Bleeding Ureter: Endometriosis Mascarading as a Ureteral Malignancy - A Case Report
S.M.L. Prakash Babu1, Puvvada Sandeep2, Amey Pathade3, H K Nagaraj4
1Assistant Professor, Department of Urology, M.S. Ramaiah Medical College and Hospital, MSRIT Post, New BEL Road, Bangalore, India.
2Post Graduate, Department of Urology, M.S. Ramaiah Medical College and Hospital, MSRIT Post, New BEL Road, Bangalore, India.
3Post Graduate, Department of Urology, M.S. Ramaiah Medical College and Hospital, MSRIT Post, New BEL Road, Bangalore, India.
4Professor, Department of Urology, M.S. Ramaiah Medical College and Hospital, MSRIT Post, New BEL Road, Bangalore, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. S.M.L. Prakash Babu, Assistant Professor, Department of Urology, M.S. Ramaiah Medical College and Hospital, Msrit Post, New Bel Road, Bangalore-560054, India. Phone : 9945311618,
E-mail: drnehaprakash@gmail.com
Ureteral endometriosis is a serious localization of disease burden that can lead to urinary tract obstruction, with subsequent hydroureter, hydronephrosis, and potential kidney loss. As the diagnosis is elusive, a heavy clinical suspicion is necessary. Surgical technique to treatment varies, but the goal is to salvage renal function and decrease disease burden. Here, we are presenting a rare case of bleeding ureter in a young lady who had endometriosis of the ureter.
Bleeding ureter, Endometriosis, Hydroureteronephrosis, Ureteral tumour
Case Report
A 35-year-old lady presented with coliky left loin pain since three months, with three episodes of painless haematuria. Menstrual cycles were regular. She has 2 children with younger child of age 6 y. Abdominal examination was apparently normal.
Her systemic and pelvic examination was within normal limits. Biochemical Investigations were within normal limits.
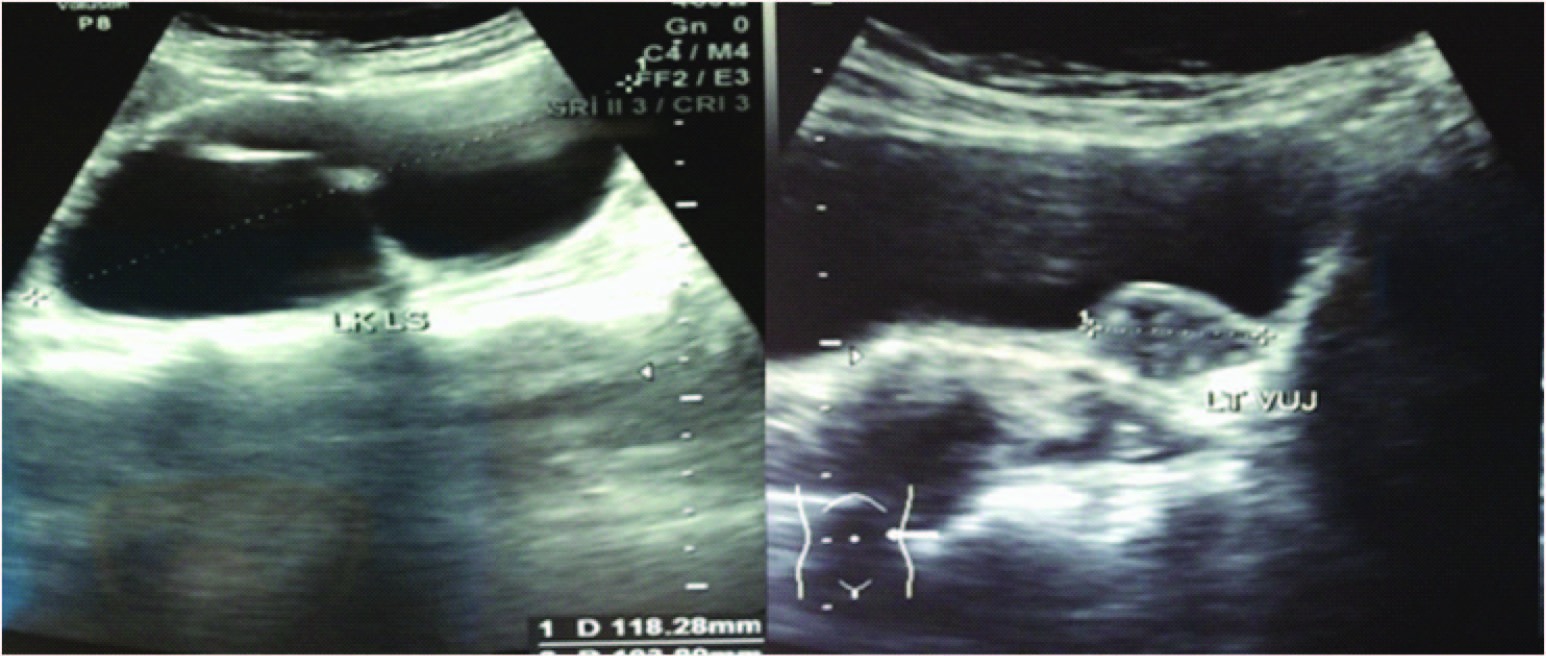
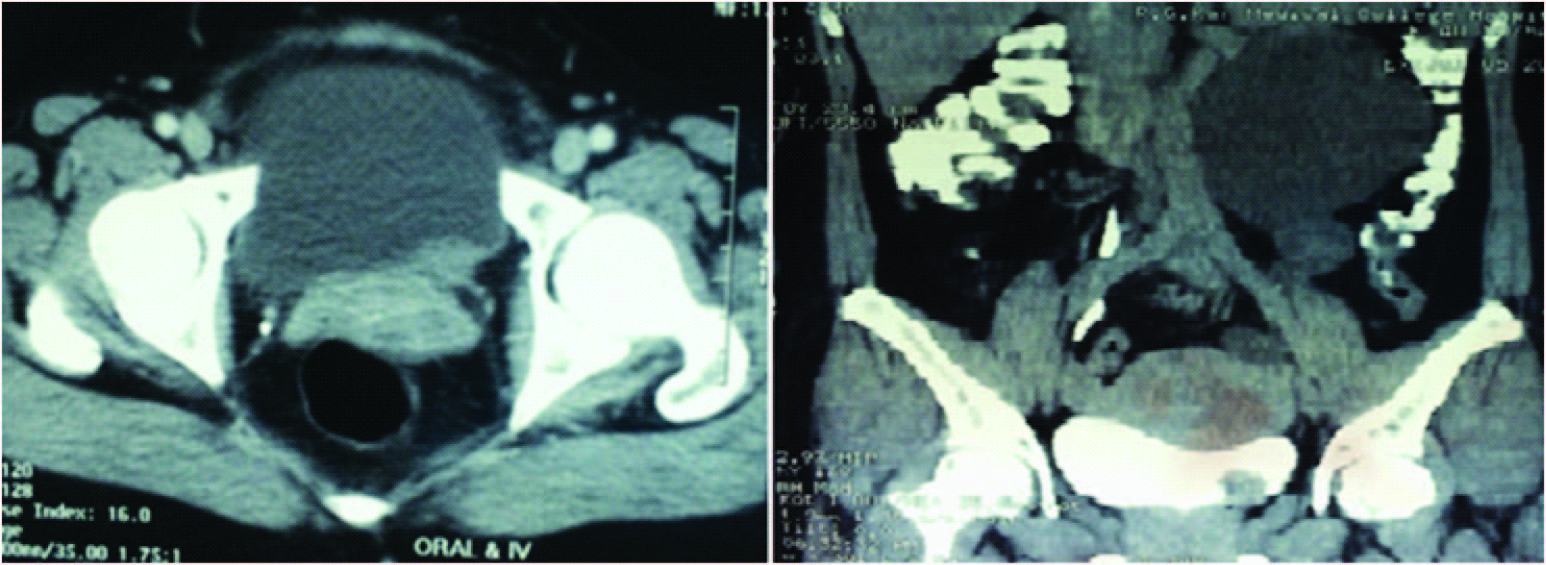
Ultrasound showed a well defined Space Occupying lesion of 19x19 mm Projecting from the Urinary Bladder at Left vesico ureteric junction [Table/Fig-1]. Contrast enhanced CT scan showed enhancing mass at left vesico ureteric junction extending from Ureter into urinary bladder with gross hydroureteronephrosis [Table/Fig-2].
Patient subjected for Cystoscopy which showed no obvious mass / growth found in the bladder. Protuberance seen at the level of left vesico ureteric junction [Table/Fig-3]. Left ureteric orifice visualized, guide wire could not be negotiated into the Left Ureter. The mass was resected, Double J stent placed and specimen sent for histopathology examination. Patients post operative recovery was found to be satisfactory.
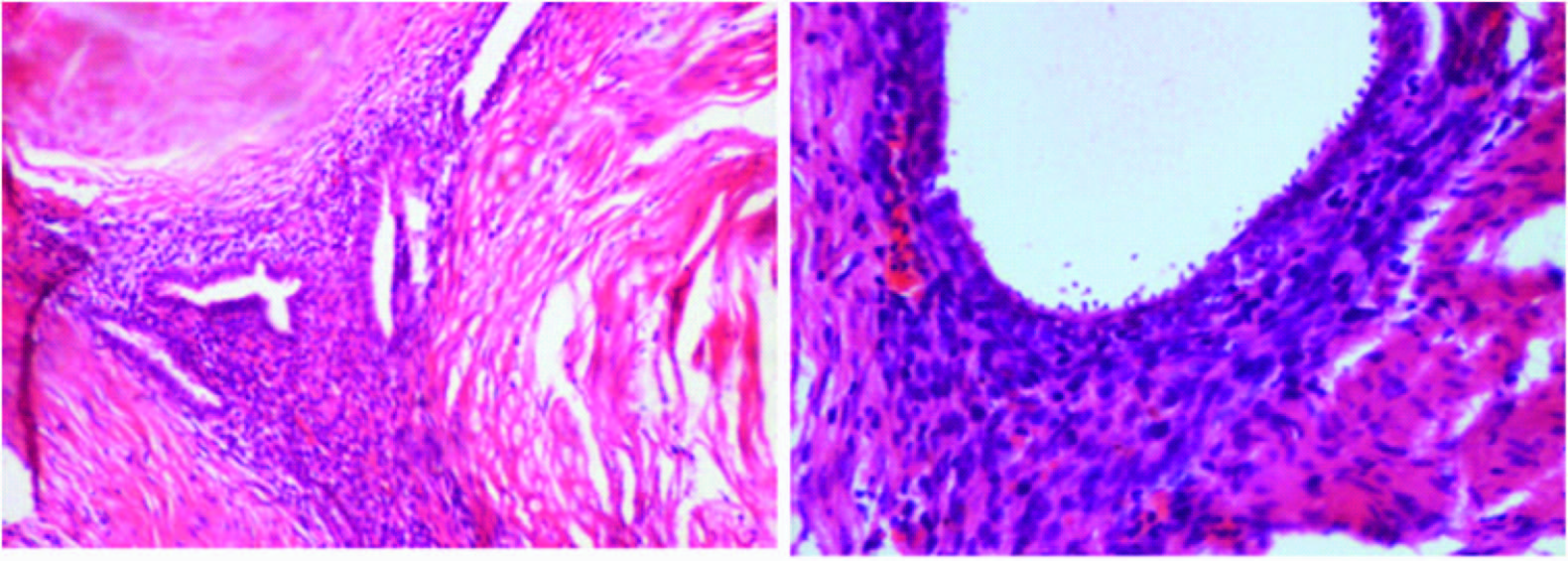
Histopathology examination revealed endometriosis of ureter [Table/Fig-4]. Patient subjected for diagnostic laparoscopy and found no suspicious lesions in the uterus, fallopian tubes and ovaries.
Double J stent removed after six weeks and diagnostic ureterorenoscopy was performed which showed no recurrence of growth.
Discussion
A benign disease such as endometrosis may have an aggressive clinical behaviour. It occurs in 15-20% women of childbearing age. Organs usually affected are ovaries, uterosacral ligaments, fallopian tubes, rectum and cervico-vaginal region [1]. Urinary tract involvement is uncommon and estimated to be about 1% [1] of which vesical involvement is the most common of them[2,3]. Usually the women of the 3rd or 4th decade of age are affected with a peak incidence in between 30-35 y [2]. Chronic pelvic pain with urinary urgency, frequency, dysuria, dysparenuea with or without cyclical haematuria are the usual clinical symptoms. Ureteric involvement may present with backpressure changes in the kidney or anuria with bilateral ureteric involvement [1]. Abdominal pain and haematuria were the presenting complaints, which could suggest urinary tract infection or stone disease, thereby making endometriosis a rare diagnosis in this case. Diagnosis of genitourinary endometriosis relies heavily on clinical suspicion.
The best treatment approach for ureteral endometriosis is still contentious. Laparoscopy is the gold standard for definitive diagnosis and surgical treatment of endometriosis. Careful destruction of all endometriotic implants is important to prevent recurrence [4,5]. Surgical excision of all endometriosis has been proven to be the most effective method for symptom relief, and advanced laparoscopy has replaced laparotomy as the mode of choice [4,6,7].
As in our case, investigative procedures play a key role in diagnosis. Abdominal sonography and CT scans were suggestive of hydroureteronephrosis secondary to an obstructive pathology. In this scenario, the most common cause would be presence of a stone or a stricture. On the other hand, cystoscopy ruled out these two most probable diagnoses and detected a mass. Histopathology revealed the mass to be endometriosis. This case shows that endometriosis can mimic other disease entities and hence the diagnosis relies on heavy clinical suspicion with the help of diagnostic aids. Endometriosis is a common gynaecological entity but its occurrence in canal of Nuck is rare [8].
A well defined SOL of 19x19 mm projecting from the urinary bladder at Lt. UVJ
Mass at lt. UVJ extending from ureter into urinary bladder with gross hydroureteronephrosis
Cystoscopy showing protuberance at the level of Left vesico ureteric junction
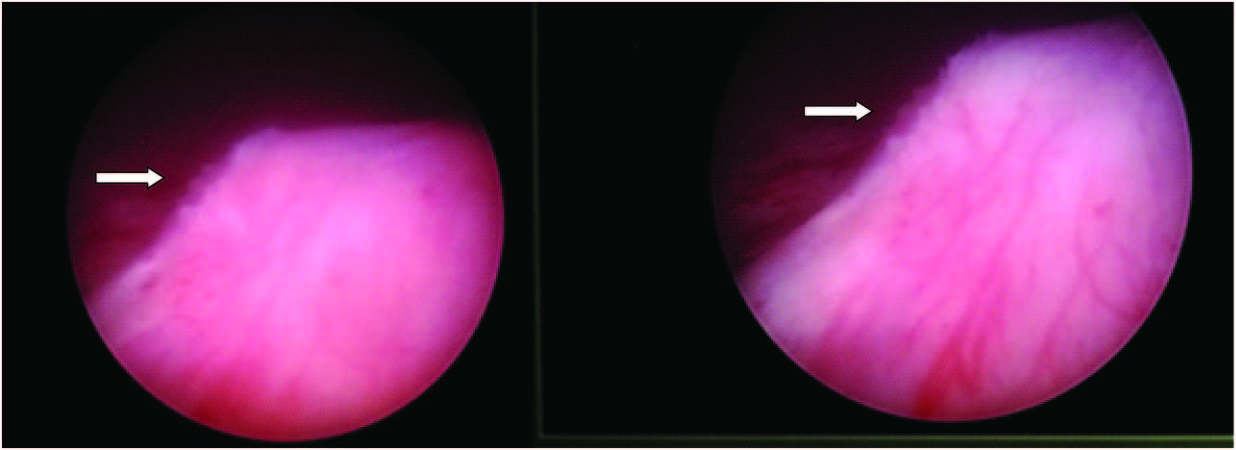
Photo microgragh showing focus of endometrial glands and stroma, surrounding fibrocollagenous tissue is seen[ H & E 10X], endometrial glands lined by cuboidal cells, and surrounding stroma [H&E 40X]
Conclusion
Ureteric endometriosis is a progressive disease, which leads to acute deterioration in renal function. The surgical urological treatment can have good results in terms of both patient compliance and prognosis. Isolated involvement of the ureter is a rare presentation itself.
[1]. JG Moore, LT Hibbard, WA Growdon, BS Schifrin, Urinary tract endometriosis: Enigmas in diagnosis and managementAm J Obstet Gynaecol 1979 134:162-72. [Google Scholar]
[2]. SP Lucero, HA Wise, G Kirsh, K Devoe, ML Hess, N Kandawalla, Ureteric obstruction secondary to endometriosis. Report of three cases with review of literatureBr J Urol 1988 61:201-04. [Google Scholar]
[3]. GJ Garcia, CJ Extramiana, CJ Esteban, Vesical endometriosis after caesarian section: diagnistico-tharapeutic aspectsActaUrolEsp 1997 21:785-88. [Google Scholar]
[4]. C Nezhat, F Nezhat, C Nezhat, Endometriosis: Ancient disease, ancient treatmentsFertSteril 2012 [Google Scholar]
[5]. CR Nezhat, When will video-assisted and robotic-assisted endoscopy replace almost all open surgeries?J Minim Invasive Gynecol 2012 19:238-438. [Google Scholar]
[6]. WE Kelley, The evolution of laparoscopy and the revolution in surgery in the decade of the 1990sJSLS 2008 12:351-57. [Google Scholar]
[7]. C Nezhat, F Nezhat, Operative laparoscopy (minimally invasive surgery): state of the artJ Gynecol Surg 1992 8:111-41. [Google Scholar]
[8]. Albal Manisha, Zaki B Mohammad , Ansari Irfan, Endometriosis in Cyst of Nuck’s canal: A Rare PresentationJournal of Case Reports 2014 8(1):88-90. [Google Scholar]