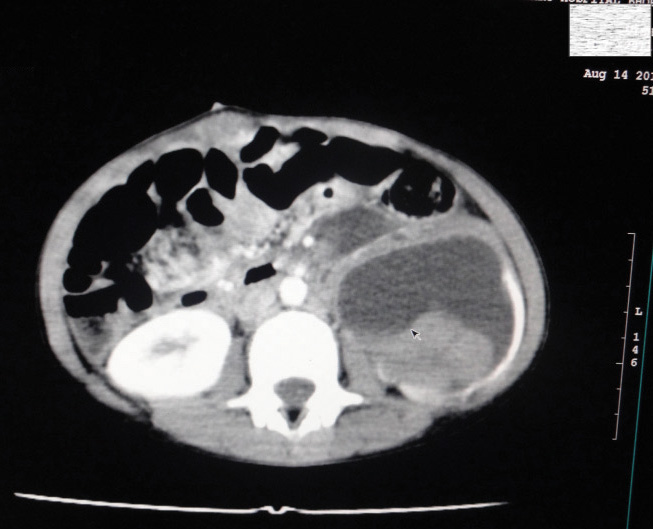
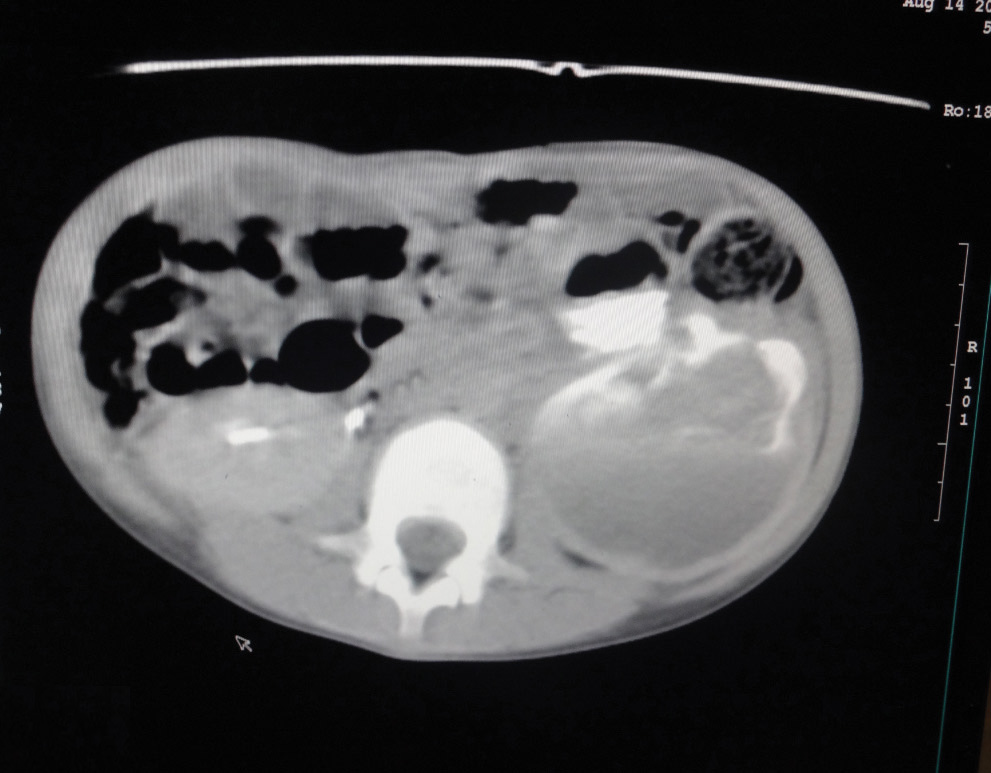
In the post operative period a plain and contrast CT scan of the abdomen was ordered to assess the urinary drainage through peritoneal drain. It revealed left hydronephrotic kidney (5.6 x 6 x 14 cm) due to PUJ obstruction with thinned out renal parenchyma with ballooned out renal pelvis [Table/Fig-2a]. It also showed left perinephric collection [Table/Fig-2b], possibly due to tear in the renal pelvis. Left ureter could not be visualised in its whole course. Right kidney was 4.5 x 4.8 x 10 cm and reported as normal.
CT scan abdomen showing left hydronephrotic, and right normal kidney
CT scan abdomen showing left hydronephrotic kidney with left perinephric collection
The urinary drainage through abdominal drain could not stop on conservative management, and needed nephrostomy. This nephrostomy tube functioned well for two days only thereafter the urine started draining through peritoneal drain again. A nephrostogram was done which showed dye only in renal pelvis and calices and was not going in the ureter [Table/Fig-3]. Nephrostomy revision was done and thereafter he responded well. Peritoneal drain was removed and he was discharged with the nephrostomy tube in place.
Nephrostogram showing dye in renal pelvis and calices, but no dye in ureter

During the management of the child, IVP was also done and showed normal function of the right kidney. Right ureter also well visualized in its whole course, dye in urinary bladder and intra - peritoneal drain also seen [Table/Fig-4]. Left kidney and ureter could not be visualized and reported as hydronephrotic due PUJ obstruction. DTPA scan revealed left hydronephrotic kidney due to PUJ obstruction with good function while right kidney was reported as normal [Table/Fig-5]. Open dismembered Anderson-Hynes pyeloplasty was done four months after trauma. The left kidney was hydronephrotic and PUJ was stenotic [Table/Fig-6]. A trans-anastomotic stent, nephrostomy tube and perinephric drain were inserted, prior to the closure of the wound. His postoperative recovery was excellent and uneventful. A follow-up after a month of pyeloplasty, he was doing well.
IVP showing normal function at right kidney and ureter. Left kidney and ureter not visualized (dye in urinary bladder and intra - peritoneal drain also seen)

DTPA scan showing left kidney obstructed with good function. Right kidney normal function

Operative photograph showing left hydronephrotic kidney, PUJ, and feeding tube in ureter
Discussion
Kidney is the most commonly injured solid organ, and it injured more commonly than liver, spleen or pancreas [1]. Blunt abdominal trauma is responsible for 90% of the pediatric genitourinary tract injury with the kidney being injured in 10 to 20% of the case [1]. Serious renal injuries are often associated with injuries to other organs, and may involve multiple organ and systems [1]. In children, the kidneys are larger relative to the size of the child’s body and positioned lower in the abdomen, and for the same reason making kidneys more vulnerable for injury [1]. For the similar reasons, pre-existing congenital renal anomalies may predispose the children to an increased risk of genitourinary trauma, following blunt trauma of the abdomen and it is 2 to 5 times more prevalent in children with renal injuries than similarly affected adults [1-3]. The reported incidence of pre-existing renal disease or congenital genitourinary anomalies in children sustaining renal trauma varies from 1 to 23% of the case [1,2]. Blunt renal trauma in children resulted mainly from road traffic accidents, fall, sports injuries and assault [1,4].
Gross haematuria is highly indicative of trauma to the genitourinary tract; although it does not necessarily correlates with the severity or grade of the injury, and it suggest major renal injury only in 25% of the cases [3]. Haematuria either gross or microscopic does not exclude the possibility of significant genitourinary trauma [1,3]. Abdominal and renal trauma may be associated with shock. In fact, only 5% of the children with major renal injury have clinical signs of shock and therefore shock or hypotension itself is not a reliable indicator for the severity of renal injury in children [1].
CT scan of the abdomen is the modality of choice in the evaluation of the blunt renal injury in children. CT scan of the abdomen not only identifies the pre-existing renal diseases but also is helpful in grading the renal injury [1,5]. USG of the abdomen may be the primary modality for the evaluation of the cases of blunt injury abdomen and kidney. USG evaluation of the blunt renal trauma depends upon the experience of the person doing it and also has its limitations; but in the places where CT scan is either not available or not assessable easily, USG is the only best available investigation in managing the case of blunt injury of the kidney [4].
Management of blunt renal injury in children depends on many factors and includes; the grade of renal injury, presence or absence of associated renal disease / congenital anomalies, associated other organ or system injury, and the clinical condition of the children [1-4,6,7]. The American association for the surgery of trauma (1989) classify the renal injuries into I to V grades, ranging from the most minor (grade I) to the most complex (grade V), depending upon the severity of the injury [1]. Majority of the blunt renal trauma in children can be successfully managed non-operatively, as almost 85% of the renal injuries are considered to be minor with grade I and II injuries. Major renal injuries are reported to occur in 10 to 15% of the case with major disruption of the renal pedicle occurs only in 5% of the children [1]. The need of immediate surgery in renal trauma depends upon severe grade of renal injury with active bleeding and associated abdominal organs injury.
Children with pre-existing renal disease or congenital anomalies may sustain higher grade of injury and also more likely to require surgery than those without pre-existing abnormalities [3]. The objective for operative treatment of pre-existing renal anomalies must be the salvage of the diseased kidney. Management of blunt renal trauma with pre-existing hydronephrosis due to PUJ obstruction may require nephrostomy and delayed pyeloplasty [2,6,7]. Smith M, et al., reported a 15-year-old boy, who sustained left renal injury due to blunt trauma. CT scan of the abdomen and retrograde urography revealed ruptured left hydronephrotic kidney with a large urinoma. His PUJ obstruction was treated electively [3]. In another case; a 14-year-old girl had undetected, and asymptomatic left PUJ obstruction. She had trivial fall and presented with gross haematuria. Her CT scan and renal isotope scans confirmed left hydronephrosis due to PUJ obstruction. She underwent delayed Anderson-Hynes pyeloplasty for her left PUJ obstruction [6]. Lazer L et al., reported a child with massive haematuria following blunt injury to a HDN kidney due to PUJ obstruction. Author’s managed the child with an initial tube nephrostomy to decompress the injured kidney, followed by reconstruction of the PUJ obstruction [7]. Present case had pre-existing, undiagnosed left hydronephrosis due to PUJ obstruction. He sustained blunt injury abdomen, following fall from motor cycle and admitted with haematuria, shock, and features of peritonitis. USG of the abdomen revealed the hydronephrosis and the CT scan of the abdomen confirmed the same with rupture of the renal pelvis as well. He needed exploratory laparotomy for peritonitis. The left PUJ obstruction and ruptured renal pelvis was successfully managed by tube nephrostomy, and delayed open dismembered Anderson-Hynes pyeloplasty.
Children with pre-existing, occult, renal congenital anomalies may be discovered during the evaluation of the blunt injury of the kidney and abdomen, with or without haematuria. The objective for the management of such a child would be salvage of the diseased kidney and the same may be achieved with staged procedures.
[1]. Brown RL, Garcia VF, Genitourinay tract trauma. In: Grosfeld Jay L, O’Neill JA, Fonkalsrud EW, Coran AG, Caldamone AA (eds)Pediatric Surgery. Chapter18 2006 Vol IEd 6thMosby Inc.:317-36. [Google Scholar]
[2]. Onen A, Kaya M, Cigdem MK, Otçu S, Blunt renal trauma in children with previously undiagnosed pre-existing renal lesions and guidelines for effective initial management of kidney injuryBJU Int 2002 89:936-41. [Google Scholar]
[3]. Smith M, Johnston B, Wessells H, Talner L, Rupture of a ureteropelvic junction - obstructed kidney in a 15-year-old football playerAJR Am J Roentgenol 2003 180:504 [Google Scholar]
[4]. Chirdan LB, Uba AF, Yiltok SJ, Ramyil VM, Paediatric blunt abdominal trauma: challenges of management in a developing countryEur J Pediatr Surg. 2007 17:90-95. [Google Scholar]
[5]. Kawashima A, Sandler CM, Corl FM, West OC, Imaging of renal trauma: a comprehensive reviewRadiographics. 2001 21:557-74. [Google Scholar]
[6]. Mali V, Liu B, Prabhakaran K, Loh D, Blunt renal trauma in occult congenital hydronephrosisSingapore Med J 2005 46:28-30. [Google Scholar]
[7]. Lazar L, Buchumensky V, Erez I, Aronheim M, Conservative treatment of an injured hydronephrotic kidney: the role of percutaneous nephrostomyJ Trauma. 1996 40:304-05. [Google Scholar]